Most cases of red eye in general practice are not serious and the physician can often treat these with lubricants and sometimes with antibiotic drops and ointment. One can be more definite about the diagnosis of ‘bacterial conjunctivitis’ if there is a sticky or purulent discharge.
Most of these cases will heal quickly in a few days using topical antibiotic treatment. If there is a significant associated cellulitis of the eyelids then a course of systemic antibiotic treatment should be considered. Of course, one cannot be sure that a non-purulent discharge is not bacterial in origin, however a watery discharge is usually associated with viral aetiology.
It is rarely necessary to investigate the cause of the conjunctivitis by carrying out a swab and sending the sample for laboratory diagnosis. History-taking is, as always, very useful in determining the probable cause of the conjunctivitis. Adenoviral conjunctivitis often follows a history of pharyngitis and may occur in teachers or adults who work with children.
Pre-auricular lymph nodes are sometimes swollen and a little tender in this condition. The symptoms of this type of conjunctivitis often recur and sufferers tend to re-present with ongoing irritation of the eyes. Frequent application of lubricant drops will help the patient get through this period that is now non-contagious. Sometimes it takes a few months to settle completely and you probably will have asked for the help of an ophthalmologist after a few weeks. Occasionally, a short course of steroid drop treatment can be helpful but these cases are mainly managed by reassurance and ongoing lubricant support.
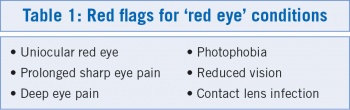
It is good to have a clear approach in your mind of how to deal with ‘red eye’. You don’t want to miss serious conditions. Ask yourself is this inflammation unilateral or bilateral? If it is obviously bilateral then you are probably not dealing with a ‘red flag’ condition (see Table 1) especially if it is not painful. However, if the redness is definitely uniocular and is painful then there is a good chance you have more than a simple conjunctivitis on your hands. Prolonged sharp pain, sometimes with photophobia, may indicate a keratitis of some kind and in your history you will probably have outruled a foreign body or trauma as the cause. Nevertheless it is good practice to instil a drop of proxymetacaine or other topical anaesthetic and use a fluorescein drop or strip to outline any significant corneal epithelial pathology. Don’t be surprised to find a corneal ulcer where there is obvious discomfort and pain.
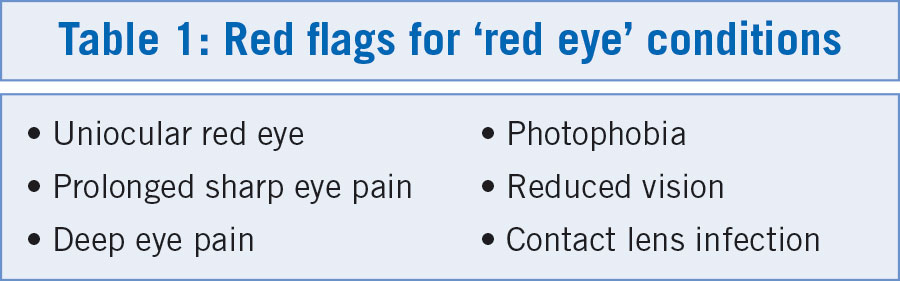
A corneal abrasion (see Picture 1) is also very obvious and it is very helpful to use a torch with a blue filter, the light from which excites the fluorescein and makes any defect in the corneal epithelium much more obvious. A magnifying loupe (see Picture 2) is also helpful, particularly for the older or long-sighted doctor.
(click to enlarge)
(click to enlarge)
Mild red eye
Dry eye
The most common presentation in general practice will be mildly red eye due to a reduced tear film. The symptoms can be very disconcerting to the patient and seem to be totally out of proportion with the severity of the condition. These cases will continue to present to you and it is important to have a basic knowledge of the composition of tears in order to treat dry eye with some measure of success.
The tears are made of a sandwich of water between a layer of oil at the front of the tear film and a layer of mucin at the rear. The layer of mucin which makes up 5% of the tear thickness allows the water element to slide easily over the hydrophobic epithelium. The water part of the tear film makes up 90% of the total tear thickness and the oil or lipid element covers the water layer anteriorly to prevent evaporation between each blink.
