Dr Timothy Ryan, Gastroenterology Registrar, Mater Misericordiae University Hospital, Dublin and Mr Padraic MacMathuna, Clinical Director of BowelScreen and Consultant Gastroenterologist, Mater Misericordiae University Hospital, Dublin
The recent cancer screening service controversy has impaired public confidence. However, with this apparent crisis in screening services comes the opportunity to redefine and refocus the frameworks of these services. In particular, there is a need to re-evaluate the efficacy of these screening programmes and examine if they are learning from new and emerging best practice evidence.
BowelScreen
The National BowelScreen Programme was set up in 2012 and has been running for seven years as an important part of the National Screening Service (NSS). It is one of only two gender-neutral programmes in the NSS. The recently published Round Two Data from the BowelScreen Programme (January 2016 to December 2017) shows slow but steady progress in the detection of cancers and pre-malignant polyps. The major issues continue to be around uptake. The data released shows the importance of raising the public profile of the programme, with colorectal cancer awareness month in April providing the ideal opportunity for this.
The round two data has also been released at an interesting time for colorectal cancer (CRC) screening internationally. The new British Society of Gastroenterology (BSG/ACPGBI) guidelines on moderate and high-risk CRC released in November 2019 rely heavily on returning moderate-risk patients to a national screening programme after initial assessment. This highlights the confidence that exists in the UK that patients with above average risk will receive adequate surveillance in the programme.
