Pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms as such”.1 Neuropathic pain is defined as pain caused by a lesion or disease of the somatosensory nervous system, ie. damage or a lesion of the sensory receptors and sensory/afferent neurons in the periphery to deeper neurons within the central nervous (spinal cord, brainstem and thalamus).
Epidemiology
The exact prevalence of neuropathic pain in Ireland is not known. A study published in the European Journal of Pain in 2006 showed 19% of adult Europeans report chronic pain of moderate to severe intensity which seriously affected the quality of their social and working lives.2 Interestingly, this study showed only 2% were currently treated by a pain management specialist and one-third of sufferers had not been treated. A postal survey conducted through general practices in Ireland showed a chronic pain prevalence rate of 35.5%. The prevalence increased with age and was associated with manual employment. Low back pain was the most common type of pain (47.6%), however, multiple pain areas were reported in over 80% of those with chronic pain.3
Studies from France and the UK reported the prevalence of pain of predominantly neuropathic origin or pain with neuropathic characteristics to be 8% and 7% of the general population.4,5 The prevalence of painful peripheral neuropathy was 16% in people with diabetes in the UK, and despite significant disability, 30% of patients had never received any treatment for their neuropathic pain.6 A German study reported 37% of patients with prolonged low back pain had predominantly neuropathic pain.7 The effect of neuropathic pain is substantial, with activities of daily living, including sleep, being affected. Some patients are unable to work, resulting in substantial personal and economic burden. Neuropathic pain will become more common and it is imperative that clinicians become familiar with diagnosing and treating neuropathic pain early on when treatment options are most beneficial.8
Pathophysiology
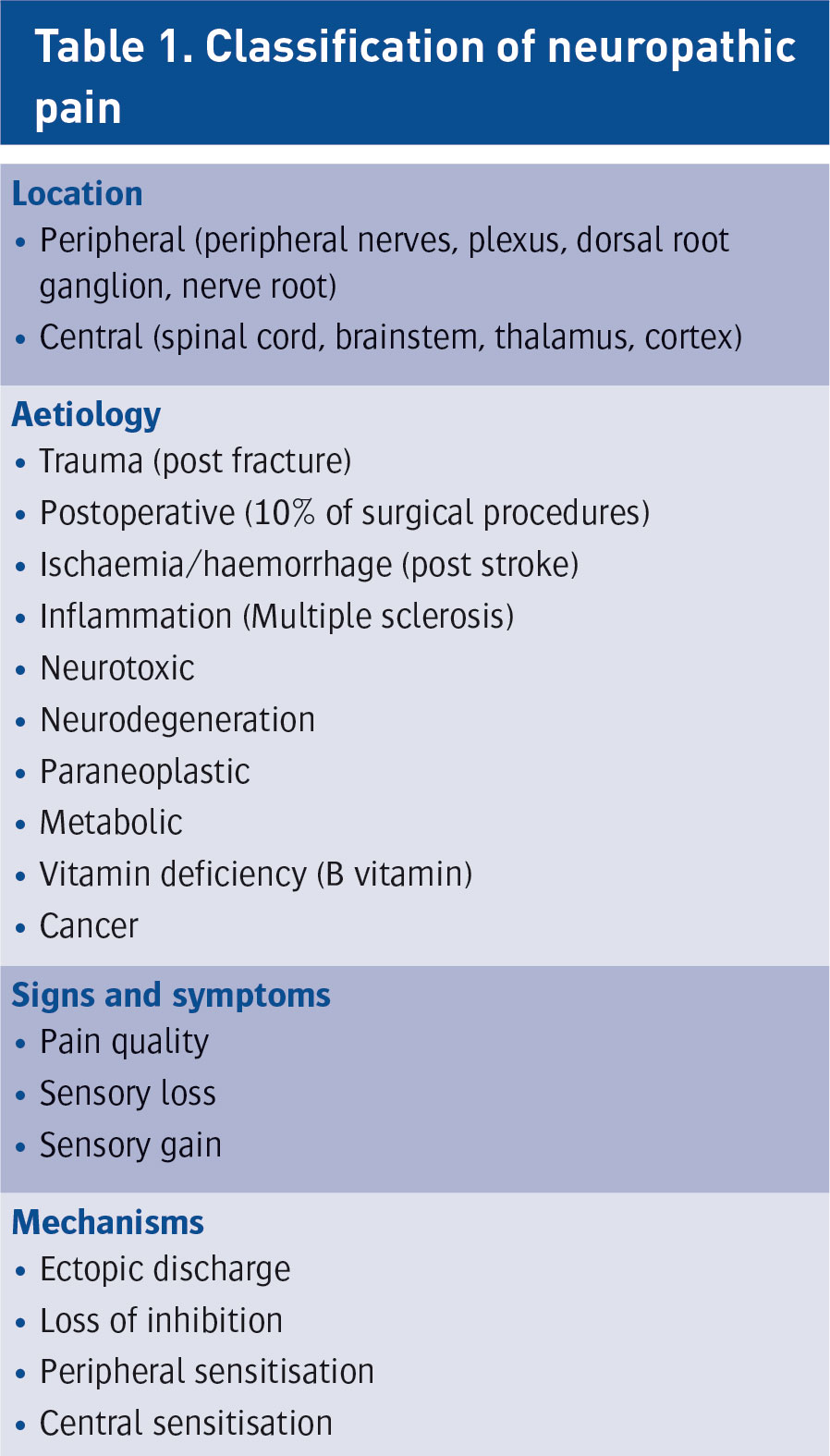
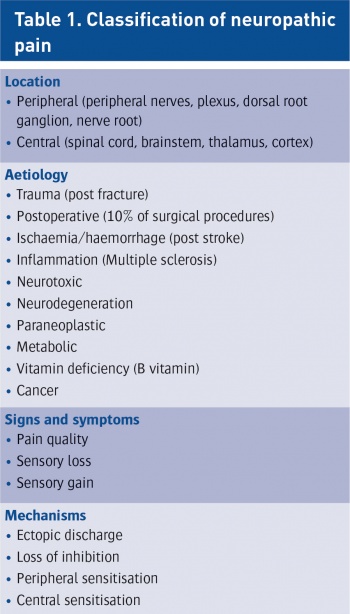
Damage to the nerve pathways can occur at any point from the peripheral sensory receptors to the neurons in the somatosensory cortex in the brain resulting in neuropathic pain. The location and nature of the causative lesion may not be apparent in a general practice setting adding to the challenge of diagnosis and treatment. Neuropathic pain can be classified based on location, on aetiology, on signs and symptoms and on mechanism (to a certain degree) (see Table 1).
(click to enlarge)
