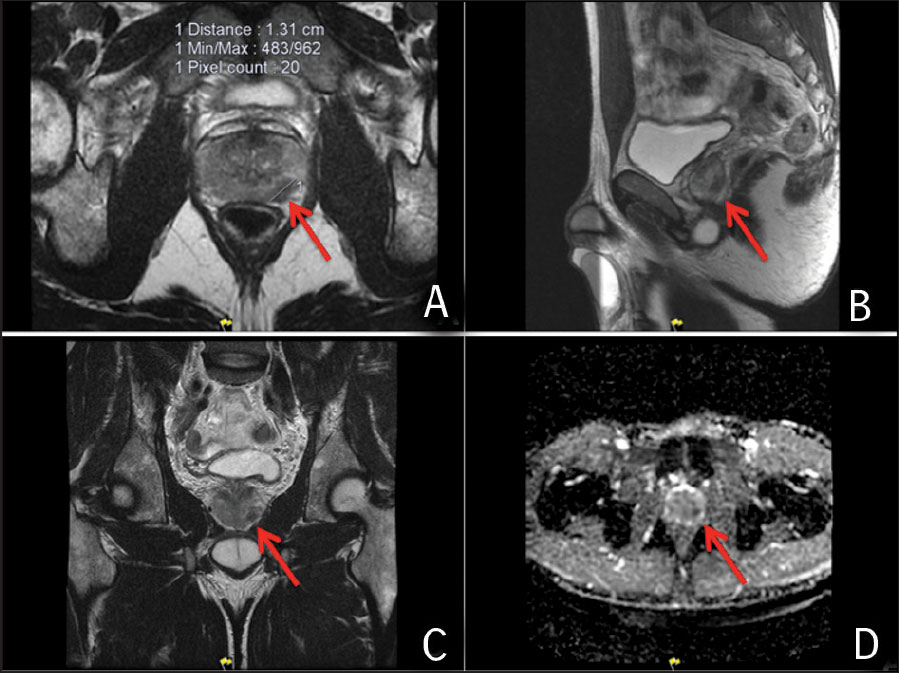
A 51-year-old man who attends his GP for an annual check up, noticed a rise in his prostate-specific antigen (PSA) from 2.49ug/l to 3.29ug/l over a 12 month period and attends for assessment in the rapid access prostate clinic. He denies any urinary symptoms and rectal examination is normal. The patient wishes to undergo MRI, and four still images are shown in Figure 1. The key here is that the abnormality is present in all sequences of the MR and also displays abnormalities on the diffusion weighted sequence, highly suspicious for an underlying prostatic malignancy.
Figure 1. Image A, B and C demonstrate a lesion in the left apex of the prostate with diffusion anomalies present in image D(click to enlarge)
The patient undergoes a standard 12 core transrectal guided (TRUS) prostate biopsy and additional cores targeted at the abnormality in the left apex. All cores from the left side of prostate show Gleason 4+4 prostate cancer (WHO Grade 4) involving from 5% to 40% of each core. Neither the MRI or bone scan suggested any extra-prostatic disease and the patient elected to undergo a radical prostatectomy with bilateral pelvic lymph node dissection with preservation of the right sided nerve bundle. The surgical pathology report confirms a fully resected lesion with negative margins and nodes. He made a good functional recovery and has remained free of biochemical recurrence for 12 months.
Teaching point
Young men should have a low PSA. Those aged 45-50 years whose PSA is >1.5ug/l need to have their PSA monitored at least every two years whereas those with a PSA of <1.5ug/l are very unlikely to develop clinically significant prostate cancer during their lifetime.1 A rise above 3ug/l in a man aged from 50-60 years requires referral through the rapid access prostate service (NCCP Guidelines – PSA thresholds for referral 2016).
Case 2
A 74-year-old man in otherwise good health attended with a 12-month history of lower urinary tract symptoms consistent with benign prostatic hyperplasia (BPH). He had a suspected recent UTI. His GP had checked his PSA and it returned at 14ug/l. Digital rectal exam (DRE) had shown an enlarged benign-feeling gland. The patient underwent cystoscopy and urodynamics and was commenced on oral tamsulosin for BPH. He was asked to return four months later with a repeat PSA as the recent UTI had likely affected the earlier PSA reading.
On review, the patient’s urinary symptoms had not responded and his PSA was now 74ug/l. A bone scan and CT demonstrated diffuse metastatic disease to bone and soft tissue. Prostate biopsy showed high grade Gleason 4+5 prostate cancer (WHO Grade 5). He was commenced on hormonal therapy and referred to medical oncology for consideration for chemotherapy and was commenced on docetaxel every three weeks. His imaging showed progressive disease and he elected to take part in a clinical trial and received abiraterone and prednisolone. He responded initially and improved with a fall in his PSA.
While holidaying in Ireland five months later he experienced two significant episodes of blood per rectum. A subsequent colonscopy and CT confirmed a large pelvic mass surrounding the rectum and biopsy demonstrated neuroendocrine differentiation of the prostate cancer. Staging scans demonstrate progressive disease and patient continues with palliative care.