In the Irish context, with continued low initial uptake by clients of BowelScreen, the questions we must answer are:
Does the same confidence in the Irish programme exist?
How does this affect the programme and subsequent national CRC screening and surveillance guidelines?
In an attempt to answer these questions, we look at the overall picture of CRC in Ireland, the successes and challenges from the first two rounds of BowelScreen to date and areas that may improve CRC detection for moderate- and high-risk cancer patients as the programme moves forward.
Colorectal cancer in Ireland
Colorectal cancer (CRC) is a major health concern with more than one million new cases each year worldwide. It is the second leading cause of cancer death (510,000). Ireland has one of the highest rates of CRC mortality in Europe with more than 2,400 cases and 1,000 deaths annually.1 CRC is a relatively gender-neutral form of cancer, the second most common form of cancer in men (1,644/year new diagnoses) and third in woman (1,131/year new diagnoses).2 The incidence of CRC is rising. As most of these cancers arise from slow growing polyps/adenomas in the bowel, there is a window to detect them in the pre-cancerous stage and ultimately reduce mortality and morbidity significantly. CRC has the potential to be easily treated; however, the stage at which it is diagnosed is the most important factor to the patient’s prognosis.
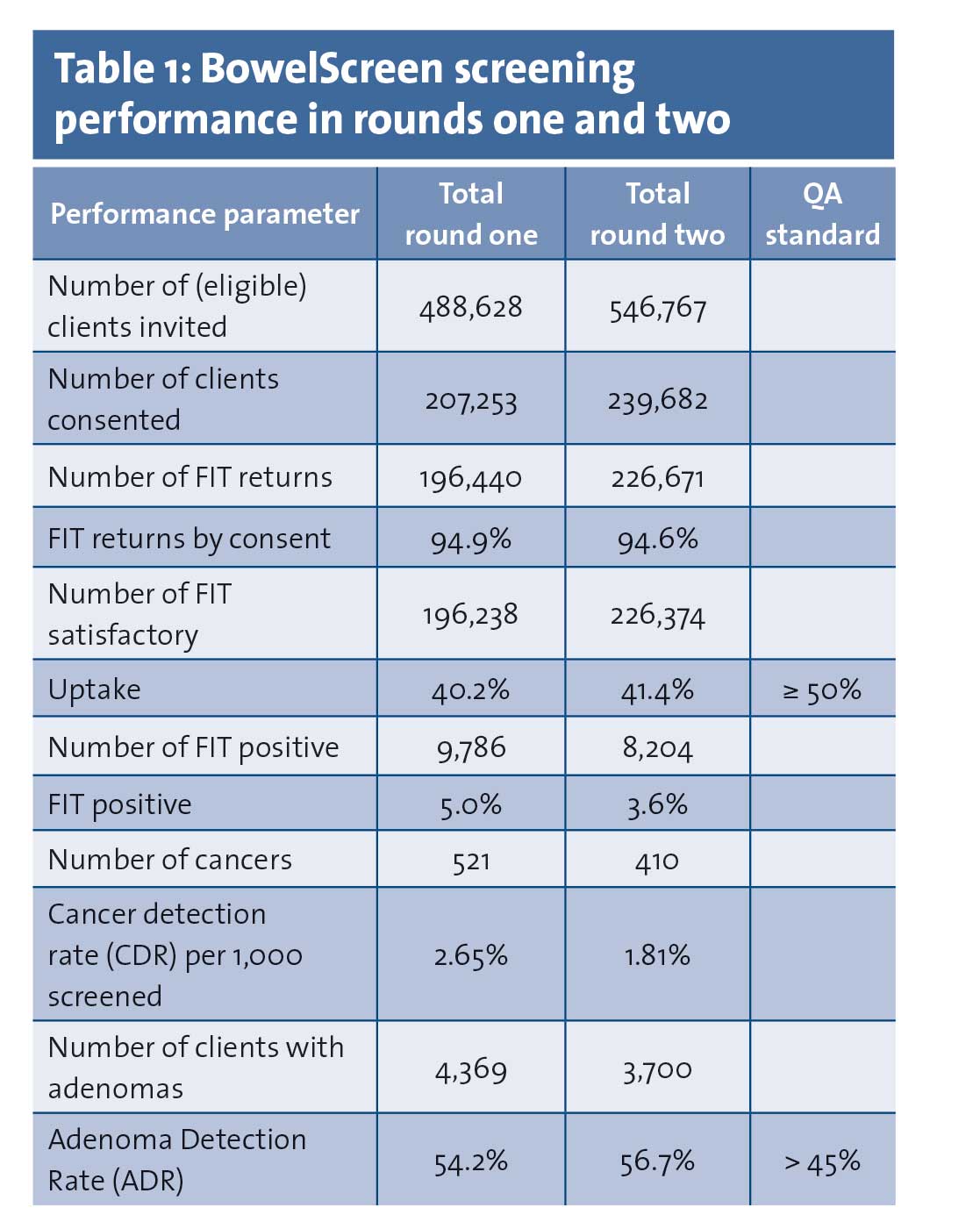
CRC has a five-year survival rate of 90% in those with localised disease and 15% with metastatic disease; hence survival is strongly linked with early detection.3Table 1 compares the screening performance of BowelScreen in rounds one and two.
