For GPs to effectively manage dyslipidaemias, the patient’s level of total CV risk and LDL-C must be calculated and lipid-lowering therapy titrated upwards until recommended targets are attained
Cardiovascular disease (CVD) due to atherosclerosis of the arterial vessel wall and to thrombosis is the foremost cause of premature mortality and morbidity in Europe. The main clinical entities are coronary artery disease (CAD), ischaemic stroke, and peripheral arterial disease (PAD).
The causes of these CVDs are multifactorial. Some of these risk factors, such as smoking, lack of physical activity, dietary habits, elevated blood pressure, type 2 diabetes, and dyslipidaemias, are modifiable.
Introduction
Prevention and treatment of dyslipidaemias should always be considered within the broader framework of CVD prevention, which is addressed in the recently published 2019 European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) Task Force guidelines for the management of dyslipidaemias.1
Some appreciation of the enormity of the problem of dyslipidaemia in general practice in Ireland can be got from the SLÁN data, where ‘high’ total cholesterol was determined as those having levels of > 5.0mmol/L.2 Over three-quarters of the sample (82%) had raised cholesterol, with most (62%) not on cholesterol-lowering medication. One-third (35%) of those treated with medication for cholesterol were not controlled.
Similarly, the Irish Longitudinal Study on Ageing (TILDA) reported that only over a third of the over-50s with known CVD; 47% of those with known diabetes; and 85% of those with a Systematic Coronary Risk Estimation (SCORE) risk greater than or equal to 5% were above a low-density lipoprotein cholesterol (LDL-C) target of 2.5mmol/L.3 Statins were used by only just over two-thirds of those with known CVD; just over half of those with known diabetes; and by just less than a fifth of adults with a SCORE risk greater than or equal to 5%. As these data show, despite strong evidence and clinical guidelines on the use of statins in Ireland, a gap exists between what the guidelines recommend and actual practice in this cohort.
ESC/EAS guidelines
The key messages regarding lipid levels and CVD prevention from the 2019 ESC/EAS guidelines1 can be summarised as follows:
The key initiating event in atherogenesis is the retention of LDL-C and other cholesterol-rich apolipoprotein (Apo) B containing lipoproteins within the arterial wall
The addition of either ezetimibe or anti-proprotein convertase subtilisin/kexin type 9 (PCSK9) monoclonal antibodies (mAbs) to statin therapy provides a further reduction in atherosclerotic cardiovascular disease (ASCVD) risk, which is directly and positively correlated with the incrementally achieved absolute LDL-C reduction
The lower the achieved LDL-C values, the lower the risk of future cardiovascular (CV) events, with no lower limit for LDL-C values, or ‘J’-curve effect
For raising high-density lipoprotein cholesterol (HDL-C), recent studies have indicated that the currently available therapies do not reduce the risk of ASCVD
Human Mendelian randomisation studies have demonstrated the critical role of LDL-C, and other cholesterol rich ApoB-containing lipoproteins, in atherosclerotic plaque formation and related subsequent CV events. Thus, there is no longer an ‘LDL-C hypothesis’, but established facts that increased LDL-C values are causally related to ASCVD, and that lowering LDL particles and other ApoB-containing lipoproteins as much as possible reduces CV events
For general risk screening, non-fasting samples seem to have at least the same prognostic value as fasting samples
Lifestyle and dietary changes are recommended for all.