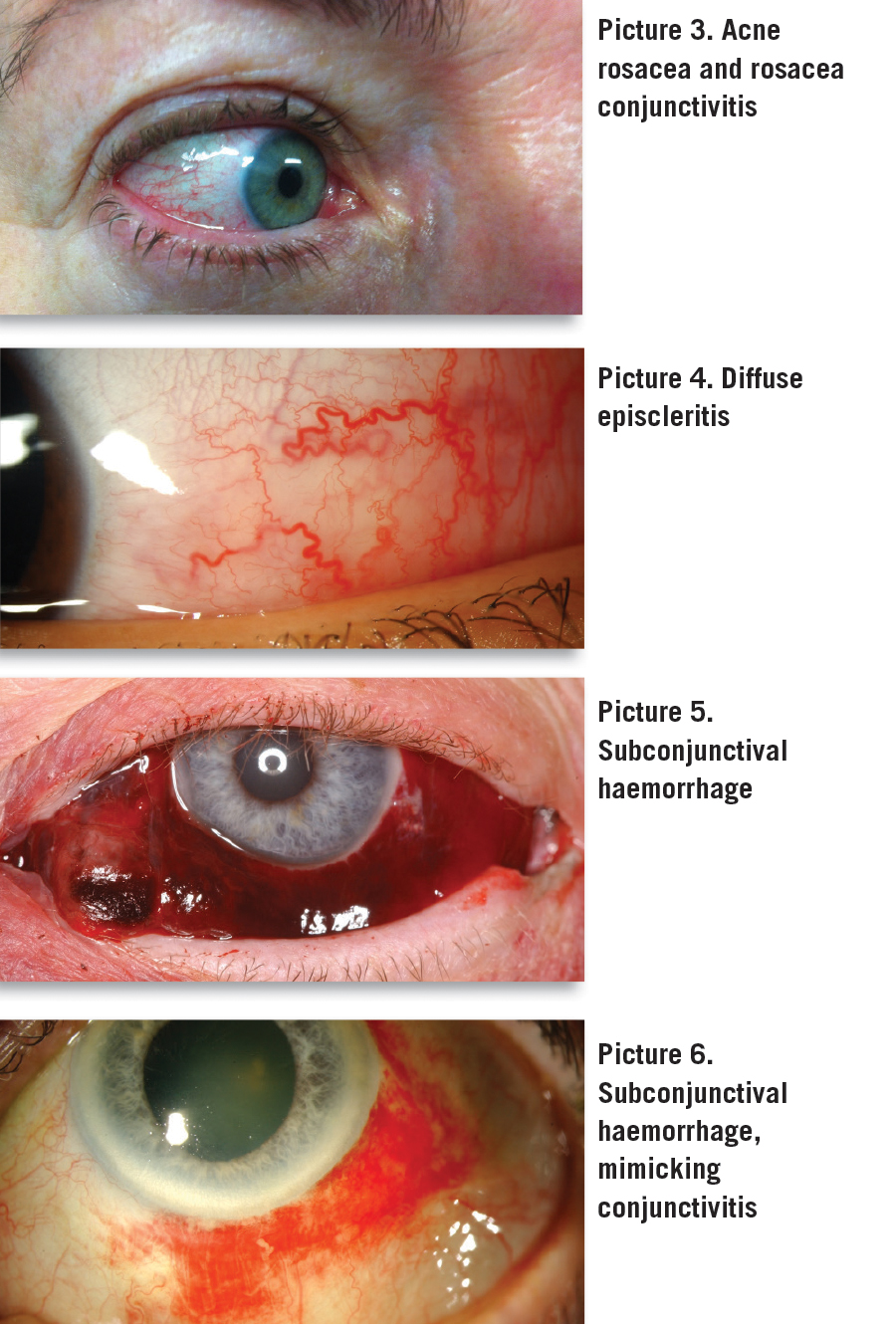
The oil layer makes up the final 5% of the total thickness of the tear film. You can make an estimation of the cause of the dryness in an individual patient by being observant. For instance, if there is even mild rosacea present (see Picture 3) then you can be sure that the lipid element of the tear film is deficient. Either there is not enough secretion from the meibomian glands or it is of poor quality, or often both, with the result that the lipid layer breaks up in a few seconds and the water evaporates making the eye very uncomfortable.
Blepharitis often accompanies this condition and lid hygiene and the use of antibiotic ointment for the eyelids can be beneficial in helping to treat the dry eye symptoms. To help these symptoms further you should prescribe an extended course of lubricant-containing oil such as Liposic eye gel (covered by GMS) or a lipid spray such as Actimist, Eye Logic or Murine Eye Spray (not covered by GMS).
