Lung cancer management in the era of precision medicine
Important advances in lung cancer biology have led to personalised treatment based on targeting specific gene mutations and signalling pathways
Prof Seamus O'Reilly, Consultant Medical Oncologist, Cork University Hospital, Cork and Dr Colum Dennehy, Medical Oncology Specialist Registrar, Mercy University Hospial, Cork
Lung cancer is a disease with significant morbidity and mortality; in 2012 there were an estimated 1.82 million new diagnoses contributing to almost 1.6 million deaths worldwide. Non-small cell lung cancer (NSCLC) diagnoses comprise approximately 85% of all lung cancer diagnoses, which is further classified into broadly three distinct histological subtypes: adenocarcinoma, squamous cell carcinoma and large cell carcinoma (LCC), with adenocarcinoma comprising the majority of all new lung cancer diagnoses.1
The practice of precision medicine is incumbent on optimal tumour sampling, accurate tumour testing, and informed application of results to patient care. The management of lung adenocarcinomas now requires multiple molecular tests, including epidermal growth factor receptor (EGFR) gene, anaplastic lymphoma kinase (ALK), programmed death-ligand 1 (PD-L1) analysis and extended panelling if there is sufficient tissue at baseline to define the optimal treatment strategy.
The role of EGFR in NSCLC
Important advances in lung cancer biology have led to personalised treatment based on targeting specific gene mutations and signalling pathways. Discovery of somatic mutations within the kinase domain of the EGFR has led in an era of targeted therapies in lung cancer. EGFR mutations occur in approximately 10-30% of the NSCLC population globally with an incidence of approximately 10% in the Caucasian population.
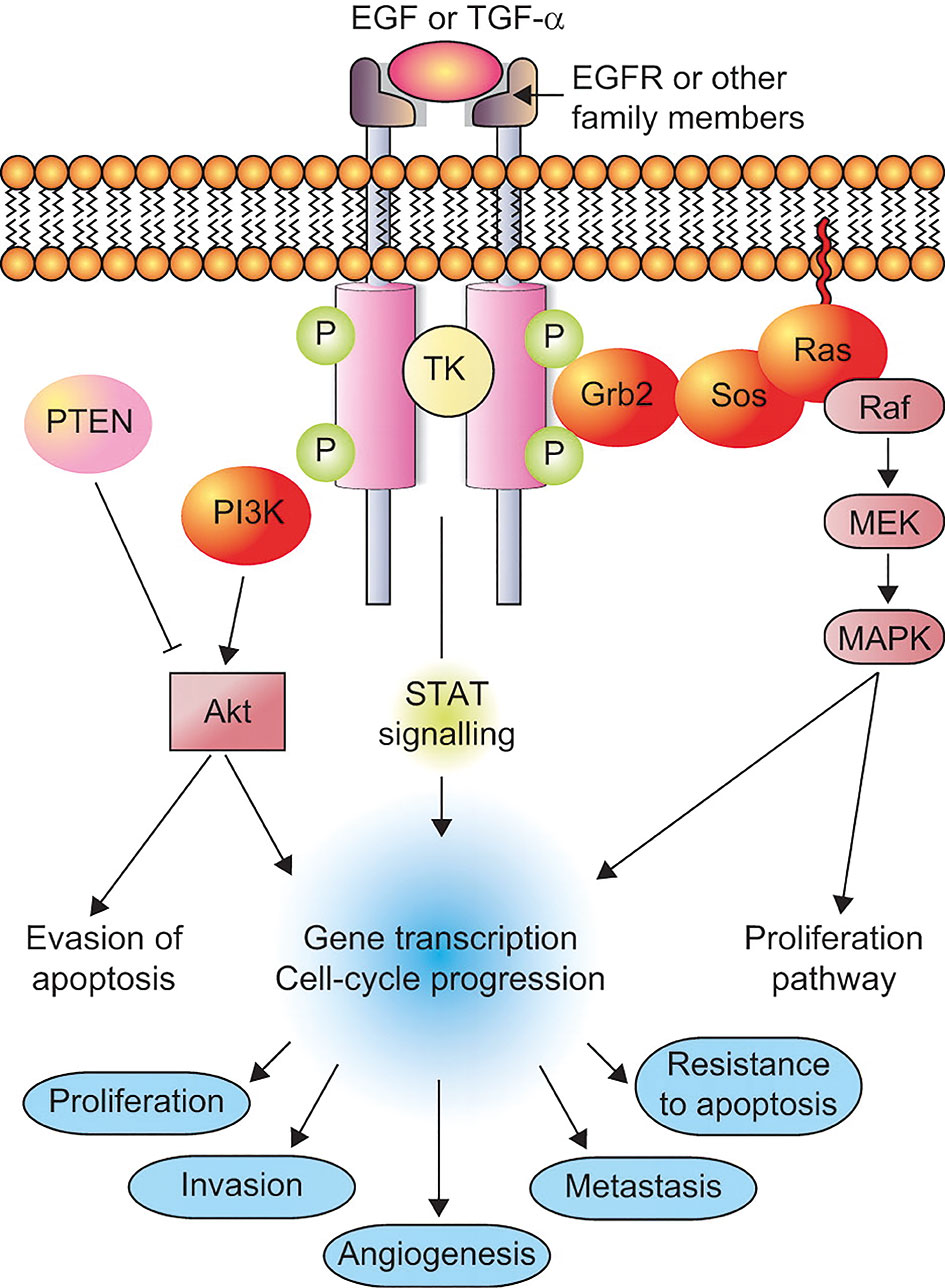
From an Irish context, in the HSE South 8% (27/334) of patients were found to have sensitising EGFR mutations.2,3,4 The function of the receptor is to regulate both cell proliferation and apoptosis via signal transduction pathways, therefore dysregulation leads to increased intracellular pathways activity, via tyrosine kinase autophosphorylation, resulting in directly or indirectly, cell proliferation, angiogenesis, invasion and metastasis (see Figure 1).