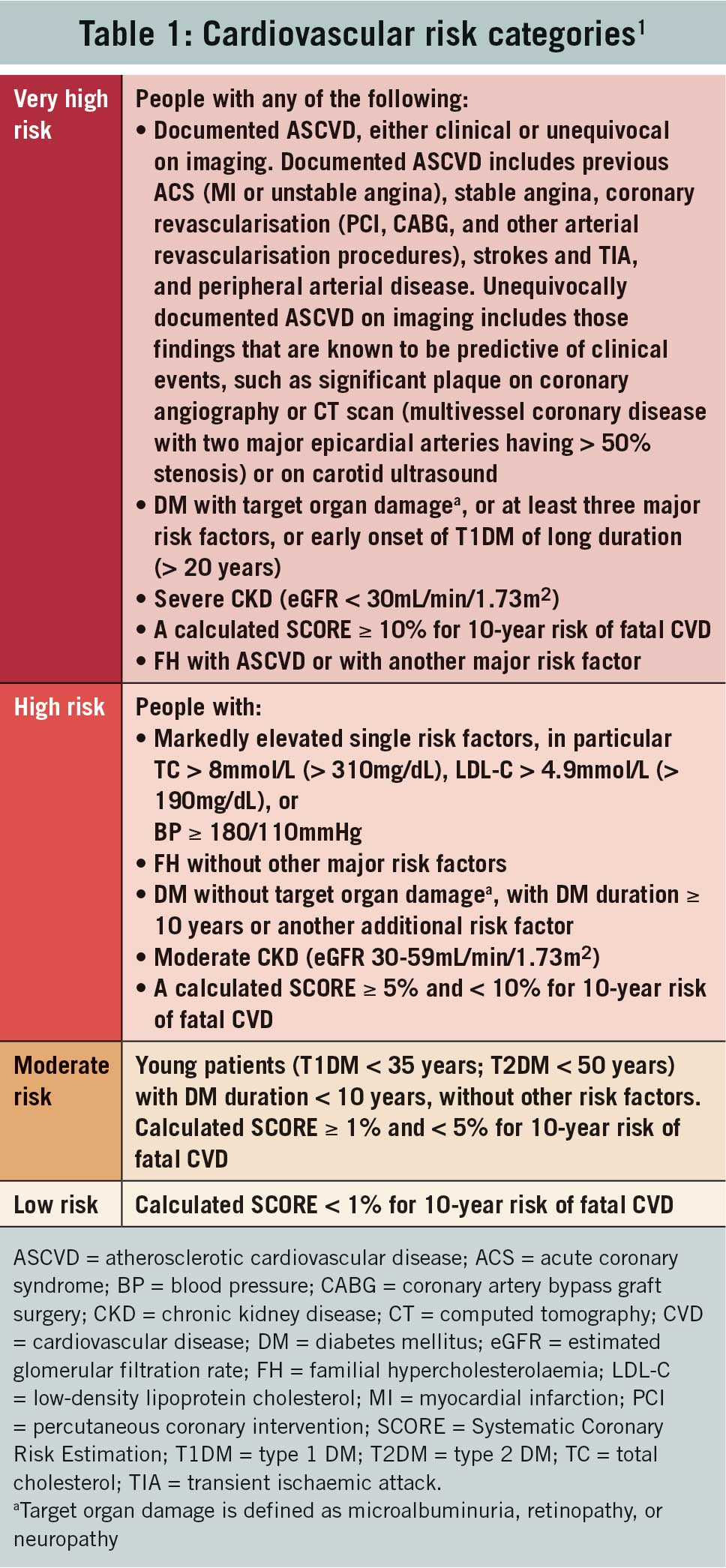
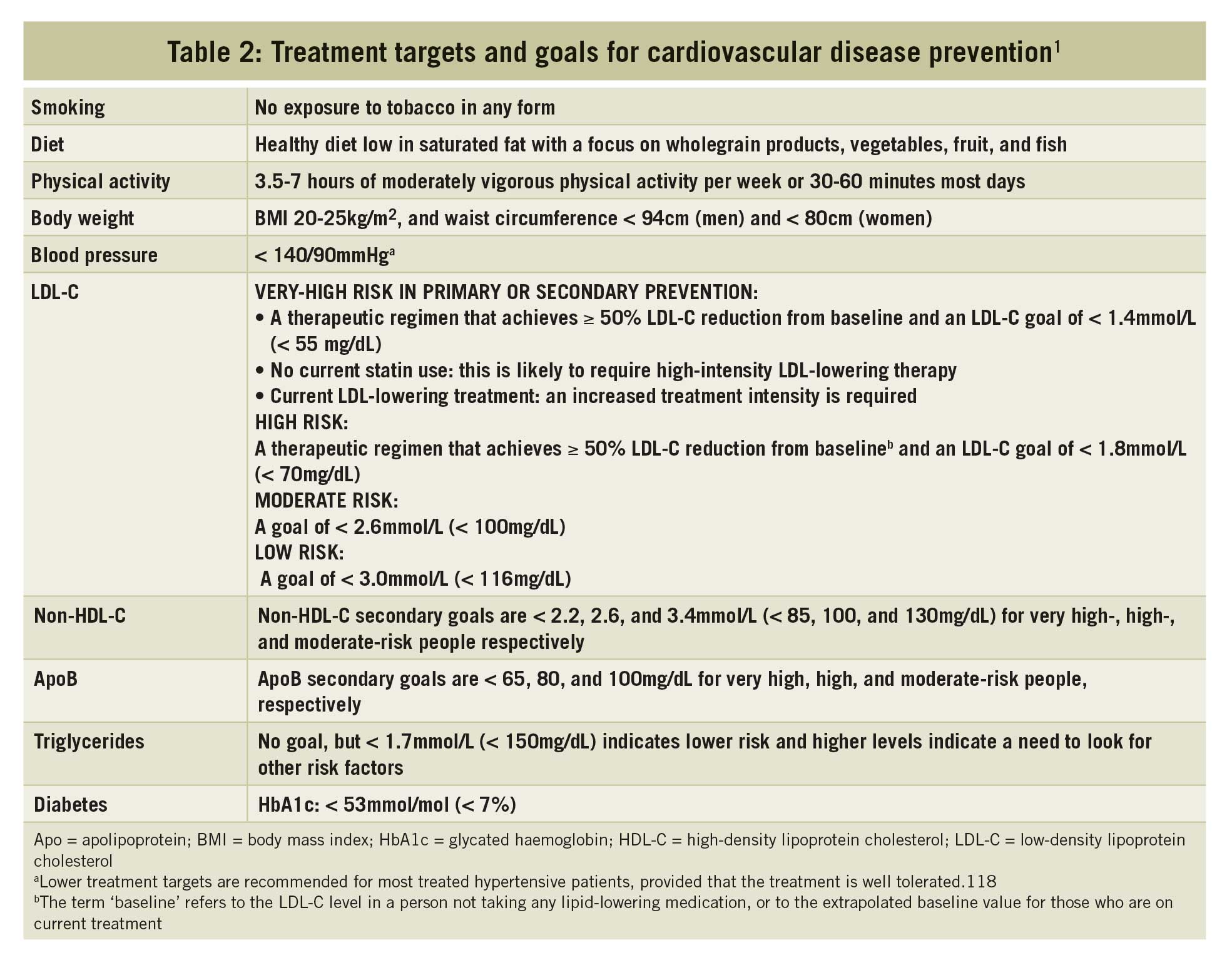
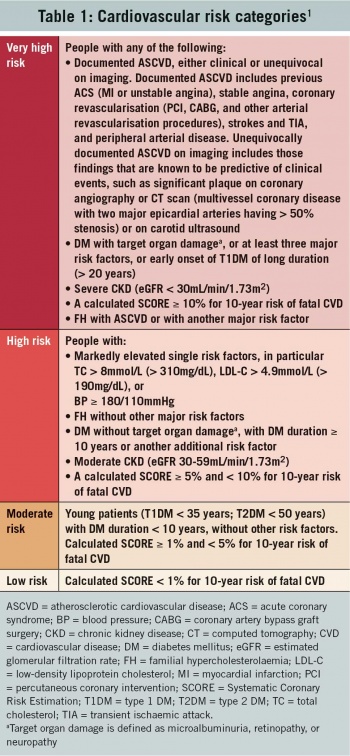
The revised cardiovascular risk categories are given in Table 1. Treatment targets and goals for cardiovascular disease prevention are given in Table 2.
(click to enlarge)
(click to enlarge)
Please note that for patients with ASCVD who experience a second vascular event within two years (not necessarily of the same type as the first event) while taking maximum tolerated statin therapy, an LDL-C goal of < 1.0mmol/L may be considered.
