The recent focus on crisis pregnancies has brought renewed attention to effective long-term contraception. In a climate of change, it may be a good time to re-assess our options in this regard. Vasectomy provokes many misconceptions and still tends to engender some fear among some our male patients, who often rely on their female partners to pursue long-term contraceptive options.
‘Vasectomy’ itself is technically a medical misnomer as the vas is interrupted and not completely removed. The prevalence of tubal ligation continues to be greater than vasectomy at a ratio of 5:1, despite the former being a much more invasive and potentially riskier procedure. Vasectomy is safer, simpler, less expensive, and just as effective as female sterilisation.2
Worldwide, approximately 253 million couples rely on sterilisation. An estimated 43 million of these couples rely on vasectomy. Asia accounts for 77% of vasectomy users worldwide, with China and India alone representing more than 70% of the world’s vasectomy users. There is significant global variation in uptake. Bhutan leads by example (40%), with countries such as New Zealand and the UK much to the fore.1
History of procedure
“Necessity is the mother of invention”
In the 1970s, China, struggling with an expanding population, was desperate to enhance and promote all realistic and viable forms of contraception. China’s contentious one- child policy was enacted in 1979, and gives an idea of the landscape at that time. Step forward one Dr Li, from the Sichuan province in China, who pioneered the novel and clever procedure of vasectomy.
He reduced exponentially the risk of bleeding and infection from the procedure2 and was determined to make it more readily acceptable. Vasectomy utilises two specially designed instruments – the round clamp and pointed haemostat, as the mainstay of the procedure (see Picture 1 and 2).
Picture 1: Round clamp (bottom) and pointed haemostat (top)(click to enlarge)
PIcture 2: LiBrand curved mosquito clamp(click to enlarge)
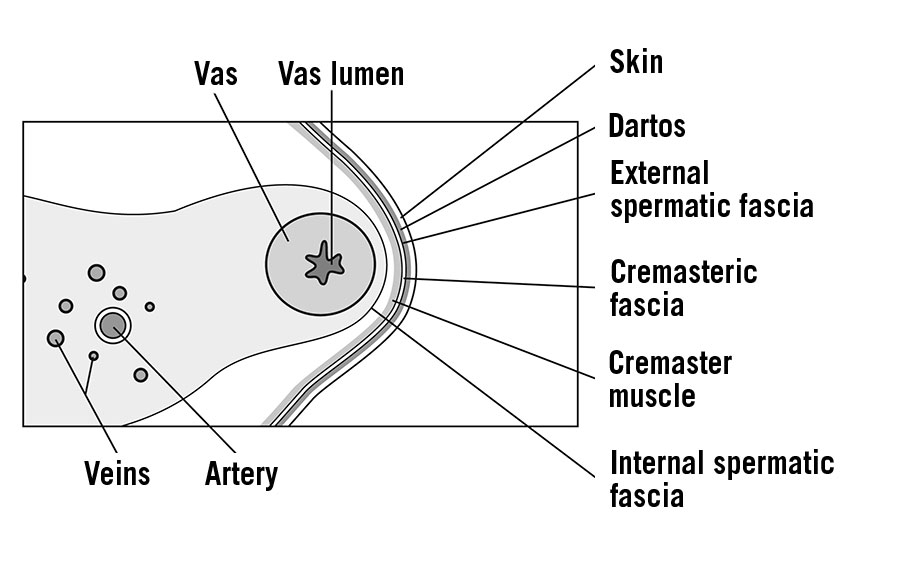
They are specifically designed to easily isolate and externalise the vas, while minimising the risk of serious damage to the proximal vasculature or nerves (see Figure 1).
Figure 1. Cross-section of the spermatic cord(click to enlarge)
By 1985 the first non-scalpel procedure was performed in the US, and by 1989 the procedure had spread to Australia. A seminal study performed in 1988 examined no-scalpel vasectomy with the standard incisional vasectomy in 1,203 patients.10 The non-scalpel vasectomy (NSV) had a complication rate of 0.4% versus the standard incisional vasectomy with 3.1%.2,17 This exponential complication rate difference has since been irrefutably confirmed in countless studies, especially focusing on haematoma and infection rates (see Table 1).
Table 1: Conventional vs non-scalpel vasectomy
Study
No of vasectomies
% with infections
% with haematoma/bleeding
Incisional vasectomy
Philp, Guillebaud, Budd, 1984
Kendrick et al, 1887
Nirapathpongporn et al, 1990
Alderman, 1991
Socal et al, 1999
534
65,155
523
1,224
627
1.3
3.5
1.3
4.0
1.3
4.5
2.0
1.7
0.3
10.7
Non-scalpel vasectomy
Nirapathpongporn et al, 1990
Li et al, 1991
Li et al, 1991
Sokal et al, 1999
Arellano et al, 1997
680
179,741
238
606
1,000
0.2
0.9
0.0
0.2
0.0
0.3
0.1
0.0
1.7
2.1
Pre counselling
Pre counselling offers a welcome opportunity to demystify the procedure with a clear and simple explanation of what it entails. The consent must be fully informed, comprehensive and exact. The goal of the counselling session is to ensure that the client has the appropriate expectations of what will happen in the pre-, intra- and postoperative periods and the consequences of the vasectomy. The patient must be aware that they play a pivotal role in the post-operative recovery and ensuring the procedure is a success by following up with their semen analysis (PVSA). NSV does not work instantaneously and needs a follow-up sample post procedure to safeguard its effectiveness.