Figure 1. Epidermal growth factor receptor (EGFR) pathway(click to enlarge)
Tyrosine kinase domain mutations
The mutations target critical regions of the tyrosine kinase domain in exons 18-21 associated with downstream signalling and are of several types, including deletions, insertions and activating point mutations. The majority of mutations in exon 21 are point mutations, primarily L858R, whereas mutations in exon 19 consist of almost entirely in-frame deletions.
First-generation (gefitinib and erlotinib), second-generation (afatinib) and since June 2018 third-generation (osimertinib) EGFR tyrosine kinase inhibitors (TKIs) are now standard of care for the first-line management of patients with advanced NSCLC harbouring EGFR-mutations, although osimertinib is not yet reimbursed in Ireland.
Gefitinib and erlotinib are reversible EGFR TKIs, whereas afatinib is an irreversible ErbB family blocker that blocks signalling from ErbB family receptors by binding covalently to proteins of the ErbB receptor network and irreversibly abrogates signalling. Treatment with EGFR TKIs in this selective patient population has extended progression-free survival (PFS) relative to chemotherapy with a median PFS of 11.0 months with EGFR TKIs gefitinib and erlotinib versus 5.6 months with chemotherapy. Similar results were demonstrated when real-world data was examined in the HSE South with an objective response rate among these patients of 74% and PFS of 13 months (range 7 to 35 months).2,3,4,5,6
Unfortunately, although the above agents improve PFS, resistance almost invariably develops within one year. Mechanisms of acquired resistance to EGFR TKIs can be broadly classified into four categories:
Secondary resistant EGFR mutations (ie. point T790M mutation in exon 20)
Activation of bypass pathways
Activation of downstream pathways
Histologic transformation.
Additional biopsies should be performed at the time of progression in patients treated with TKIs, to elucidate the common mechanisms of acquired resistance and additional identifiable mutations to define the continued use of molecularly targeted therapy.