A classification based on mechanism alone is not possible. Many patients may have one or multiple mechanisms and display varying levels of pain. Frequently, neuropathic pain is mixed with nociceptive pain, eg. in cancer pain. In these cases, both pain components should be diagnosed and treated as per guidelines.
Clinical features
Neuropathic pain may be constant or intermittent, spontaneous or provoked. Symptoms are described as positive or negative. Positive symptoms are described as: shooting, stabbing, like an electric shock, burning, tingling, tight, prickling, itching and a sensation of pins and needles. Negative symptoms are described in terms of numbness or decreased or lack of sensation in the affected area.8 Signs include:
Paraesthesia (abnormal sensation, spontaneous or evoked)
Dysaesthesia (unpleasant sensation, spontaneous or evoked)
Hypoaesthesia (decreased sensitivity to stimulation; tactile or thermal)
Hyperaesthesia (increased sensitivity to stimulation; tactile or thermal)
Hypoalgesia (diminished pain response to a normally painful stimulus)
Hyperalgesia (an increased response to a stimulus that is normally painful)
Allodynia (pain due to a stimulus that does not normally cause pain).
Other symptoms may be present which may complicate the diagnosis of neuropathic pain, eg. muscle cramping, muscle paralysis, autonomic nervous system changes (skin changes, temperature changes).
Assessment
Assessment of a patient with likely neuropathic pain is aimed at:
First, recognising neuropathic pain
Localising the lesion (peripheral or central, peripheral nerves, plexus, dorsal root ganglion (DRG), spinal cord, brainstem, cortex)
Diagnosing the causative disease or event
Assessing the functional limitations that result from pain.
Assessment of psychosocial aspects is necessary for an individually tailored management strategy. Possible comorbidities include impaired sleep, anxiety, depression, disability, secondary impairment in work, family, and social life.
History and clinical examination
The history should include questions about the location, intensity, character and timeline of the pain, possible relieving and exacerbating factors. Factors such as disturbed sleep and ability to work should be specifically enquired about.
The intensity of the pain may be established verbally (mild to severe), numerically (0-10) or using a visual analogue scale. If nociceptive pain is also present, this should be assessed separately using the above methods.
Pain drawings (where patients mark area of their body which is affected by pain) are an effective method of establishing the anatomical area affected. These allow the clinician to establish the damaged nerve, plexus or root.