The greater proportion of your patients presenting will have this type of tear problem as rosacea is a very common condition in Celtic races. Dry eye due to insufficient water volume is also quite common and many of your elderly patients will have this condition. The symptoms are more severe in patients with Sjogren’s syndrome and one should always enquire about other areas of the body such as a dry mouth, especially if the patient is of a younger age group.
There are many lubricants on the market that can be used as replacement tears and you are already familiar with many of them. It is best practice to avoid drops with preservatives, especially where frequent applications are desirable. Here are a couple of ‘top tips’:
When people use computers, tablets, or are reading or watching television they tend to blink less and if they have dry eyes their symptoms appear for the first time, or become worse, during these activities. You should explain this to them and encourage them to blink more often. They will blink automatically if they raise their eyes from the page and look around every so often, just for a short time before going back to the job on hand. The extra blinking will help keep their corneas moist.
Another helpful suggestion is to instil one drop into each eye from a preservative-free single dose unit (SDU) every 15 minutes. There are eight to 10 drops in these units, so one unit should last at least an hour. Of course these patients should discard any remaining drops when they have finished their activity. Suitable drops would be Artelac SDUs or Celluvisc 0.5% SDUs; both of these are covered by the GMS. There are many other lubricant SDUs on the market, for example Systane, Blink and others.
Most dry eyes are due to a deficiency in both the oil layer and the water layer and a combination of the treatments above should be recommended in many dry eye patients. Many ophthalmologists will agree that most patients with dry eye do not use lubricants often enough.
Dry eye due to mucin layer deficiency is much rarer and more problematic. It can cause filamentary keratitis which is a slit lamp diagnosis. Treatment for mucin layer deficiency includes acetylcysteine eye drops (Ilube – covered by GMS). If you have difficulty improving the symptoms of dry eye patients despite the use of copious lubricants then the insertion of punctal plugs may be necessary. These are placed in the lower puncta and reduce the drainage of tears from the eyes. Punctal cauterisation is an extra measure that may have to be resorted to in more extreme cases.
It is always important to consider systemic causes in the more persistent cases of dry eye, eg. Sjogren’s or other autoimmune conditions.
(click to enlarge)
Episcleritis
This is a benign condition characterised by a slightly painful and uncomfortable red eye where there is inflammation of the vessels of the episclera (superficial sclera). It is classified as either diffuse or nodular. The diffuse type (see Picture 4) is more commonly encountered and usually extends to a small area in the temporal part of the globe. However, it is occasionally more extensive, making the eye look ‘pink’ rather than ‘red’.
Although it appears very similar to mild conjunctivitis there is no involvement of the tarsal conjunctiva which will appear similar in colour to the other eye. The condition is often self-limiting and clears within a short period of time, not lasting much more than a few weeks. Occasionally this condition is more persistent. The treatment is supportive lubricant drops and sometimes mild steroid drops.
Nodular episcleritis, as the name suggests, is associated with a nodular swelling of the episclera which appears more intensely red than the immediate surrounding area. Again, despite its appearance, it is not usually painful. The aetiology is often idiopathic but up to a third of cases can be associated with systemic conditions. Investigations are not usually instituted unless the condition becomes persistent or recurs on a frequent basis.
Subconjunctival haemorrhage
This painless condition is not an inflammation but is so commonly experienced in general practice that it is worth mentioning here. The diagnosis is usually very obvious (see Picture 5) but if the bleeding is of low volume its appearance can mimic conjunctivitis (see Picture 6) and the use of a magnifier or a loupe during examination can be helpful.
The bleed usually clears within a week but occasionally is so extensive the haemorrhage can take up to two weeks to resolve. This condition is sometimes associated with hypertension but can also be brought on by coughing or sneezing or anything that increases pressure or congestion in the head from a Valsalva manoeuvre; for example straining during constipation.
Choking or vomiting are also associated with subconjunctival haemorrhages. The small conjunctival vessels are quite fragile and can bleed easily from rubbing the eye, especially if the patient is taking aspirin or some other blood thinner. Lubricant drops can be helpful especially if the haemorrhage is slightly bulky.