Osimertinib is an irreversible EGFR TKI inhibitor that is selective for both EGFR TKI sensitising and T790M resistance mutations with activity in the central nervous system in patients with NSCLC.7,8 It has shown efficacy in both patients previously treated with TKIs with T790M mutations and as first-line in untreated EGFR-mutated advanced NSCLC. In the second-line setting median duration of PFS was significantly longer with osimertinib than with platinum therapy plus pemetrexed (10.1 months versus 4.4 months).
In the first-line setting, median progression-free survival was shown to be significantly longer with osimertinib than with standard EGFR TKIs – 18.9 months (CI, 15.2 to 21.4) versus 10.2 months (CI, 9.6 to 11.1) respectfully with similar overall response rates (80% versus 76%).7,8
Tissue sampling/serum analysis ‘liquid biopsy’
Typical tissue sampling uses bronchoscopy or image guidance to obtain a sample of tumour tissue, however this is not always feasible due to time constraints, available resources and patient preference. Liquid biopsy allows clinicians to determine patients suitable for EGFR-targeted therapy by analysis of circulating-free tumour DNA (cfDNA) in peripheral blood samples and may replace additional tissue biopsy in the future as it is less time and resource consuming.
Several studies have shown that mutations detected in plasma can be highly concordant (usually 60-90%) with those detected in tumour tissue in NSCLC patients, however no clear method of assessment has been deemed superior, therefore there is no established gold-standard test against which to evaluate them.9,10,11
Explanations for the discordance between tissue and serum sampling may be related to the tissue sampling not being fully reflective of the heterogeneity of patients’ lung tumours.
The two most sensitive techniques are targeted next-generation sequencing (NGS) and emulsion polymerase chain reaction (PCR). PCR is best suited for identifying known hotspot mutations. One challenge with high-sensitivity genotyping assays such as NGS is the potential to detect low variant allele frequency (VAF) with uncertain clinical significance.
Liquid biopsy is currently not optimised for comprehensive tumour sequencing and characterisation because it has become clinically relevant only in the past few years and further research is needed to improve specificity, sensitivity and positive predicative value.12
