Missing an abnormality in the functioning of the thyroid during pregnancy can have devastating consequences for the developing foetus
Dr Faiza Murad, Endocrinology Registrar, Mercy University Hospital, Cork and Dr Sheila O'Sullivan, Consultant Endocrinologist, Mercy University Hospital, Cork
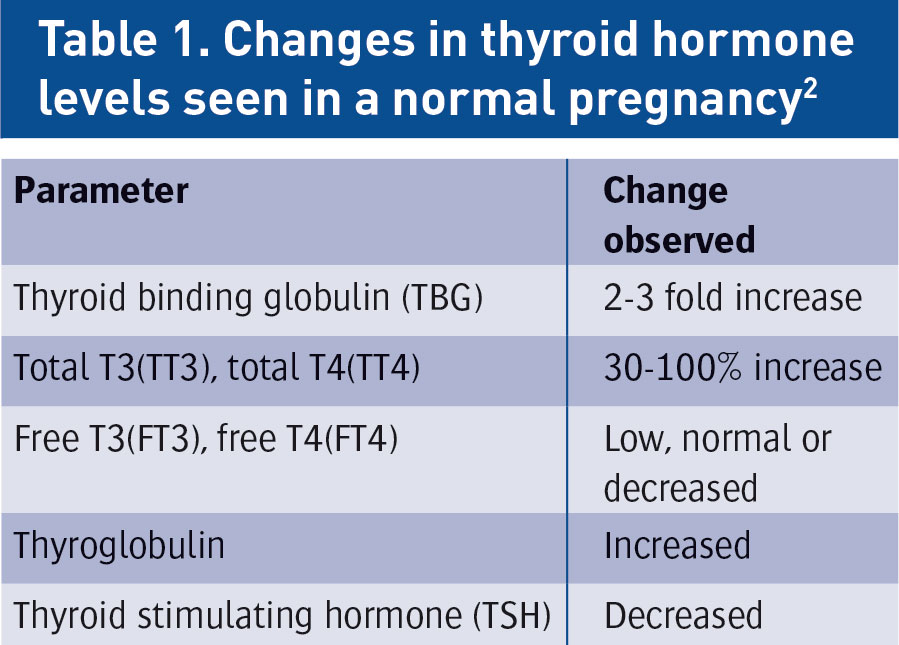
Pregnancy encompasses a range of physiological changes in the female body. Even in a healthy female, the workings of the thyroid gland are significantly altered with conception, producing a picture that in a non-pregnant female would be pathological. Missing an abnormality in the functioning of the thyroid during pregnancy can have devastating consequences for the developing foetus,1 hence there is a vital need to have adequate systems in place for the early identification of these patients and their timely and effective management (see Table 1).
(click to enlarge)
Iodine requirements in pregnancy
In pregnancy, thyroid hormone synthesis increases by 20-40%.3 Concurrently, the demand for dietary iodine is increased and failure to meet this demand can be a cause of thyroid dysfunction. Women in the childbearing age group require 150ug of dietary iodine per day. During pregnancy and