(click to enlarge)
Round two successes
Slight increase in uptake by 1.2%
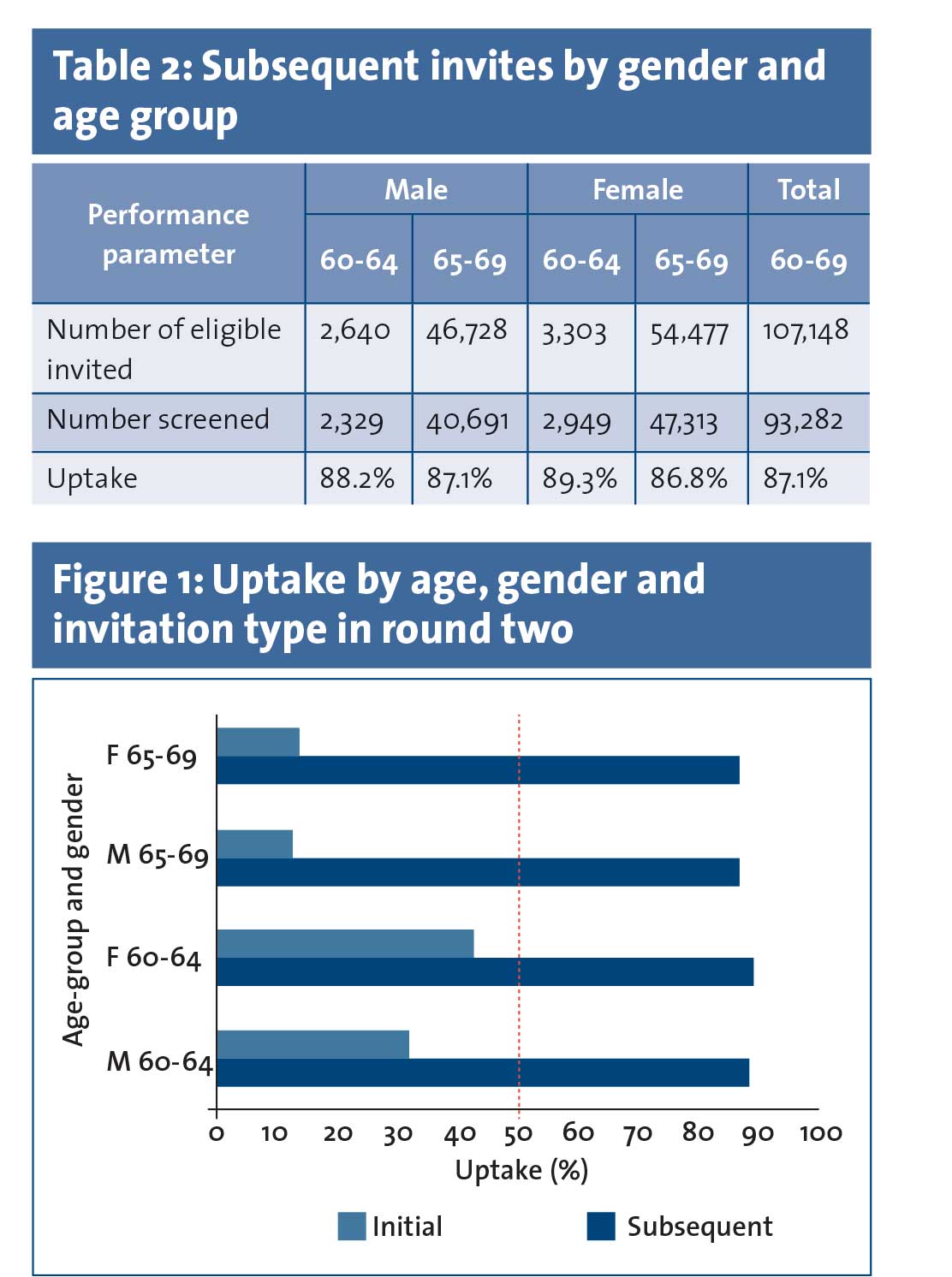
High uptake in the subsequent client group (87.1%), defined as clients who have previously attended BowelScreen and are being invited for the second or subsequent time. Hence it is believed that clients who are already engaged in the programme are satisfied with the test and service (see Table 2)
Similar engagement rates among men and women in the subsequent client category
Unsatisfactory faecal immunochemical test (FIT) rates remained low and these patients were offered a repeat test
Attrition rates from those deemed suitable for colonoscopy after pre-screening to those who actually attended for colonoscopy remained the same in round one and two, at about 6%
All targets were met in regard to colonoscopy performance standards. The use of CT colonoscopy reduced slightly (2.8%), well within the QA standard
High rate of early cancer detection, with 59.9% of cancers detected at Stage I or II
Adenoma detection rates have slightly improved from 54% in round one to 56.7% in round two
Most of the goals on the BowelScreen charter of commitments to clients were met.