If LDL-C goals are not achieved with the maximum tolerated dose of statin, combination with ezetimibe is recommended. For secondary prevention, patients at very-high risk not achieving their goal on a maximum tolerated dose of statin and ezetimibe, a combination with a PCSK9 inhibitor is recommended.
Statin treatment is recommended as the first drug of choice for reducing CVD risk in high-risk individuals with hypertriglyceridaemia, that is triglyceride (TG) levels > 2.3mmol/L). In high-risk (or above) patients with TG levels between 1.5 and 5.6mmol/L (135-499mg/dL) despite statin treatment, n-3 PUFAs (icosapent ethyl 2, 2g/day) should be considered in combination with statins.
In primary prevention, for individuals with familial hyperlipidaemia (FH) at very-high risk, an LDL-C reduction of > 50% from baseline and an LDL-C goal of < 1.4mmol/L should be considered.
Treatment with statins is recommended for primary prevention, according to the level of risk, in older people aged < 75. Initiation of statin treatment for primary prevention in older people aged > 75 may be considered, if at high risk or above.
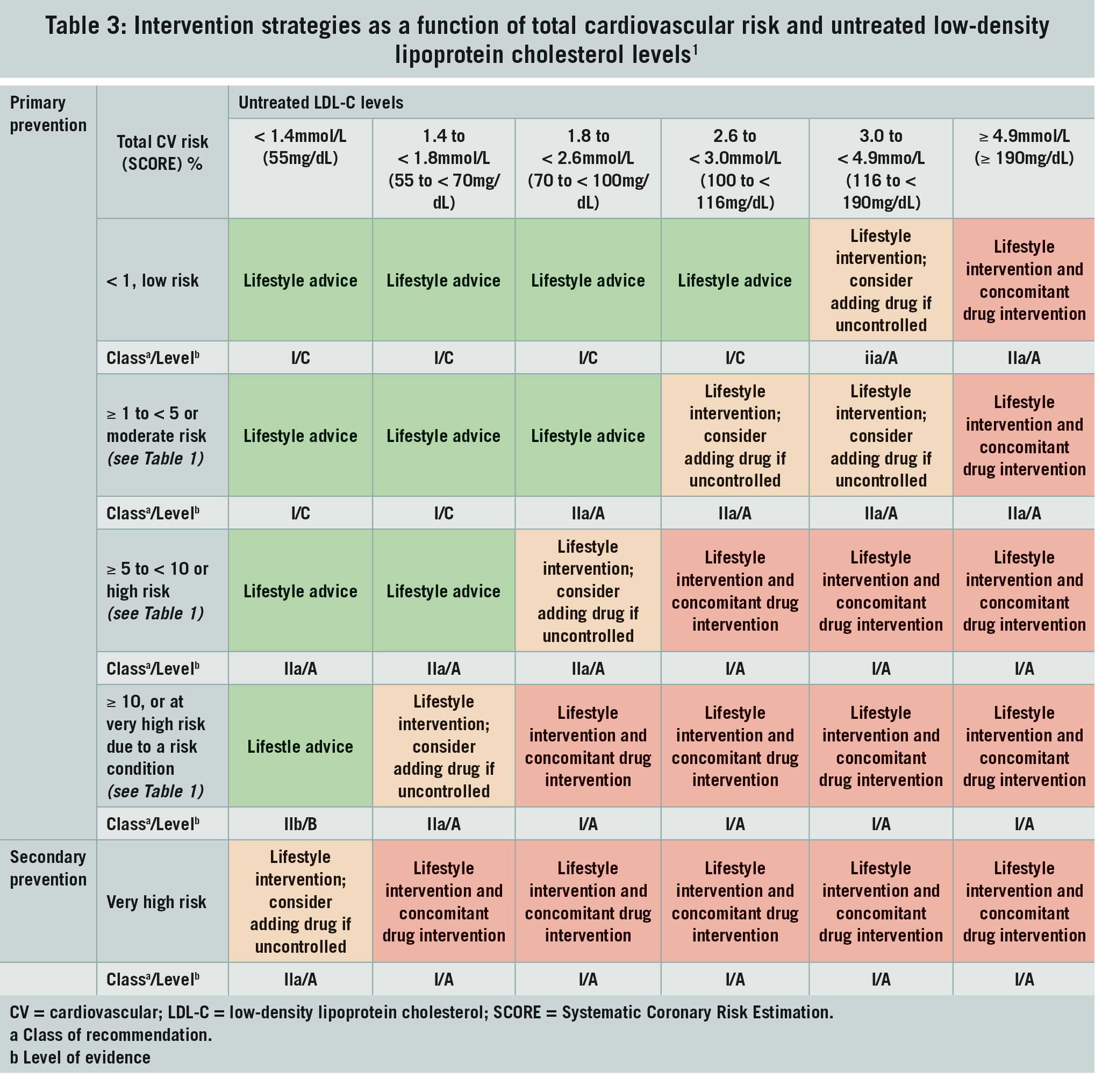
Intervention strategies as a function of total cardiovascular risk and untreated LDL-C levels are given in Table 3.