Side effects/toxicity
Our treatment decisions as clinicians are based on assessing differences in effectiveness (PFS/overall survival) of each of the above TKIs against the differences in treatment-related toxicities.
A recent meta-analysis demonstrated that among the EGFR TKI-specific toxicities of all grades, diarrhoea (53.3%) and rash (66.5%) were the most frequent, affecting more than half of patients.13
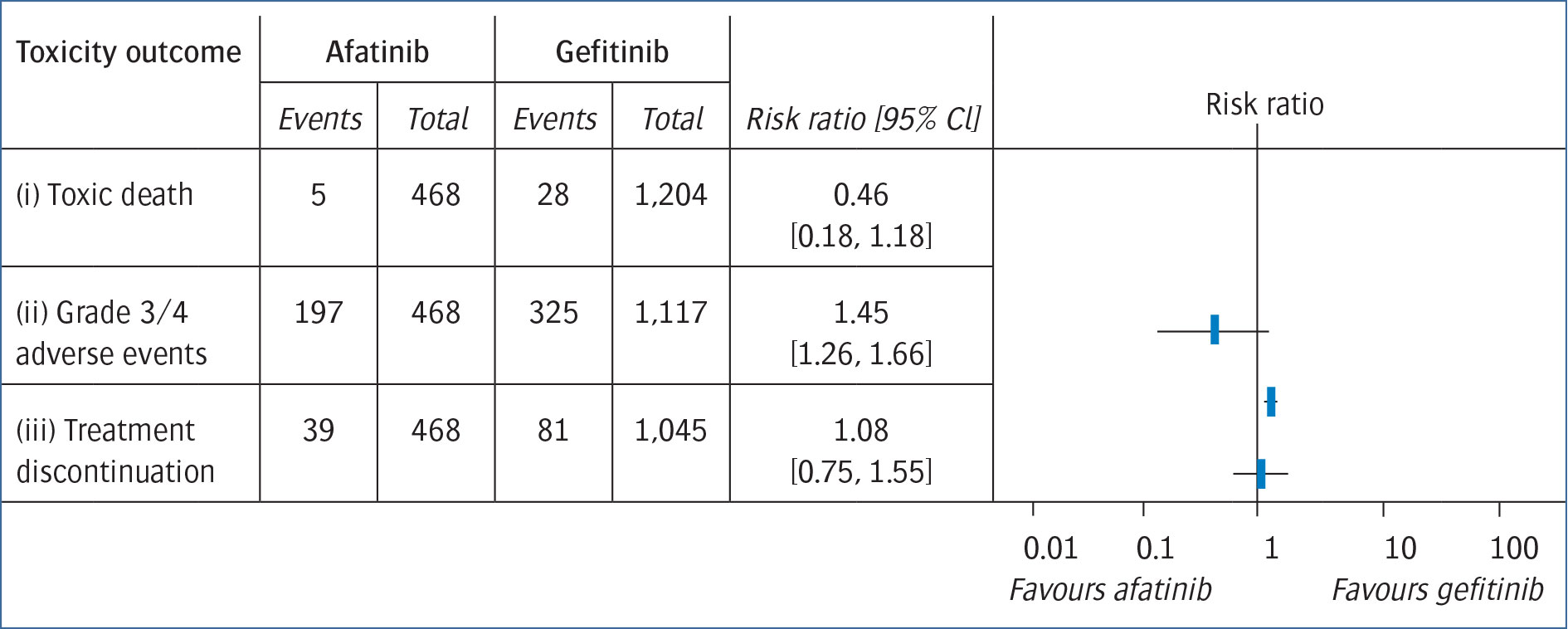
Afatinib resulted in significantly higher rates of diarrhoea (91.7% versus 44.4%, p < 0.01), rash (84.8% versus 62.0%, p < 0.01), stomatitis (61.8% versus 21.8%, p < 0.01), and paronychia (44.4% versus 15.9%, p < 0.01) and more patients had G3/4 toxicities when treated with afatinib than with gefitinib (RR = 1.45, 95% CI: 1.26 to 1.66, p < 0.01) (see Figure 2). Risk for discontinuation of treatment was therefore higher in afatinib (8.3% [95% CI: 5.9 to 11.4%]) when compared to gefitinib (7.8% [95% CI: 6.2 to 9.6%]).
Figure 2. Risk of treatment-related toxicities from EGFR tyrosine kinase inhibitors afatinib and gefitinib(click to enlarge)
When comparing treatment benefits, afatinib showed modest statistical significant improvements with a median PFS of 11.0 months (95% CI 10.6 to 12.9) compared to 10.9 months (9.1 to 11.5) with gefitinib (hazard ratio [HR] 0.73 [95% CI: 0·57 to 0·95], p = 0·017) and a time-to-treatment failure of 13.7 months (95% CI: 11.9 to 15.0) with afatinib versus 11.5 months (10.1 to 13.1) with gefitinib (HR 0.73 [95% CI: 0.58 to 0.92], p = 0.0073).4
When comparing first- and second-generation TKIs to third-generation osimertinib, it has a favourable toxicity profile in both severity and rate of adverse events (AEs). More patients had G3/4 toxicities in the standard EGFR TKI group than in the osimertinib group (45% versus 38%). Osimertinib was comparable in any grade adverse events with 58% developing rash or acne (78% in the standard EGFR TKI group), 58% developing diarrhoea (57% EGFR TKI group), and equal rates of dry skin (36% in each group).8
EGFR TKIs are usually very well tolerated, with less than 10% of instances of cessation of treatment being related to AEs. The side-effect profiles vary between EGFR TKIs in both symptomatology and grading and can be used to inform the choice of treatment for advanced EGFR-mutated NSCLC.