Allergic conjunctivitis
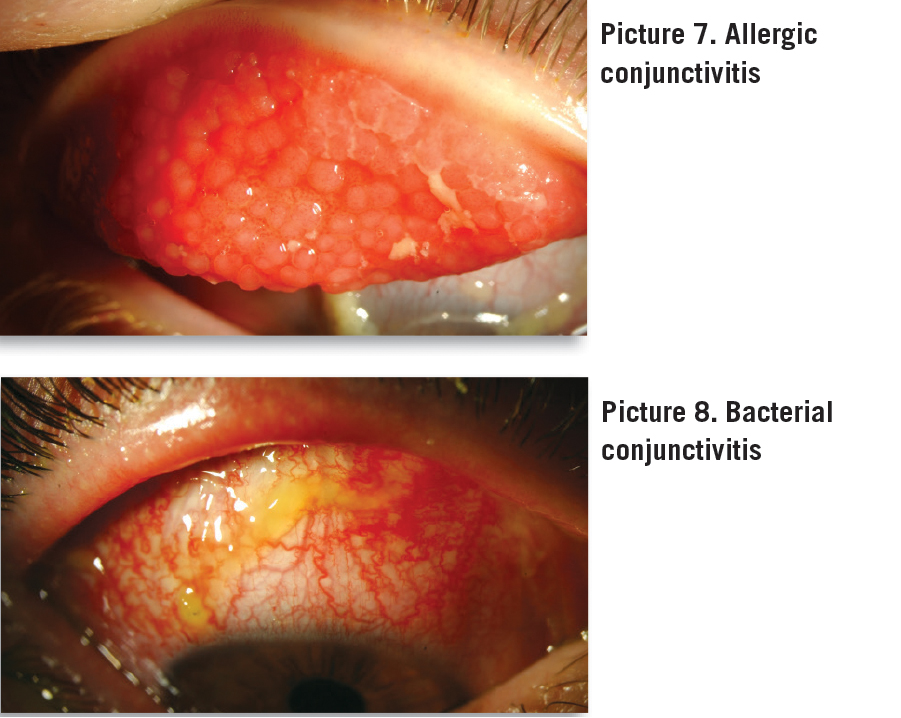
This condition is usually painless and normally presents with intense pruritus. Itchiness is the hallmark of this condition and if the patient does not complain of pruritus the redness is probably not due to allergic conjunctivitis. With your magnifying loupe you may be able to make out the follicular conjunctivitis that usually is present in allergic conjunctivitis (see Picture 7). This image shows large follicles under the upper tarsal plate, but follicles mainly occur in the lower conjunctival sulcus where they are smaller than the ones shown in this image.
Medical history often includes allergic rhinitis and asthma. Antihistamine drops such as emedastine (Emadine) can be very useful and are used on a PRN basis. Sodium cromoglycate (Opticrom) and olopatadine (Opatanol) eye drops act in a different way and can also work very well. Opatanol has antihistaminic effects as well as mast-cell stabilising properties. Opticrom has only mast-cell stabilising effects though it has a long record of success in allergic conjunctivitis. Both Opticrom and Opatanol need to be taken for at least one month, sometimes for the whole season and occasionally permanently.
(click to enlarge)
Moderately severe red eye
Keratoconjunctivitis sicca
When ‘dry eye’ becomes extra dry the surface of the cornea and conjunctiva can be become damaged. Injured epithelial cells will stain as tiny green punctate epithelial defects with fluorescein when illuminated with a blue light. It may be necessary to use a magnifier or a loupe to observe subtle changes which are obvious on slit lamp examination.
The symptoms are more severe than in mild dry eye situations and the treatment needs to be more intense with very frequent lubrication, and punctal plugs can help in many of these cases. One needs to be more aware of other diagnoses such as Sjogren’s syndrome, lupus erythematosus, pemphigus and other autoimmune conditions.
Acute follicular conjunctivitis
This term is used to describe a type of conjunctival reaction where there are small round collections of lymph cells in the tarsal conjunctiva that appear as small red bumps in the inside of the lids called follicles, similar but much darker red than the follicles of allergic conjunctivitis. These can be observed using a magnifier or loupe and a bright torch light. This is a reaction that occurs as a result of various assaults, most commonly adenoviral conjunctivitis, but also can occur in herpes zoster keratoconjunctivitis, infectious mononucleosis, Epstein-Barr viral infection or chlamydial eye infection.