(click to enlarge)
We will now use the 2019 ESC/EAS guidelines to manage some typical cases we would meet in practice.
Case 1: A farmer aged 47
Mr PC is a local farmer aged 47. His wife, who is a nurse, has sent him to you for a check-up. He is a non-smoker, his BMI is normal and his blood pressure is 134/85mmHg. His total cholesterol (TC) is 7.0mmol/L, LDL-C is 4.0mmol/L, HDL-C is 1.3mmol/L and TGs are 1.5mmol/L.
We are all familiar with the request, usually from a perfectly healthy young man, for a ‘cholesterol test’ often as part of what is referred to as a ‘complete check-up’. Some laboratories have written to GPs asking that they adopt a more evidence-based approach to requests for ‘routine’ lipid profiles in their patients.
The current guideline recommends risk factor screening, including the lipid profile in adult men ≥ 40 years of age, and in women ≥ 50 years of age or post-menopausal, particularly in the presence of other risk factors. However, all subjects with the conditions listed in the very high, high and moderate risk groups outlined above, irrespective of age, should be assessed.
Another important issue for GPs, who do most of their risk factor screening on an opportunistic basis, is whether the specimen has to be taken from a patient in a fasting or non-fasting state. Thankfully, the present guidelines acknowledge that for general risk screening such as we do in our surgeries, non-fasting samples seem to have at least the same prognostic value as fasting samples.
As our patient Mr PC is a healthy man with no history of CVD, diabetes or chronic kidney disease, we need to calculate his cardiovascular risk. How we do this will probably depend on the software we use on our practice computers as some programmes give an automatic QRISK®3 or HeartScore result.
This raises the very practical point of how to convert a QRISK®3 result, which is based on fatal + non-fatal CV events, to HeartScore, which is based on the fatal CV events. The original text as written in the 2019 ESC/EAS guidelines1 is as follows: “To convert the risk of fatal CVD to risk of total (fatal + non-fatal) CVD, multiply by 3 in men and by 4 in women, and slightly less in older people – so a SCORE risk of 5% in a middle-aged man translates into a CVD risk of ∼15% of total (fatal + non-fatal) CVD endpoints.”
However, in the context of the busy world of general practice, (especially in the middle of the flu season!), we could I think be forgiven for simplifying this as follows:
QRISK®3 > 30% ≈ SCORE > 10%
QRISK®3 15-29% ≈ SCORE 5-9%
QRISK®3 5-14% ≈ SCORE 1-4%
QRISK®3 <5% ≈ SCORE < 1%.
I have calculated our patient’s QRISK®3 result at 3.2%. I have also calculated his total CVD risk at 1% using HeartScore (moderate risk – see Table 1). Interestingly, had I used QRISK®3 and the conversion above, I would have got a SCORE < 1% (low risk – see Table 1). Going to Table 2, we see that the treatment goal for primary prevention in a case such as ours with moderate risk is an LDL-C level of < 2.6mmol/L. For a person with low risk, it is an LDL-C of < 3.0mmol/L.