breastfeeding, this requirement is increased to 250ug/day. Intake should not exceed 500ug/day.4 Even in the current age of widespread salt iodinisation, the prevalence of iodine deficiency is as high as 50% in parts of Europe and China5 and it is to iodine deficiency that the largest number of cases of preventable foetal brain damage are attributed.6
Screening for thyroid disorders
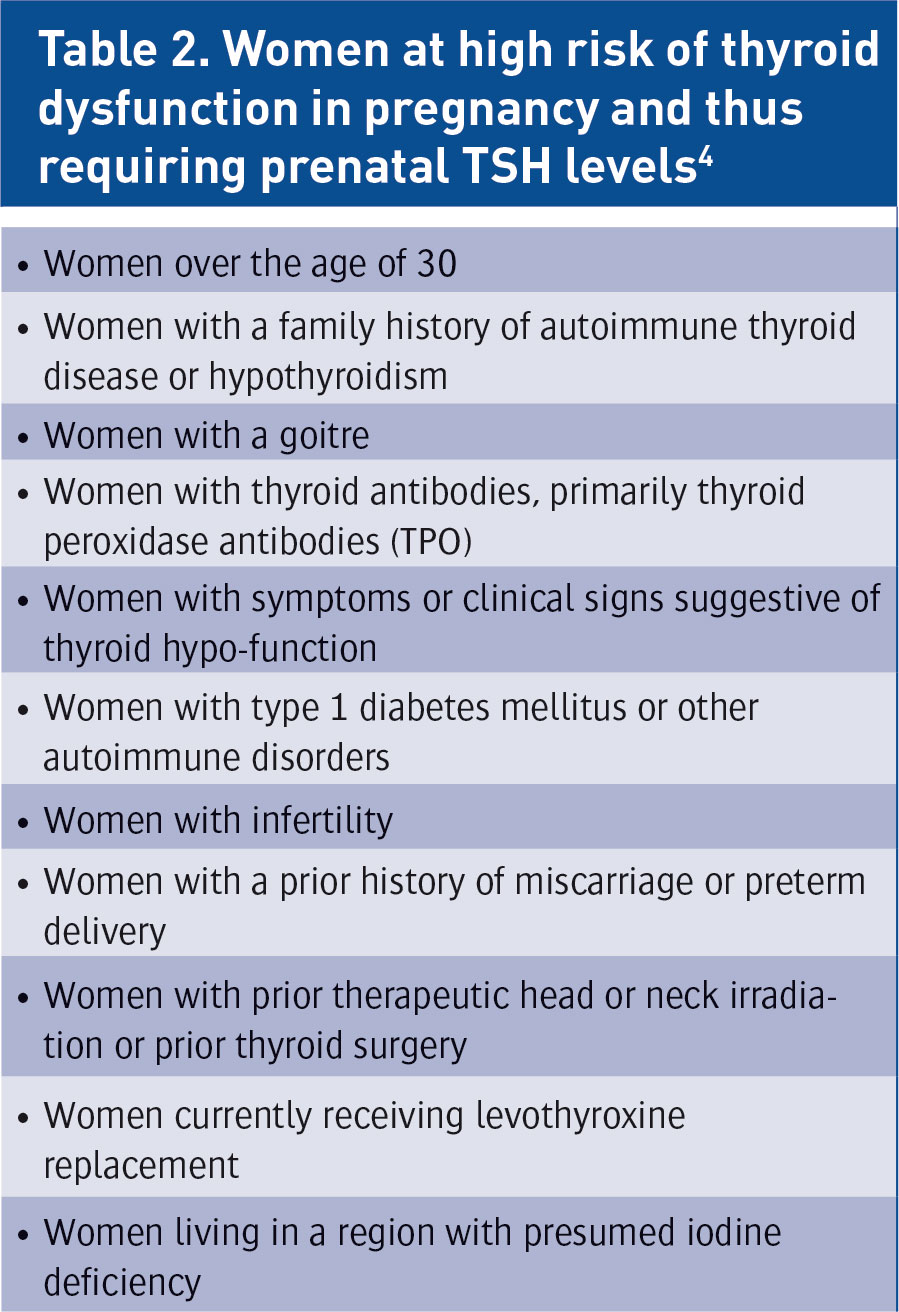
The tests used to assess for thyroid dysfunction in pregnancy and postpartum are the same as those in non-pregnant populations, ie. TSH, T4 and T3 levels, however in assessing the results of these tests, trimester and method specific reference intervals need to be applied.7 Large scale screening of all women prior to pregnancy is not currently recommended.4 By nine weeks of gestation, TSH, T4 and TPO levels should have been assessed in all pregnant females.7Table 2 shows high risk groups who require prenatal TSH levels.
(click to enlarge)
Hypothyroidism in pregnancy
The possible causes of hypothyroidism in pregnancy are:4,8
Iodine deficiency
Autoimmune thyroiditis
Radioiodine ablation or surgery for hyperthyroidism
Thyroid tumour surgery
Congenital hypothyroidism
Lymphocytic hypophysitis.