Bacterial conjunctivitis
This conjunctivitis is quite common, especially in children, and is characterised by a mucopurulent discharge and a moderate to deep erythematous reaction in the lower conjunctival sulcus with a similar injection of the bulbar conjunctiva (see Picture 8). This infectious condition is usually bilateral although it can begin in one eye but spreads to the other within 24-48 hours.
(click to enlarge)
If the condition establishes itself in one eye only, then you should consider the presence of a foreign body or other focus of infection. The most common cause of this conjunctivitis is Staphylococcus aureus followed by Streptococcus pneumoniae and Haemophilus influenza. Other causes include Pseudomonas aeruginosa, Moraxella lacunata, Streptococcus viridans and Proteus mirabilis.
The conjunctivitis usually clears with antibiotic drops but if severe, a course of systemic antibiotics is indicated. Sufferers should not rub their eyes and should wash their hands regularly using their own towel or paper hand towels, which should be safely discarded. In certain demographics gonococcal conjunctivitis is relatively common and is recognised by a particularly purulent conjunctivitis in conjunction with a history of exposure.
This can potentially lead to serious, blinding infection of the cornea and should there be any suspicion, a conjunctival swab should be taken and the condition should be empirically treated with systemic antibiotics in accordance with the local protocol for the venereal variant of the disease.
Infected chalazion
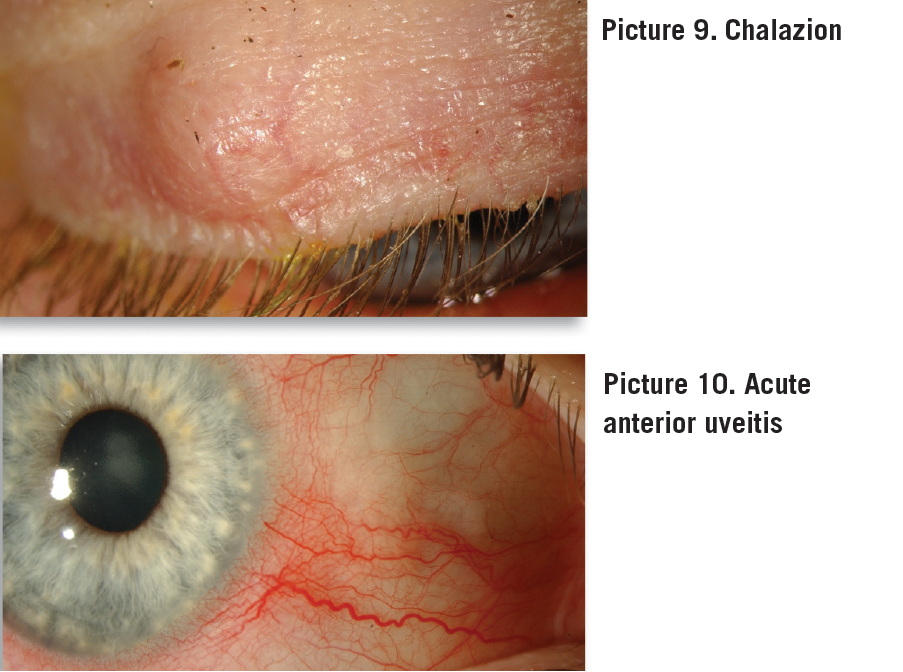
A meibomian cyst or chalazion is caused by blockage in the drainage duct of a meibomian gland while the gland continues to produce oil that then congeals and turns into a gel-like substance (see Picture 9). Sometimes this sequence can be accompanied by infection and abscess formation in the gland with surrounding cellulitis and eyelid swelling.
The acute situation requires immediate systemic antibiotics, antibiotic eye drops and frequent (three to four times a day) hot poultices. If there is no improvement in 24-48 hours “ubi pus ibi evacuate” which is a job for the ophthalmologist. Incision is usually carried out subtarsally.
Severe red eye (red flags)
Uveitis
Deep eye pain in association with red eye often points to uveitis, which is an inflammation of the uveal tract. The term uveitis covers iritis, cyclitis and choroiditis. There can be an associated vitritis and retinitis in some cases. If the anterior and posterior eye is involved the condition is known as panuveitis or diffuse uveitis which is not a common condition. Most cases of uveitis are confined to the front of the globe and may be referred to as anterior uveitis which is usually iritis but can also include extension into the ciliary body which is called cyclitis. Symptoms and signs include photophobia and deep pain with conjunctival and episcleral redness, often including circumcorneal injection (see Picture 10). The pain is more severe if cyclitis is present in which case circumcorneal injection will be more obvious. If the ciliary body is involved the visual acuity is more likely to be reduced due to the more intense inflammatory reaction.