In Table 3 we see that the intervention strategies for a person at moderate risk and low risk of CVD and an untreated LDL-C level of 4.0mmol/L are lifestyle intervention and the recommendation that we consider adding a drug if LDL-C level is uncontrolled on these measures. In practice, I often find a family history of premature CVD in first-degree relatives, that is before 55 years of age in men and 65 years of age in women, helpful in making the decision to start drug treatment in this situation.
As with previous versions of this guideline, a large emphasis is placed on lifestyle modifications to improve the plasma lipid profile. All GPs and practice nurses should have copies of the excellent Irish Heart Foundation leaflet A healthy cholesterol for a healthy heart’ available when discussing cholesterol-lowering diets with their patients. This leaflet can be viewed at https://irishheart.ie/publications/a-healthy-cholesterol/. Similarly, the benefits of exercise and weight reduction in the reduction of LDL-C and the raising of HDL-C levels are emphasised in the guideline. Again, the relevant Irish Heart Foundation leaflets are invaluable.
Case 2: A retired teacher aged 67
Ms DC is a retired teacher aged 67 who has recently been diagnosed with uncomplicated type 2 diabetes. She is a non-smoker, her BMI is normal and blood pressure is 130/74mmHg. Her total TC is 6.4mmol/L, LDL-C is 4.5mmol/L, HDL is 1.1mmol/L and TGs are 1.2mmol/L.
We start by establishing the level of total CVD risk this lady has. From Table 1 we see that this lady is in the high-risk group. Note that persons in the high-risk group do not need to have a QRISK®3 or SCORE/HeartScore calculation as they are already at high risk of complications of CVD.
For patients at high risk, such as our Ms DC, an LDL-C reduction of > 50% from baseline and an LDL-C goal of < 1.8mmol/L are now recommended (please see Table 2). The treatment goal of an LDL-C reduction of at least 50% from baseline (50% of 4.5mmol/L) comes to 2.25mmol/L. Thus, an LDL-C of less than 1.8mmol/L is now the treatment goal for this patient according to the current guideline.
In terms of management (please see Table 3), we see that for a high-risk patient with an LDL-C of 4.5mmol/L, lifestyle intervention, as already discussed above, and concomitant drug intervention are recommended. Treatment with statins is recommended for primary prevention, according to the level of risk, in older people aged < 75. This lady requires prescription of a statin to achieve the treatment target of < 1.8mmol/L specified above.
A chemical in grapefruit can increase the level of some statins (simvastatin, atorvastatin and lovastatin) in the bloodstream, which can make side-effects from the statin more likely. It is a good idea to print a patient information leaflet with the first prescription from the link https://patient.info/health/statins-and-other-lipid-lowering-medicines. Please note that patients should stop statin therapy if prescribed clarithromycin (or other potent inhibitors of cytochrome P450 3A4) as this combination increases the risk of myopathy and rhabdomyolysis by increasing the concentration of HMG-CoA reductase inhibitory activity in the plasma.
Case 3: A 57-year-old with three stents
Mr JB is a 57-year-old who had three stents inserted last year following an ST-elevation myocardial infarction. In spite of “maximal treatment with a potent statin” (atorvastatin 80mg/day), TC is 6.7mmol/L, LDL-C is 4.9mmol/L, HDL is 1.1mmol/L and TGs are 2.3mmol/L. What other agents should you try?
Mr JB is a very high-risk patient (please see Table 1). For secondary prevention in such very high-risk patients, the 2019 ESC/EAS guidelines recommend an LDL-C reduction of > 50% from baseline and an LDL-C goal of < 1.4mmol/L (please see Table 2). If LDL-C goals are not achieved with the maximum tolerated dose of statin, as is the case here, a combination of the statin with the cholesterol absorption inhibitor ezetimibe is recommended.
