Genetic predisposition, second-hand smoking and occupational exposure are some of the lung cancer risk factors explored by Dr Judith Lyons and Dr Finbarr O’Connell
Dr Judith Lyons, SpR in Respiratory Medicine, St James's Hospital, Dublin and Dr Finbarr O'Connell, Consultant Respiratory Physician, St James's Hospital, Dublin
Lung cancer is the leading cause of cancer-related death in Ireland. It is the third commonest cancer excluding non-melanoma skin cancers. In Ireland the incidence of lung cancer has been rising. However, the rate of increase is more rapid in women as a result of increased smoking prevalence. In 2011 it became the leading cause of cancer-related death in women in Ireland, overtaking breast cancer.1
The proportion of lung cancer which is adenocarcinoma is also increasing while that of squamous cell carcinoma is decreasing in men. In women there has been an increase in the incidence of both squamous and adenocarcinoma. The change in the prominent histological pattern from squamous to adenocarcinoma is observed worldwide and is thought to reflect the more widespread use of filters and increase in nitrate levels in the tobacco resulting in the carcinogens being deposited more distally in the airways.2,3
Lung cancer in non-smokers
While it is well established that tobacco smoking is a major cause of lung cancer a significant proportion occurs in non-smokers.4 It is estimated that 10-15% of lung cancer occurs in never-smokers and the trend is increasing in developed countries.
Lung cancer in never-smokers, as a separate entity from that which is smoking related, is one of the leading causes of cancer-related death. It ranked as the sixth most common cause of cancer death in the US in 2008.4 The incidence of lung cancer in never-smokers is raised significantly in Asian countries such as Japan where in 2004 never-smokers were 38.3% of total lung cancers.5
In St James’s Hospital, of the 583 patients diagnosed with lung cancer in 2011, 7.4% were never-smokers (see Figure 1 and 2), a percentage which has remained relatively stable since 2007. Lung cancer which is not associated with smoking differs from that which is smoking related in its molecular profile, prognosis and response to targeted therapy.
Figure 1(click to enlarge)
Figure 2(click to enlarge)
Risk factors
The aetiology of lung cancer in never-smokers is unclear. However, a number of risk factors have been identified. In the US it is estimated that half of the cases are attributable to indoor radon in homes or to exposure to second hand smoke (see Table 1).
Radon is a respiratory carcinogen which is a recognised contaminant of indoor air. The alpha particle emissions from inhaled radon progeny are responsible for its carcinogenesis.6 Numerous studies on miners who were exposed to increased levels of radon7 and on the general public by measuring radon levels in residences show a significant association between lung cancer and radon independent of smoking status.8,9
Secondhand smoking is a well-established risk factor for the development of lung cancer in never smokers. Numerous studies have repeatedly demonstrated the association.10,11 The clean indoor air policies introduced in Ireland should help to reduce the exposure of non-smokers to the harmful effects of cigarettes.
Occupational exposure in particular to paints and paint thinners, wielding equipment, smoke soot or exhaust fumes has been associated with lung cancer in never smokers.12
A history of any previous lung disease is associated with an increased risk of lung cancer including asthma, chronic bronchitis, emphysema, pulmonary fibrosis and pneumonia.13 In particular an association has been shown between a history of pulmonary tuberculosis and the development of lung cancer.14
Indoor air pollution such as that caused by the burning of coal or biomass for heating and cooking in poorly ventilated areas has been associated with an increased lung cancer risk.15 Approximately 50% of the world’s population mostly in developing countries are dependent on biomass fuels for heating and cooking.
Genetic predisposition to the development of lung cancer has been studied. A meta-analysis of published literature performed in 2005 found that there was a twofold increase in risk associated with having a family history of lung cancer in a first-degree relative. Risk was greatest in those whose relatives were diagnosed at an early age and in those with a greater number of affected relatives. This result may have been confounded by shared exposure to tobacco smoke.