Questionnaires can be used in conjunction with history and examination. Questionnaires including the Oswestry Disability Index, Hospital Anxiety and Depression Scale and Pain Catastrophising Scale are used in our institution to establish the psychological impact of patients’ pain. Specific questionnaires exist for the identification of neuropathic pain, for example, Leeds Assessment of Neuropathic Symptoms and Signs (LANSS), Douleur neuropathique 4 questions (DN4), the Neuropathic Pain Questionnaire (NPQ), painDETECT, and ID Pain – all of which use a combination of history and clinical examination to detect neuropathic pain. The sensitivity and specificity of these tests are approximately 80%.9
Management
Management of neuropathic pain consists of non-pharmacological, pharmacological and interventional methods.
Non-pharmacological
Exercise can improve function and decrease pain. There is some evidence that exercise can help with patients’ work disability but degree of improvement is small. One common issue regarding physical therapy is poor patient compliance. This can be improved if the patient attends a group-based activity class. Regardless, exercise should be actively recommended by clinicians.
Results of meta-analysis and systematic reviews of patients with chronic pain suggest that psychological input can offer modest improvement in pain and physical and emotional functioning. Psychological interventions include operant conditioning (positive reinforcement, negative reinforcement) and cognitive-based therapy (eg. mindfulness-based cognitive therapy). These approaches emphasise patient coping, adaptation, self-management and reduction of disability associated with the patients’ symptoms, rather than elimination of physical causes of pain. Psychological techniques used to achieve these goals include cognitive therapy, relaxation, even hypnosis. These techniques help patients to change from being passive, reactive, dependent and helpless, to being active and resourceful in coping with their symptoms.
Pharmacological
Pharmacological guidelines have been published recently by both NICE and in Lancet Neurology.
Regarding a treatment plan, clinicians need to formally acknowledge both the patients’ concerns and expectations regarding that treatment. The most common side-effects of the medications being prescribed must be discussed. Realistic goals for pain control must be agreed. A reduction in pain by 30-50% is considered a positive response. Complete elimination of pain is unlikely in the chronic setting.10,11
The following parameters should be discussed:
The severity of the pain and its impact on lifestyle, daily activities (including sleep disturbance) and participation in activities
The underlying cause of the pain and whether this condition has deteriorated
Why a particular pharmacological treatment is being offered
The benefits and possible adverse effects of pharmacological treatments
The importance of dosage titration and the titration process, providing the person with individualised information and advice
Coping strategies for acute flare-ups and for possible adverse effects of treatment
Non-pharmacological treatments, for example, physical and psychological therapies (which may be offered through a pain management service)