Round two challenge
Overall uptake remains poor at 41.4%
A clear gender divide exists in the uptake of initial clients, with a 10.6% difference between male and female uptake in the younger age category (60-64 years of age). Initial clients are defined as clients who are being invited for the first time and also clients who were invited in round one but failed to take up the offer of screening and were re-invited in round two (see Figure 1)
Non-progression of clients to colonoscopy from those referred has increased to 25.8% from 17.6% in round one
Waiting times have also changed from 63% receiving a colonoscopy within the recommended standard of four weeks from pre-assessment in round one to 52% in round two
Of the cancers diagnosed by BowelScreen where the stage was known, over 59% were stage I or II. This is down from 71% in round one
Subsequent client cancer detection rate of 1.48/1,000 may infer that cancers were not present or not detected on initial screening
The percentage of patients receiving first invitation within 24 months of becoming known to the programme or becoming eligible (76.3%) has yet to reach the QA standard of > 90%.4
(click to enlarge)
Planning for the future
Certain challenges remain to be addressed by the BowelScreen programme:
How to increase uptake among initial clients?
What are the barriers to this population engaging with the programme?
How to bridge the gender gap?
Cancer detection rates remain twice as high for men than women in all age categories. One of the questions this raises is, are symptomatic or high-risk men more likely to engage with the programme?
One way this may be achieved is through the lobbying expertise of groups such as the Irish Cancer Society to increase the public profile of the programme and as a result increase compliance. Public awareness campaigns, such as CRC awareness month in April this year, offer the opportunity to increase the profile and awareness of the BowelScreen programme.
BowelScreen has also identified limited colonoscopy capacity and insufficient manpower nationally, particularly endoscopists, to address both symptomatic and BowelScreen referrals.
False-positive FIT
One issue identified to potentially reduce waiting lists is the appropriate follow-up for patients with false-positive FIT tests from initial screening, ie. patients with positive FIT tests who go on to have a normal colonoscopy. Could an extension in FIT intervals reduce demand on overstretched colonoscopy services?
An Irish retrospective study by UCD of false-positive FIT clients followed up in round two of BowelScreen showed a significant reduction in re-attendance rates of these clients. This study emphasises the role of letters to clients from BowelScreen as well as gastroenterologists and advanced nurse practitioner encouragement to get clients to re-attend.5
At present, consideration is being given to continue to offer repeat FIT testing at two years, or extend this out to three to five years, since repeat FIT positive tests at two years after a normal colonoscopy will lead to extra colonoscopies that may not benefit the client.
A 2018 Spanish study from Rivero-Sanchez et al looking at 810 such patients found that 95% of patients did not present with a subsequent lesion to explain the FIT positive result.6 The follow-up FIT testing in this trial was undertaken at 42 and 76 months post negative colonoscopy. This study does offer reassurance that increasing the interval would appear a safe and appropriate use of limited resources.
Incorporation of moderate risk patients into BowelScreen – a worthwhile initiative?
At present BowelScreen, being a purely FIT (stool test) driven programme, does not incorporate above average risk populations either inside or outside of the target age profile. In the UK, the new BSG guidelines on moderate- and high-risk CRC puts an increased emphasis on utilising the UK national screening programme in average- and moderate-risk populations. Moderate-risk individuals are defined as having one first-degree relative with CRC diagnosed before the age of 50, or two first-degree relatives diagnosed at any age. They recommend a one-off colonoscopy at 55 years for these patients and if this is normal then the patient reverts to the national screening programme.
As stated previously, this infers a high level of confidence in the screening programme and, once engaged, that the programme offers sufficient testing to detect potential tumours. The challenge is to establish a co-ordinated high-risk CRC service to be incorporated into the established national BowelScreen programme.
On a positive note, when we examine the high ‘subsequent’ client uptake rates in the round two data, it is far more encouraging that patients already linked in with services will re-engage for future surveillance. As a result, patients that have been referred for assessment and classified as moderate risk are no longer truly ‘initial’ clients and as such are far more likely to engage with the programme. This should give more confidence in the programme for these individuals.