Life after TKIs
Immunotherapy-inhibiting PD-1 and its ligand PD-L1 have been shown to be efficacious as both first-line and second-line treatment, either as monotherapy or in combination with chemotherapy, in improving survival outcomes in the EGFR wild-type NSCLC population. Unfortunately, a recent meta-analysis examining the EGFR-mutated subgroup (n = 186), the pooled HR was 1.05 (95% CI: 0.70 to 1.55, p < 0.81; heterogeneity p = 0.80) when comparing immunotherapy to docetaxel chemotherapy.15
EGFR-mutated lung cancer has been shown to have low mutation burden using next-generation sequencing, providing a plausible biological explanation for the finding of this meta-analysis.16
Additional methods to increase immunogenicity of tumours utilising either additional CTLA-4 inhibitors or using cytotoxic agents to trigger tumour cell death and releasing tumour neo-antigens may potentially improve the host’s immune response.
There are multiple trials currently enrolling that are examining combination strategies with synergistic antitumour activity using immunotherapy as a partner for targeted agents. It is hoped that this approach will represent a promising field for the treatment of patients with EGFR-mutated advanced NSCLC.
References
Ferlay J et al. Cancer incidence and mortality worldwide. IARC Cancer Base No 11. Lyon, France: International Agency for Research on Cancer, 2013
Kelly D et al. A regional analysis of epidermal growth factor receptor (EGFR) mutated lung cancer for HSE South. Ir J Med Sci 2017; 186: 855-7
Rosell R et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol 2012; 13: 239-246
Mok TS, Wu Y-L et al. Gefitinib or carboplatin–paclitaxel in pulmonary adenocarcinoma. N Engl J Med 2009; 361:947-957
Sequist LV et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol 2013; 31: 3327-3334
Lee CK et al. Gefitinib or erlotinib vs chemotherapy for EGFR mutation-positive lung cancer: individual patient data meta-analysis of overall survival. J Natl Cancer Inst 2017; 109(6): djw279
Mok TS et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med 2017; 376: 629-640
Soria JC et al. Osimertinib in untreated EGFR-mutated advanced non-small cell lung cancer. N Engl J Med 2018; 378(2): 113-125
Li X et al. Peripheral blood for epidermal growth factor receptor mutation detection in non-small cell lung cancer patients. Transl Oncol 2014; 7: 341-8
Douillard JY et al. Gefitinib treatment in EGFR mutated Caucasian of EGFR status. J Thorac Oncol 2014; 9: 1345-53
Weber B et al. Detection of EGFR mutations in plasma and biopsies from non-small cell lung cancer patients by allele-specific PCR assays. BMC Cancer 2014; 14: 294
Kwapisz D. The first liquid biopsy test approved. Is it a new era of mutation testing for non-small cell lung cancer? Ann Transl Med 2017;5: 46
Ding PN et al: Risk of treatment-related toxicities from EGFR tyrosine kinase inhibitors: A meta-analysis of clinical trials of gefitinib, erlotinib, and afatinib in advanced EGFR mutated non-small cell lung Cancer. J Thorac Oncol 2017; 12: 633-643
Park K et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a phase 2B, open-label, randomised controlled trial. Lancet Oncol 2016; 17: 577-589
Lee CK et al: Checkpoint inhibitors in metastatic EGFR-mutated non-small cell lung cancer: A meta-analysis. J Thorac Oncol 2017; 12: 403-407
Spigel DR et al. Total mutation burden (TMB) in lung cancer (LC) and relationship with response to PD-1/PD-L1 targeted therapies (abstract). J Clin Oncol 2016; 34: 9017
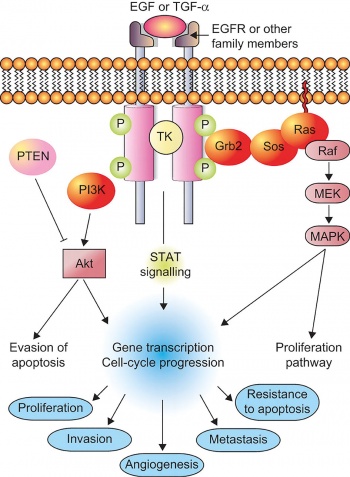 Figure 1. Epidermal growth factor receptor (EGFR) pathway(click to enlarge)
Figure 1. Epidermal growth factor receptor (EGFR) pathway(click to enlarge)