Surgical intervention – appropriate direct referral to surgeons if indicated.
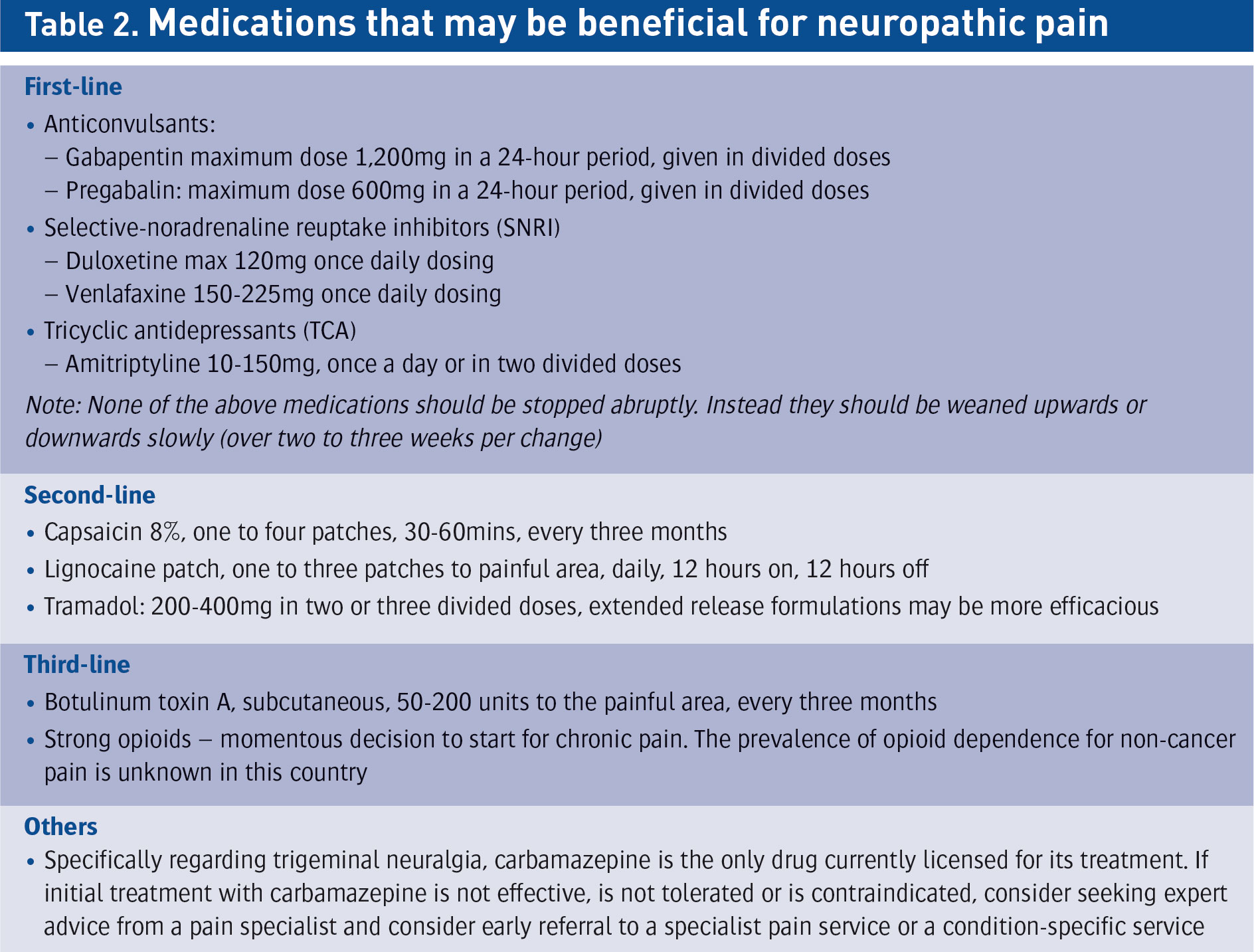
Clinicians should also discuss how therapy should be discontinued if the benefits do not outweigh the risks. Medications that may be beneficial in the management of neuropathic pain are set out in Table 2.
(click to enlarge)
Practical advice on prescribing for neuropathic pain
Offer a choice of amitriptyline, duloxetine, gabapentin or pregabalin as initial treatment for neuropathic pain (except for trigeminal neuralgia, for which first-line is carbamazepine)
If the initial treatment is not effective or is not tolerated, offer one of the remaining three drugs, and consider switching again if the second and third drugs tried are also not effective or not tolerated
Consider tramadol if acute rescue therapy is needed
Consider capsaicin cream for patients with localised neuropathic pain who wish to avoid, or who cannot tolerate, systemic agents.
Prescribing strong opioids
Risk stratification tools do not allow doctors to consistently and accurately identify opioid addiction risk. The risks of opioid overdose and potentially death increases in a dose-dependent manner.11
Deaths from prescribed opioids have quadrupled in the US over the past 15 years. This increase was seen in parallel with an increase in prescribed opioids for pain. A similar increase in opioid prescribing has been seen in the UK.
In an unprecedented move, the Surgeon General in the US issued a letter and opioid prescribing card published in the New England Journal of Medicine in August 2016. The letter called on healthcare professionals to help combat the worsening opioid epidemic in a new campaign called ‘Turn the Tide Rx’. The article included advice on medications to prescribe before opioids, when to prescribe opioids and how to manage opioid doses in patients. The maximum recommended morphine milligram equivalent (MME) is 90mg, and above this level, risks of overdose and addiction escalate markedly. It also briefly discusses protocols in treating opioid overdose and addiction.
The CDC Guideline for Prescribing Opioids for Chronic Pain recommends three key principles:
Non-opioid therapy is preferable for chronic non-cancer pain. Opioids should only be considered in addition to other treatments when the expected benefits outweigh the substantial risks
When opioids are used, the lowest possible effective dose should be prescribed to reduce risk of abuse and overdose. Benefits and risks should be assessed when doses of greater than 50 MME are given per day. Doses above 90 MME should be avoided unless carefully considered and justified
All patients on opioids should be monitored closely. Concurrent benzodiazepines should be avoided. Doses should be regularly reviewed and dose-tapering options should be offered.12
Interventions
Steroid injections
Injection of steroid into the suspected site of nerve injury: if successful, the patient will achieve short to medium term relief from the steroid injection. However, the injection will need to be performed again if the pain returns. Ideally, steroid injections should not be performed more than three times per year. The injections can be performed peripherally or more centrally at the level of the nerve root, dorsal root ganglion or into the epidural space.