Subclinical hypothyroidism
If the patient is found to have a normal T4 but a high TSH for the trimester specific range, a diagnosis of sub-clinical hypothyroidism (SCH) is made. Treatment with thyroxine aimed at suppressing the TSH has been found to decrease the incidence of adverse pregnancy outcomes such as preterm delivery, respiratory distress syndrome and foetal and perinatal death.9
In addition to its consequences in pregnancy, the finding of subclinical hypothyroidism can also preclude pregnancy. Thyroid hormones affect fertility in a myriad of ways. Hypothyroidism causes increased thyroid releasing hormone (TRH) production from the hypothalamus, which increases production of prolactin (PL) and thyroid stimulating hormone (TSH) by the anterior pituitary. Prolactin in turn suppresses the pulsatile secretion of GnRH and decreases fertility.
A brief literature review leaves little doubt as to the benefit of using thyroxine in cases of subfertility associated with subclinical hypothyroidism. Yoshiuka et al studied 69 infertile female patients with SCH (mean TSH 5.46) who were treated with thyroxine and documented an 84.1% conception rate.18 Abalovitch et al documented SCH in 19% of women with infertility of greater than one year duration as compared to 3.9% in women with documented fertility.19
The ATA guidelines recommend that levothyroxine replacement for the following subgroups of patients:16
Women of childbearing age who are pregnant or planning a pregnancy, including assisted conception methods, who have positive TPO antibodies or TSH >2.5
Women of childbearing age who desire pregnancy who have positive TPO antibodies or TSH levels >2.5 who have had a past history of miscarriage or hypothyroidism.
New diagnosis of hypothyroidism
In a patient with a new diagnosis of hypothyroidism made during pregnancy, thyroxine treatment needs to be started as soon as possible to reduce TSH level to <2.5 (first trimester) because in early gestation (first 12 weeks), before the foetal thyroid gland begins to function, the foetus is entirely dependent on maternal thyroxine. Thyroid hormone deficiency in this period can lead to a cognitive impairment in the foetus.10 The patient will need frequent testing (every four to six weeks) until thyroid hormone levels stabilise.7
Known hypothyroidism
TFTs should be performed in a patient with known hypothyroidism during the course of a pregnancy at the following times:4,7
Preconception
At time of diagnosis of pregnancy
Antenatal booking
At least once in the second and third trimesters
At two to four weeks postpartum.
The dose of thyroxine will need to be increased to about 30-50% of their usual dose due to higher requirements during pregnancy.11 In the postpartum period, the dose can once again be reduced.
Hyperthyroidism in pregnancy
Hyperthyroidism can develop de novo in pregnancy or can be reactivated in women previously treated for Grave’s disease. Common causes of hyperthyroidism in pregnancy include:4,8
Graves’ disease – 85%
Thyroid nodular disease
Gestational thyrotoxicosis.
Subclinical hyperthyroidism
If a patient is found to have subclinical hyperthyroidism in pregnancy (ie. a suppressed TSH level in the presence of T3 and T4 levels that are normal for that trimester), the current Endocrine Society guidelines do not recommend treatment.4
New diagnosis of hyperthyroidism
If the patient is found to have overt hyperthyroidism, thyroid receptor antibodies (TRAb) need to be measured as they can cross the placenta and affect the foetal thyroid. Treatment is with antithyroid drugs (ATD) and is aimed at keeping the T4 in the upper limit of the reference range.4
There is some controversy about the ideal management of hyperthyroidism in the first trimester of pregnancy. Previously, it was widely held that during pregnancy propylthiouracil (PTU) is much safer. This was due to a recognised association between the use of carbimazole and the development of foetal abnormalities such as aplasia cutis, choanal atresia and aesophageal atresia.12 Due to this, the prescription of PTU relative to carbimazole had increased 3.5 fold in the UK since 1981.13 However, with this increase in the use of PTU came the discovery that it too has teratogenic potential.14 Also the FDA warning regarding fulminant hepatic failure with the use of PTU has made physicians more cautious than ever.15 The current Endocrine Society practice guideline recommends PTU in the first trimester and then advises that the patient be shifted to carbimazole for the remainder of the pregnancy;4 however the same guideline recognises the difficulty in shifting patients from one ATD to another and advises physician discretion.