Incorporation of high-risk patients
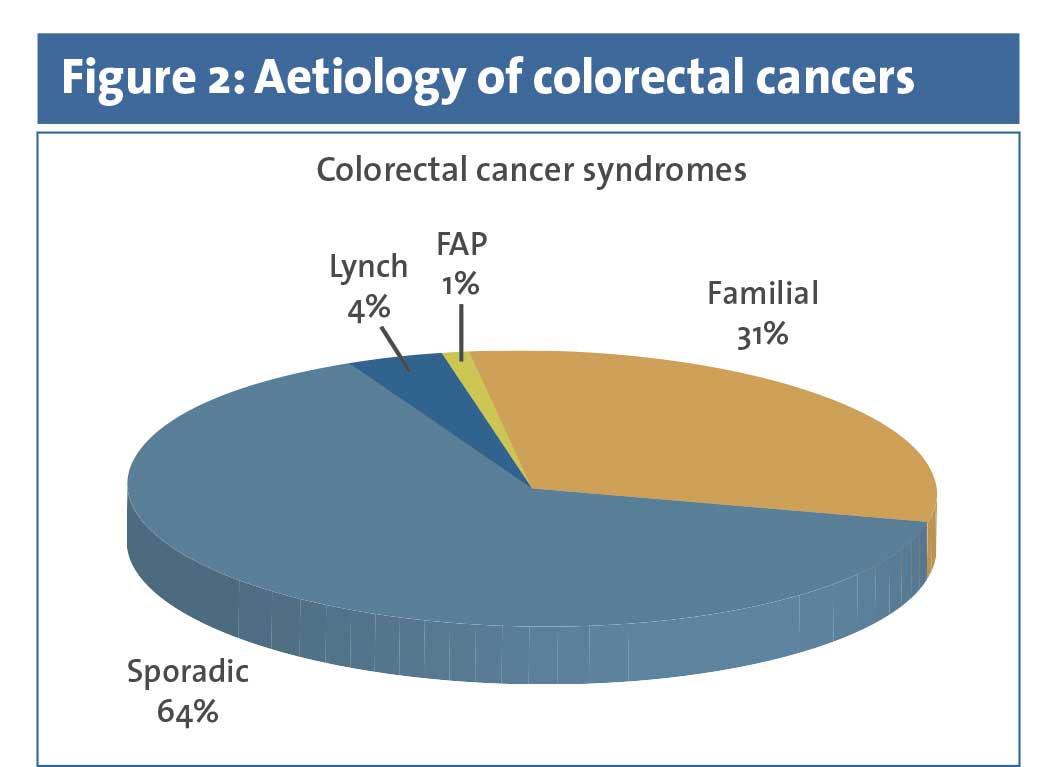
In regard to high-risk patients there is a large deficit in the rates of detection of familial CRCs. The World Health Organization reports that 1 in 30 cases of CRC are as a result of Lynch syndrome (the most commonly known genetic cause of CRC), and that the prevalence of Lynch syndrome in the general population is approximately 1 in 125.7 This makes it two to three times more common than inflammatory bowel disease. However, it is believed that only 5% of individuals at risk are aware of their diagnosis. The total numbers of CRCs attributed to familial syndromes remains unclear at present, however some studies report heritable factors accounting for up to 36% of all CRCs (see Figure 2).8
(click to enlarge)
Currently cases of high-risk CRC are detected either by genetic testing of cancers, most commonly in younger patients believed to be of higher risk of having an underlying syndrome or by clinical algorithms based on family history and relying on a clinician having a high index of suspicion. This is an ad hoc approach to identifying at-risk individuals, with no national guidance or consensus, leaving the potential for cases to be missed. Often family members of those diagnosed with cancer remain unaware of their increased risk of not just CRCs but also uterine, endometrial and others in the case of a patient with Lynch syndrome. This risk can be up to 70% higher than in the general population depending on the gene affected.9
BowelScreen can play a role in increasing detection and surveillance of these individuals given its pre-existing national reach and interaction with all eight cancer centres. By identifying those individuals with tumours suspicious for underlying genetic components, through universal micro-satellite instability (MSI)/immunohistochemistry (IHC) tumour testing, high-risk patients can be triaged out for those that need further genetic testing.