However, pooling of data in never-smokers found an increased risk associated with having a first-degree relative with lung cancer that was statistically significant suggesting a genetic or environmental component.16
Radiation such as that used in the treatment of Hodgkin lymphoma or breast cancer is associated with an increased risk of lung cancer. However, this risk is more pronounced among smokers.17,18
(click to enlarge)
Natural history and prognosis
Lung cancer in never-smokers has been shown to occur at a younger age than in smokers. It affects women with a greater frequency than men. The histological type is predominantly adenocarcinoma with a small proportion of squamous and small cell carcinomas.
The never-smoking status in addition to female gender and adenocarcinoma have all been shown to be associated with improved post-operative survival in lung cancer. In never-smokers, cancer-specific survival was also found to be improved.
Tumours in never-smokers tend to be diagnosed at a smaller size than in that of smokers, suggesting that the cancer may grow more slowly and metastasise later.19 Studies also found that in patients with advanced NSCLC at the time of diagnosis, the prognosis was significantly better for never-smokers compared with that of smokers.20
Molecular targeted treatment in never-smokers
In clinical trials on patients with the tyrosine kinase inhibitors gefitinib and erlotinib, a markedly better clinical outcome was consistently noted in never-smokers.
Further studies showed that the response was more marked in patients of east Asian ancestry and in adenocarcinomas.21 This prompted much research in the field of lung cancer in never-smokers. In 2004 it was discovered that mutations in the tyrosine kinase domain of the epidermal growth factor receptor (EGFR) was associated with a response to tyrosine kinase inhibitors.22,23
Activating mutations in EGFR were found to be more common in never-smokers, in women, in adenocarcinoma and in patients of east Asian origin explaining why tyrosine kinase inhibitors were more effective in this patient group.
Approximately half of patients who are never-smokers with NSCLC will have an EGFR mutation and will benefit from targeted therapy with tyrosine kinase inhibitors.
In 2007 another mutation was discovered in lung cancer patients. This mutation was in the echinoderm micro-tubule-associated protein-like 4 and the anaplastic lymphoma kinase (EML4- ALK) fusion gene.24 It was found in approximately 5% of patients with NSCLC. EML4-ALK is more common in adenocarcinoma and never or light smokers. It is also associated with a younger age of onset.25
Targeted therapy with crizotinib, an ALK/MET inhibitor, has shown good response in patients with an EML4-ALK mutation.26
Summary
While smoking is the most common risk factor associated with lung cancer, a significant percentage occurs in never-smokers. Radon, second-hand smoking, occupational exposure, indoor air pollution and genetic predisposition are risk factors for the development of lung cancer in non-smokers.
Lung cancer not related to smoking has different clinical, pathological and molecular findings. It is commonly adenocarcinoma. It occurs more frequently in women, particularly women of Asian ancestry. It tends to occur at a younger age and have a better prognosis than lung cancer in smokers.
Mutations in EGFR and EML4-ALK occur more commonly in never-smokers or light smokers enabling targeted therapy with tyrosine kinase inhibitors and crizotinib respectively.