The American Thyroid Association guideline has given an alternative suggestion that the patient can be given PTU for the entire duration of the pregnancy, with four weekly liver function tests done with each thyroid function test. However, the data demonstrating the success of this approach in preventing the development of fulminant hepatic failure is questionable.16
Indications for surgical management of hyperthyroidism in pregnancy4,16 (subtotal thyroidectomy in hyperthyroid patients carried out in the second trimester) are as follows:
Severe adverse reaction to ATD
High dose requirements for ATD (>30mg/day of methimazole or >450mg/day of PTU)
Non-adherence to drug therapy.
Pre-existing hyperthyroidism
In patients with pre-existing hyperthyroidism, ATD may need to be modified before conception. The block and replace regimen is contraindicated and titration regimens have to be used. The dose of ATD therapy may need to be reduced with the aim of maintaining T4 in the upper end of the preconception range.17 TFTs will need to be assessed again in the postpartum period as this time is associated with a high risk of relapse.7
Gestational hyperthyroidism
DeGroot et al define gestational hyperthyroidism as “transient hyperthyroidism, limited to the first half of pregnancy, characterised by elevated serum T4 and suppressed or undetectable serum TSH, in the absence of thyroid autoimmunity”.4 It has a strong association with hyperemesis gravidarum.
The aetiology of gestational hyperthyroidism include:4,16
• Thyroid stimulation by hCG
• Thyroid stimulation by variant proteins related to hCG
• Multiple gestation
• Hydatiform mole
• Choriocarcinoma
• Thyroid stimulating hormone receptor (TSHR) mutations with functional hypersensitivity to HCG
• Hyperplacentosis
• Hyperreactio luteinalis.
Unless there is co-existent Graves’ disease, ATD therapy is not usually required.
Thyroid nodules in pregnancy
The workup for thyroid nodules in pregnancy is the same as that in the general population with TFTs, thyroid ultrasound and fine needle aspiration (FNA), but radionuclide scans are avoided until the postpartum period.20 If differentiated thyroid cancer is found, surgery can be offered in the second trimester as it does not affect pregnancy outcome adversely.21 If the diagnosis is made in the third trimester, further investigation and treatment can be delayed to after delivery, as this has not been shown to be associated with a worse prognosis.22 The patient can be given thyroxine to suppress the TSH while maintaining T4 in the upper limit of normal for the duration of the pregnancy.4
Postpartum thyroiditis (PPT)
Postpartum thyroiditis (incidence of 5% in iodine replete areas) occurs two to six months postpartum and is characterised by a thyrotoxic phase followed by a hypothyroid phase. Patients with positive thyroperoxidase (TPO) antibodies in pregnancy have a 30-50% chance of developing postpartum thyroiditis.23 It usually resolves spontaneously and the majority of patients will be found to be euthyroid one year after the condition onset.24 This population however has a much higher incidence of developing longstanding hypothyroidism, especially in the presence of high anti-TPO antibodies. Up to 29% of these patients have been shown to be hypothyroid on long term follow up.25
Current guidelines do not recommend screening all women in the postpartum phase for PPT.7
Patients requiring screening for PPT with T4 and TSH levels at six to eight weeks postpartum, are those with:4,7
Goitre
Non-specific symptoms that may be suggestive of thyroiditis
Past history of thyroiditis
Past history of immune disease
TPO positive.
Since PPT is usually self-limiting, treatment is often not necessary. The hyperthyroid phase can be associated with symptoms like palpitations, anxiety and sweating, for which a beta blocker such as propranolol may be used.24 The use of thyroxine to treat the hypothyroid phase depends on the clinical discretion of the physician but it is generally advisable to treat if the hypothyroidism is symptomatic or if the TSH is >10.26
Conclusion
A physician treating a pregnant female is responsible for not one but two patients. Missing a thyroid abnormality can have devastating consequences. The need to follow guidelines that clarify what investigations and management steps to take at different times, to ensure that any thyroid dysfunction is identified and treated, is thus paramount. The subject matter is quite extensive. This is not just the domain of the endocrinologist to be aware of the different thyroid disorders that can manifest in pregnancy and their possible consequences and treatment options. Any physician coming into contact with pregnant women in their professional life should have a grasp of this topic.