Evidence reveals an alarmingly high non-compliance rate submitting this sample post-operatively. Alarmingly, only 78% of patients submit a single PVSA across 46 published studies.16 This percentage of failures occurs due to patients not following the straightforward procedural pathway. I emphasise this point at every verbal and written contact with our patients.
The profile of the patient is noteworthy: younger patients < 27; those under acute stress; partner-driven decision; or significant psychiatric illness should generate caution. A cooling-off period pre a second review can be utilised if the patient profile generates physician concern.1,6 A study revealed a 12.5 times greater likelihood of patients seeking a reversal if they underwent the procedure in their 20s.18 No procedure is of course, without risk, and although a relatively minor procedure, NSV does carry a degree of risk.
Certain measures are utilised to make the procedure technically less challenging for the vasectomist and straightforward for the patient. Examples include a pre-procedural anxiolytic, shaving the scrotal area, applying a hot water bottle to the area immediately prior to the procedure and raising the room temperature to relax the cremasteric reflex.
The key potential complications are:
Bleeding: The risk of bleeding is highly dependent on post-operative care. Recommencing heavy lifting or strenuous exercise prematurely is a key risk. Compliance with post-operative instructions is paramount. Genuine haematomas are rare, and usually self-remitting over a period of up to two months without surgical intervention, but they do delay the overlay recovery significantly. The rate of haematoma is 1-2% in most series.1 Most are self-remitting over time with conservative treatment, and it is extremely rare for surgical drainage to be required.
Infection: Infection is rare and performing the procedure with sterile technique is of course vital. Signs of infection include wound dehiscence, localised purulent discharge, localised erythema, pyrexia or escalating pain, 0.1-2% approximately
Failure: Two types of failure can occur: primary and secondary. Primary failure occurs where the procedure is not confirmed by a clear post-vasectomy semen sample. This dominates the overall failure numbers. The rate of primary failure is dependent on the experience of the vasectomist, but approximates at 1%. The rate of secondary failure, ie. failure after confirmed sterility on post-vasectomy procedure semen sample, is approximately 1/2,000-5,000, depending on which article you read.
Post-vasectomy pain syndrome: Chronic scrotal pain severe enough to interfere with quality of life occurs in 1-2% of men post-vasectomy, according to the American Urological Association1
Sperm granuloma: the rate of the formation of a symptomatic nodule varies based on technique, but in the overwhelming majority of available studies it was diagnosed at < 5% and was rarely symptomatic.
It’s important to be mindful however, that the vast majority of patients do not encounter any of these complications, have an uneventful procedure, return to work within a few days and to normal activity within one week. There is no evidence to support a link between testicular cancers with vasectomy. The weak association in some studies between prostate cancer and vasectomy is unlikely to be causal. There is also no significant evidence to support the link between vasectomy and cardiovascular disease.
After-care and follow-up
Following the procedure, avoiding heavy lifting or strenuous exercise is advised for one week approximately (two to seven days). It is normal to experience some bruising, scrotal swelling and mild discomfort, that usually subsides within a few days. The patient should seek medical advice if experiencing high temperature, worsening pain, swelling or ooze at the wound site. Showers can be taken the day after the procedure, but avoid soaking the scrotum in a bath or hot tub for one week. Wearing tight underwear/athletic support enhances support and aids recovery. Sexual activity should be avoided for one week as per AUA guidelines.1
PVSA (post-vasectomy semen analysis)
There is cross-centre variation on when post-vasectomy samples are submitted but evidence advises not earlier than 12 weeks and at least 20 ejaculations.3,7 The American Urological Association guidelines state that patients may stop using other methods of contraception when examination of one well-mixed, uncentrifuged, fresh post-vasectomy semen specimen shows the absence of sperm.
Patients may discontinue other forms of contraception when fresh post-vasectomy semen specimen shows azoospermia or only rare non-motile sperm (RNMS or ≤ 100,000 non-motile sperm/mL confirmed on two consecutive samples after a period of seven months has elapsed (special clearance).1
According to the Canadian Urological Association, the evaluation of two post-operative semen samples is a better predictor of success than evaluation of a single semen sample.6 The co-operation of local laboratories is vital to ensure that best practice and standards are maintained. Samples must be repeated if there are any inconsistencies in the result or concerns regarding clearance are detected. Motile sperm visualised in a sample post-six months is considered a failure and needs to be repeated.
Safe and effective
Non-scalpel vasectomy is an extremely safe, accessible and effective form of permanent contraception. The algorithm is clear and once rigorously followed compares favourably to other forms of long-term contraception. Couples should be fully informed of all options when at the appropriate stage in their family planning.
 Picture 1: Round clamp (bottom) and pointed haemostat (top)(click to enlarge)
Picture 1: Round clamp (bottom) and pointed haemostat (top)(click to enlarge)