Rhizotomy and pulsed radiofrequency (PRF)lesioning
The passage of heat at various temperatures to a peripheral nerve or more centrally causes a small lesion on the nerve. It is thought that the nerve is temporarily ‘reset’.
Neuromodulation
For resistant neuropathic pain, advanced medical technology is used to enhance or depress specific parts of the central or peripheral nervous system. This technology consists of implantable or non-implantable devices that deliver electrical or chemical agents to modulate cells of the brain or nervous system. The advantages of neuromodulation are that it is highly targeted to specific areas of the brain or spinal cord and highly reversible.13
Spinal cord stimulation (SCS)
Failed back surgery syndrome: Spinal cord stimulation involves placing a series of electrodes in the epidural space overlying the dorsal columns of the spinal cord. This results in direct inhibition of pain transmission by the dorsal horn to the brain.
Complex regional pain syndrome (CRPS): CRPS is the second commonest indication for spinal cord stimulation. SCS is a favourable and effective modality for treating CRPS with high-level evidence (1B+). There is a paucity of evidence for functional improvements, resolution of CRPS signs, sleep hygiene, psychological impact, and analgesic sparing effects.14
New developments include burst stimulation, a form of stimulation therapy that delivers closely-spaced pulses of electrical energy to a patient’s spinal cord to manage chronic pain15 and high frequency (HF) spinal cord stimulation with electrodes placed between T9 and T10, which can achieve pain relief of the back and leg (conventional SCS improves leg pain mainly). A recent clinical trial concluded that HF 10KHz stimulation resulted in improved back and leg pain. These patients experience no paraesthesia.16
With dorsal root ganglion, electrodes with four contacts are threaded via the epidural space through the intervertebral foramen to rest on the sensory dorsal root ganglia. Electrical fields are generated that can selectively stimulate different parts of the dorsal root ganglia. This treatment is used for specific pain areas, such as chronic testicular pain and post surgical pain (post herniorrhaphy).17
Spinal cord stimulation requires that a trial lead is placed and if a > 50% reduction in pain is achieved, progression to a full implant is undertaken.
References
IASP: Part III, Pain Terms, A Current List with Definitions and Notes on Usage 1994, 209-214
Breivik H et al. Survey of Chronic pain in Europe: Prevalence, impact on daily life and treatment. Eur J Pain, 2006
McGuire B et al. Chronic pain in the Republic of Ireland community prevalence, psychosocial profile and predictors of pain-related disability, PRIME Study, Pain 2011
Bouhassira D et al. Prevalence of chronic pain with neuropathic characteristics in the general population, Pain, 2008 Jun; 136(3): 380-7
Torrance N et al. The Epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey. J Pain 2006 Apr; 7(4): 281-9
Abbott CA. Prevalence and characteristics of painful diabetic neuropathy in a large community-based diabetic population in the UK. Diabetes Care 2011(Oct); 34(10):2220-4
Freynhagen R. The evaluation of neuropathic components in low back pain, Curr Pain Headache Rep. 2009 Jun; 13(3):185-90
International Association for Study of Pain. Pain Clinical Update, Diagnosis and Classification of Neuropathic Pain 2010 (Sept); 18(7)
Bennett MI. Using screening tools to identify neuropathic pain. Pain 2007; 127:199-203
NICE. Neuropathic pain in adults: pharmacological management in non-specialist settings. Clinical guideline CG173 2014
Finnerup NB, Attal N. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis; Lancet Neurology 2015; 162-73
Frieden TR, Hours D. Reducing the risks of relief - The CDC Opioid-Prescribing Guideline. N Engl J Med 2016; 374:1501-4
Thompson S. International Neuromodulation Society Dec 2016
Visnjevac O. A comprehensive outcome-specific review of the use of spinal cord stimulation for complex regional pain syndrome. Pain Pract 2016 Oct 14
Deer T. St Jude Medical, SUNBURST trial – data analysis ongoing, preliminary results
Kapural L. Novel 10-kHz High-frequency Therapy (HF10 Therapy) Is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: The SENZA-RCT Randomized Controlled Trial, Anesthesiology 10 2015; 123:851-860
Liem L. One-year outcomes of spinal cord stimulation of the dorsal root ganglion in the treatment of chronic neuropathic pain, Neuromodulation. 2015 Jan;18(1):41-8
 (click to enlarge)
(click to enlarge)