References
Haddow J, Palomaki G, Allan W et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med 1999; 341: 549-555
Fantz C, Dagogo-Jack S, Ladenson J, Gronowski A. Thyroid function during pregnancy. Clin Chem. 1999 Dec; 45(12): 2250-2258
Brent G. Maternal hypothyroidism: recognition and management. Thyroid 1999; 9: 661-665
De Groot L, Abalovich M et al. Management of Thyroid Dysfunction during Pregnancy and Postpartum: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab, August 2012, 97(8): 2543-65
Campbell N, Dary O, Cappuccio F et al. Collaboration to optimize dietary intakes of salt and iodine: a critical but overlooked public health issue. Bull World Health Organ 2012, 90: 73-74
Glinoer D. Maternal and fetal impact of chronic iodine deficiency. Clin Obstet Gynecol 1997; 40:102-16
British Thyroid Association website. Guidelines for use of thyroid function tests. Available at: http://www.british-thyroid-association.org/info-for-patients/Docs/TFT_guideline_final_version_July_2006.pdf
Lazarus JH. Thyroid disorders associated with pregnancy: etiology, diagnosis, and management. Treat Endocrinol 2005; 4(1):31-41
De Vivo A, Mancuso A, Giacobbe A et al. Thyroid function in women found to have early pregnancy loss. Thyroid 2010; 20: 633-7
Pop V, Brouwers E, Vader H et al. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study. Clin Endocrinol (Oxf) 2003; 59:282-8
Alexander E, Marqusee E, Lawrence J et al. Timing and magnitude of increases in levothyroxine requirements during pregnancy in women with hypothyroidism. N Engl J Med 2004; 351:241-9
Cooper D. Antithyroid drugs. N Eng J Med 2005, Vol 352:328-31
Pearce SHS. Spontaneous reporting of adverse reactions to carbimazole and propylthiouracil in the UK. Clinical Endocrinology 2004; 61(5):589-94
Hackmon R, Blichowski M, Koren G. The safety of methimazole and propylthiouracil in pregnancy: a systematic review. J Obstet Gynaecol Can. 2012 Nov; 34(11):1077-86
FDA.org. New boxed warning on severe liver injury with propylthiouracil. 2010 April. Available online at http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm
Bahn R, Burch L, Cooper D et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the ATA. Hyperthyroidism Management Guidelines, Endocr Pract 2011; 17
Masiukiewicz U, Burrow G. Hyperthyroidism in pregnancy: Diagnosis and treatment. Thyroid 1999; 9: 647-52
Yoshioka W, Amino N, Ide A et al. Thyroxine treatment may be useful for subclinical hypothyroidism in patients with female infertility. Endocr J 2015; 62(1):87-92
Abalovich M, Mitelberg L, Allami C et al. Subclinical hypothyroidism and thyroid autoimmunity in women with infertility. Gynecol Endocrinol 2007 May; 23(5):279-83
Cooper D, Doherty G, Haugen B et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009; 19:1167-214
Sam S, Molitch M. Timing and special concerns regarding endocrine surgery during pregnancy. Endocrinol Metab Clin North Am 2003; 32: 337-54
Moosa M, Mazzaferri E. Outcome of differentiated thyroid cancer diagnosed in pregnant women. J Clin Endocrinol Metab 1997; 82: 2862-6
Amino N, Tada H, Hidaka Y. Postpartum autoimmune thyroid syndrome: a model of aggravation of autoimmune disease. Thyroid 1999; 9:705-13
Stagnaro-Green A. Postpartum thyroiditis. J Clin Endocrin Metabol 2002; 87(9):4042-7
Othman S, Phillips DIW, Parkes AB et al. A long-term follow-up of postpartum thyroiditis. Clin Endocrinol (Oxf) 1990; 32: 559-64
Stuckey BGA, Kent GN, Allen JR. The biochemical and clinical course of postpartum thyroid dysfunction: the treatment decision. Clin Endocrinol (Oxf) 2001; 54: 377-83
 (click to enlarge)
(click to enlarge)