References
The National Cancer Registry Ireland, 2009
Hoffmann D, Hoffmann I. The changing cigarette, 1959-1995 Journal of Toxicology and Environmental Health 1997; 50: 307-64
Wynder EL, Muscat JE. The changing epidemiology of smoking and lung cancer histology. Environ Health Perspect 1995; 103 (Suppl 8): 143-148
Jamal A, Siegel R, Ward E et al. Cancer Statistics, 2008 CA:58: 71096
Sawabata N, Fujii Y, Asamura H et al. Analysis of lung cancer registry cases resected in 2004 Japanese Joint Committee for Lung Cancer Registration. J Jpn Assoc Chest Surgery 25: 107-123
National Research Council N. (NRC). Committee on Health Risks and Exposure to Radon, Board on Radiation Effects Research and Commission on Life Sciences Health Effects of exposure to Radon. Washington DC: National Academy Press 1999
Samet JM, Kutvirt DM, Waxweiler RJ, Key CR. Uranium mining and lung cancer in Navajo men. N Engl J Med 1984; 310: 1481-1484
Krewski D, Lubin JH, Zielinski JM et al. A combined analysis of North American casr-control studies of residential radon and lung cancer. J Toxicol Environ Health A 2006; 69(7): 533-597
Darby S, Hill D, Auvinen A, Barros –Dios JM et al. Residential radon and lung cancer – Detailed results of a collaborative analysis of individual data on 7148 persons with lung cancer and 14,208 persons without lung cancer from 13 epidemiologic studies in Europe. Scand J Work Environ Health 2006; 32 suppl 1: 1-83
Zong L, Goldberg MS, Parent M et al. Exposure to environmental tobacco smoke and the risk of lung cancer: a meta analysis . Lung Cancer 2000; 27: 3-18
Brennan P, Buffler PA, Reynolds P et al. Secondhand smoke exposure in adulthood and risk of lung cancer among never smokers:a pooled analysis of two large studies. Int J cancer 2004; 109: 125-131
Brenner Dr, Hung RJ, Tsao MS et al. Lung cancer risk in never smokers: a population based case control study of epidemiologic risk factors. BMC Cancer 2010; 10: 285
Wu AH, Fontham ETH, Reynolds P et al. Previous lung disease and lung cancer among lifetime non-smoking women in the United States. Am J Epidemiol 1995; 141:1023-1032
Liang HY, Li XL, Yu XS et al. Facts and fiction of the relationship between preexisting tuberculosis and lung cancer risk: a systematic review. Int J Cancer 2009; 125: 2936-2944
International Agency for research on cancer. Household use of solid fuels and high temperature frying vol 95. Lyon, France. 2008 IARC Monographs on the evaluation of carcinogenic risks to humans.
A Matakidou, T Eisen, RS Houlston et al. Systematic review of the relationship between family history and lung cancer risk. Br J Cancer 2005; 93: 825-833
Prochazka M, Hall P, Gagliardi G et al. Ionizing radiation and tobacco use increased the risk of a subsequent lung carcinoma in women with breast cancer: case only design J Clin Oncol 2005; 23(30): 7467-7474
vanLeeuwen FE, Klokman WJ, Stovall M et al. J Natl cancer Inst 1995; 87(20): 1530-1537
Yano T, Miura N, Takenata et al. Never-smoking non small cell lung cancer as a separate entity- the clinic-pathologic features and survival. Cancer 2008; 113: 1012-1018
Toh CK, Gao F, Lim WT et al. Never smokers with lung cancer. Epidemiologic ecidence of a distinct disease entity. J Clin Oncol 2006; 24: 2245-2251
Miller VA, Kris MG, Shah N et al . Bronchioloalveolar pathologic subtype and smoking history predict sensitivity to gefitinib in advanced non small cell lung cancer J Clin Oncol 2004; 22: 1103-9.
Lynch TJ, Bell DW, Sordella R et al, Activating mutations in epidermal growth factor receptor underlying responsiveness of non small cell lung cancer to gefitinib N Engl JMed 2004; 350: 2129-39
Pao W, Miller V, Zakowski M et al . EGF receptor gene mutations Ware common in lung cancers from “never smokers” and are associated with sensitivity of tumors to gefitinib and erlotinib. Proc Natl Acad Sci USA 2004; 101: 13306-13311
Soda M, Choi YL, Enomoto M et al. Identification of the transforming EML4-ALK fusion gene in non small cell lung cancer. Nature 2007; 448: 561-566
Shaw AT, Yeap BY, Mino-kenudson M et al. Clinical features and outcomes of patients with non small cell lung cancer who harbor EML4-ALK. J Clin Oncol 2009; 27: 4247-4253
Crino L, Kim D, Riely GJ et al. Initial phase II results with crizotinib in advanced ALK- Positive non-small cell lung cancer (NSCLC);PROFILE 1005. J clin Oncol 2011; 29 Suppl: Abstr 7514
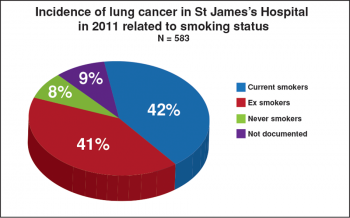 Figure 1(click to enlarge)
Figure 1(click to enlarge)