Teaching point
Neuroendocrine differentiation of a prostate cancer can occur following treatment and unfortunately runs an aggressive course.
Case 3
A 67-year-old man presents with recent dysuria and a PSA of 9.9ug/l through his GP. A repeat PSA six weeks later returns at 13.9ug/l. On assessment his DRE demonstrates a swollen tender prostate and he is treated as a prostatitis with oral ciprofloxacin and advised to repeat the PSA in 12 weeks. The repeat PSA has now risen to 18ug/l. The patient agrees to undergo a 12 core TRUS guided biopsy. This identifies five cores of prostate cancer with two cores containing Gleason 4+5 prostate cancer (WHO Grade 5). Staging MRI and bone scan do not identify any metastases and the man is offered either surgery (radical prostatectomy) or radiotherapy and hormonal therapy.
He is aware that there is a high likelihood of adjuvant radiotherapy treatment. He decides to proceed with surgery and undergoes a radical prostatectomy with bilateral pelvic lymph node dissection. The surgical pathology confirms Gleason 9 prostate adenocarcinoma with invasion of the seminal vesicle and a single lymph node with a metastatic deposit. His urinary control returns within six weeks and he has opted for a penile implant to treat his impotence. On review 18 months after the surgery he remains biochemically free of recurrent disease.
Teaching point
Aggressive prostate cancer can present similar to prostatitis. I have certainly seen three or more cases present with prostatitis recently which were later diagnosed with high grade disease. Ensure PSA follow up once the acute symptoms settle. This man’s high risk pathology features certainly put him at risk for recurrence. He can opt for adjuvant or salvage radiotherapy but as he remains biochemically free he does want radiotherapy at this time and will be treated if his PSA recurs. Post-prostatectomy radiotherapy can lead to bladder neck contracture or radiation cystitis.
Case 4
A 42-year-old Man is referred to the rapid access prostate clinic with a single PSA reading of 6.2ug/l. He denies any urinary symptoms. His DRE demonstrates a benign smooth prostate and undergoes a TRUS guided prostate biopsy. No cancer is identified and the patient attends with a repeat PSA that is now risen to 8ug/l. Before proceeding to a further biopsy, an MRI prostate is obtained, in keeping with NCCP guidelines.2
The image in Figure 2 demonstrates a large anterior prostate lesion with abnormalities on the diffusion weighted imaging, strongly suggestive of an underlying cancer. A targeted prostate biopsy of this anterior prostate cancer revealed Gleason 3+4 prostate cancer involving 60% of two cores. Staging scans did not demonstrate any disease beyond the prostate and the patient underwent a nerve sparing radical prostatectomy. He made an excellent functional recovery and has remained free of biochemical recurrence.
Figure 2. MRI images demonstrate a lesion on the anterior surface of the prostate in image A, with diffusion abnormalities in image B(click to enlarge)
Teaching point
Where the PSA does not normalise after a prostate biopsy, an MRI must be obtained before proceeding to another biopsy. A repeat standard biopsy would have missed the anterior lesion that was targeted in this case.
Case 5
A 91-year-old man was referred by his GP with an elevated PSA. The patient was in exceptionally good health and played two to three rounds of golf a week. The patient had noted he was getting up more often at night. The initial PSA was 16.3ug/l and on repeat returned at 19ug/l. On DRE a 1cm nodule was palpable at the left apex and he agreed to have a TRUS prostate biopsy. A Gleason 4+5 adenocarcinoma was identified.
Subsequent staging scans were normal and the man elected to undergo hormonal treatment with radiotherapy. He has recovered very well and is now back playing golf.
Teaching point
Any man with a 10 year life expectancy should be considered for prostate cancer testing and possible radical therapy.3 This man is very likely to survive to over 100 years and has an excellent quality of life. Had he not had his PSA checked, undergone a biopsy and treatment, he would have developed metastases within one to two years.
References
Lilja H, Ulmert D, Björk T et al. Long-term prediction of prostate cancer up to 25 years before diagnosis of prostate cancer using prostate kallikreins measured at age 44 to 50 years. J Clin Oncol 2007 (Feb); 1;25(4): 431-6
Fütterer JJ, Briganti A, De Visschere P et al. Can clinically significant prostate cancer be detected with multiparametric magnetic resonance imaging? A systematic review of the literature. Eur Urol 2015 (Dec); 68(6): 1045-53
Murphy DG, Ahlering T, Catalona WJ et al. The Melbourne consensus statement on the early detection of prostate cancer. BJU Int 2014 (Feb); 113(2): 186-8.
 Figure 1. Image A, B and C demonstrate a lesion in the left apex of the prostate with diffusion anomalies present in image D(click to enlarge)
Figure 1. Image A, B and C demonstrate a lesion in the left apex of the prostate with diffusion anomalies present in image D(click to enlarge)