For secondary prevention, in patients at very high risk not achieving their goal on a maximum tolerated dose of statin and ezetimibe as was the case with our patient, Mr JB, a combination with a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor is now recommended. PCSK9 inhibitors target a protein (PCSK9) involved in the control of the LDL receptor. PCSK9 inhibitors are injectable drugs given subcutaneously every two or four weeks that have been shown to dramatically lower LDL-C levels.
These drugs are monoclonal antibodies, a biologic drug. PCSK9 itself inactivates the needed receptors on the liver cell surface that transport LDL into the liver for metabolism. Without these receptors, more LDL-C remains in the blood. So, by inactivating PCSK9 via inhibition, more receptors are available to capture LDL-C for metabolism and removal from the blood.
The European Medicines Agency and the US Food and Drug Administration have approved two monoclonal antibodies, evolocumab (Repatha) and alirocumab (Praluent) for the control of elevated plasma LDL-C. The efficacy of these agents at reducing LDL-C is in the range of 50-70%, independent of the presence of a background therapy (statins, ezetimibe, etc); data from trials suggest a reduction of CV events in line with the LDL-C reduction achieved.
People like Mr JB at very high total CVD risk and who in spite of “maximal treatment with a potent statin” still have persistently high levels of LDL-C should now be prescribed these drugs. However, for the moment, referral back to our local cardiology clinic was required for my patient as these agents are not available for prescription in general practice at present.
Case 4: A 60-year-old with type 2 diabetes
Ms RG is a 60-year-old lady with type 2 diabetes and no obvious complications. Diabetes control is good with metformin and diet. Her TC is 4.0mmol/L, LDL-C is 2.0mmol/L, HDL is 1.0mmol/L and TGs 3.4mmol/L in spite of “maximal treatment with a potent statin” (rosuvastatin 20mg/day). What might you do about the high triglyceride levels?
This case brings up the issue of the treatment of hypertriglyceridaemia, which is always controversial. According to the 2019 ESC/EAS guidelines, statin treatment is recommended as the first drug of choice for reducing CVD risk in high-risk individuals, such as our patient Ms RG, with hypertriglyceridaemia (TG > 2.3mmol/L). In high-risk (or above) patients with TG levels between 1.5 and 5.6mmol/L despite statin treatment, n-3 PUFAs (icosapent ethyl 2, 2g/day) should now be considered in combination with statins.
N-3 fatty acids reduce TGs, but their effects on other lipoproteins are trivial. The REDUCE-IT trial examined the effects of the impacts on CVD of adding the omega-3 fatty acid, icosapent ethyl in a dose of 2g bid in high-risk patients such as Ms RG, with raised TGs who were taking a statin.4
Over a median of 4.9 years, there was a significant (P < 0.001) 25% reduction in the composite primary outcome of CV death, non-fatal MI, non-fatal stroke, coronary revascularisation, or unstable angina, corresponding with an absolute reduction of 4.8%, which was offset by a 1% increased absolute risk of hospitalisation for atrial fibrillation or flutter. The US drug regulator, the Food and Drugs Administration, licensed this drug, now called Vascepa, for people with extremely high levels of triglycerides in 2018 but this preparation is not yet listed on MIMS Online Ireland.
Conclusion
If GPs, who after all manage the majority of patients with dyslipidaemias, are to do this effectively, we must be prepared to calculate the patient’s level of total CV risk, make management decisions based on LDL-C levels and titrate lipid-lowering therapy upwards until the recommended targets based on CV risk level are attained.
References
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J 2019 00, 1–78. https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehz455/5556353 (Last accessed 28/11/2019)
SLAN 2007. Survey of lifestyle, attitudes and nutrition in Ireland. Department of Health and Children, 2008. Published by the Stationery Office Dublin
Murphy C, Bennett K, Fahey T, et al. Statin use in adults at high risk of cardiovascular disease mortality: cross-sectional analysis of baseline data from The Irish Longitudinal Study on Ageing (TILDA). BMJ Open 2015;5: e008017. doi:10.1136/bmjopen-2015- 008017
Bhatt DL, Steg PG, Miller M, et al. REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med 2019; 380: 1122
 (click to enlarge)
(click to enlarge)