By setting up family cancer clinics within the pre-existing cancer centres, these individuals can be identified and processed through BowelScreen, as an acceptable public health measure. This is of increased importance as genetic testing is becoming readily available, affordable and likely to become more significant in treatment options for patients.
Universal MSI/IHC testing has been thoroughly examined in the 2017 NICE guidelines and shown to be a cost-effective and appropriate first step in identifying at-risk populations.10 Incorporating these tests at a national level through the BowelScreen programme offers the advantage of removing the boundaries of having the same families being followed by multiple hospitals/services and reduces the risk of individuals slipping through the net. The creation and implementation of national guidelines also facilitates the identification of patients who are receiving colonoscopies too frequently and their surveillance intervals can be reduced as appropriate, further reducing the healthcare burden.
Conclusion
The round two data from the BowelScreen programme documents the steady progress being made in CRC prevention and early treatment. The programme has a national profile and is being slowly established as the only cancer prevention gender-neutral programme.
However, significant challenges remain around the areas of uptake of initial clients, sex discrepancies and long colonoscopy waiting lists. Enhancing compliance, incorporating diversity of strategy and planning to include moderate- and high-risk populations, offers exciting initiatives to consolidate the BowelScreen programme as it enters its fourth round.
Timothy Ryan is a gastroenterology registrar at the Mater Misericordiae University Hospital, Dublin, and Newman Fellow at University College Dublin, Padraic MacMathuna is clinical director of BowelScreen, consultant gastroenterologist at MMUH and professor of medicine at UCD, and Sinead Foy is administrator of the Family Screening Clinic at the Gastrointestinal Unit, MMUH
References
Colorectal cancer in Ireland 1994-2010. National Cancer Registry of Ireland. June 2013
Cancer Factsheet Colorectal, National Cancer Registry (updated May 2017). Available online at: https://www.ncri.ie/sites/ncri/files/factsheets/colorectal.pdf
Larsen MB, Njor S, Ingeholm P, et al. Effectiveness of colorectal cancer screening in detecting earlier-stage disease – A nationwide cohort study in Denmark. Gastroenterology 2018; 155(1): 99-106
BowelScreen Statistical Bulletin 2016-2017, National Screening Service. 2019. Available online at: http://www.screeningservice.ie/publications/BowelScreen_statistical_bulletin_2016-2017_FINAL%203_7_19.pdf
Ch’Ng BX, Mooney T, O’Donoghue D, et al. Return to bowel screening after a false-positive faecal immunochemical test in BowelScreen (the National Bowel Screening Programme in Ireland). Journal of Medical Screening 2019; 26(4): 186-90
Rivero-Sánchez L, Grau J, Augé J, , et al. Colorectal cancer after negative colonoscopy in fecal immunochemical test-positive participants from a colorectal cancer screening program. Endoscopy International Open 2018; 6(9): E1140-E1148
Nagtegaal ID, Odze RD, Klimstra D, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020; 76(2): 182-188
Lichtenstein P, Holm NV, Verkasalo PK, et al. Environmental and heritable factors in the causation of cancer – Analyses of cohorts of twins from Sweden, Denmark, and Finland. New England Journal of Medicine 2000; 343(2): 78-85
Møller P, Seppälä T, Bernstein I, et al. Cancer incidence and survival in Lynch syndrome patients receiving colonoscopic and gynaecological surveillance: First report from the prospective Lynch syndrome database. Gut 2015; 66(3): 464-72
National Institute for Health and Care Excellence. Molecular testing strategies for Lynch syndrome in people with colorectal cancer. NICE guidance (DG27); 2017
 (click to enlarge)
(click to enlarge)