(click to enlarge)
You will need the help of the ophthalmologist, especially if it is the first time the condition presents in an individual case. You will be familiar with the patients who have had this condition previously and they will also be aware when it recurs. It is important that treatment is commenced as soon as possible and steroid drops to reduce the inflammation are necessary to prevent the pupil margin adhering to the anterior lens capsule causing the development of posterior synechiae. Cycloplaegic eye drops such as cyclopentolate 1% are also important to reduce the pain and help prevent posterior synechiae.
When uveitis presents for the first time in a healthy person the condition is treated empirically and usually the condition is not investigated in depth. More than one episode should prompt a full search for the cause as uveitis can be associated with many systemic conditions and certain eye conditions. A careful family history followed by a full systems review may point the way for appropriate investigations in order to avoid a huge battery of blood tests and x-rays, many of them unnecessary.
Conditions that can be associated with uveitis include herpes simplex, herpes zoster, ankylosing spondylitis, brucellosis, sarcoidosis, inflammatory bowel disease, Bechet’s disease and several other conditions. It is important to take a history about back and joint pain in patients with acute uveitis as this can help identify patients with spondyloarthropathies in accordance with the international acclaimed Dublin Uveitis Evaluation Tool (DUET) that was developed by Prof Conor Murphy’s group at RCSI.
Acute angle closure glaucoma
Ruling out acute angle closure glaucoma is important as a differential diagnosis in red eye. The typical severe case of this condition is quite obviously due to ‘angle closure’ as the patient suffers much discomfort, the cornea is cloudy from oedema, the pupil is non-reactive, the eye is very red and rock hard to digital palpation. This is an acute emergency and needs immediate hospital treatment.
However, angle closure glaucoma can also present in a less acute form with intermittently raised pressure, not too much discomfort and some redness that could be mistaken for other conditions. Again, medical history is very helpful and if you ask appropriate questions the answers can steer you in the right direction.
There are two main groups of individuals who suffer from angle closure glaucoma. The most common presentation is in elderly people who have cataracts. The cataract swells and pushes the iris forward narrowing the drainage angle and causing the intra-ocular pressure to increase. If your patient has previously had cataract surgery then you can be confident that the red eye is not due to angle closure glaucoma as the artificial intra-ocular lens is much thinner and these cases have a deep anterior chamber.
The next time you receive a call to a nursing home for ‘conjunctivitis’ in an elderly patient be sure to have angle closure glaucoma foremost in your mind as the main differential diagnosis before arriving for the consultation. A good history and a careful examination will probably be all that is needed to out rule angle closure glaucoma, but if you are not sure of the diagnosis then an ophthalmologist’s opinion may be required.
The second group of individuals who suffer from acute angle closure glaucoma are typically long-sighted (hypermetropic) patients, usually female, who are middle aged. These cases are rare enough in an Irish population but they do occur from time to time. Hypermetropic eyes can be very short in length and the drainage angle is quite narrow in some individuals. Again, a very painful red eye which suddenly occurs is the usual presentation. However in some cases the pressure increases slowly without causing any symptoms. The patient becomes tolerant to the increase in intra-ocular pressure and if this is prolonged and not discovered, then optic nerve damage can result.
So while angle closure glaucoma is not an infection it is important to rule it out as a cause of acute red eye. It is worthwhile remembering that myopic (short-sighted) individuals are unlikely to experience acute angle closure because they usually have wide open angles due to the length of their eyes, which are longer than average.
It is useful to be able to tell the whether someone is short-sighted or long-sighted when attempting to outrule subacute angle closure glaucoma. A long-sighted person’s eyes will look magnified when wearing their distance glasses and a short-sighted person’s eye look smaller when they wear their distance glasses.
So a ‘top tip’ is to ask for the patient’s distance glasses (not reading glasses) and see if the glasses cause magnification or make things smaller when placed over an object. If the glasses cause ‘minification’ then it is unlikely that the owner would suffer from acute angle closure glaucoma.
Dendritic ulcer
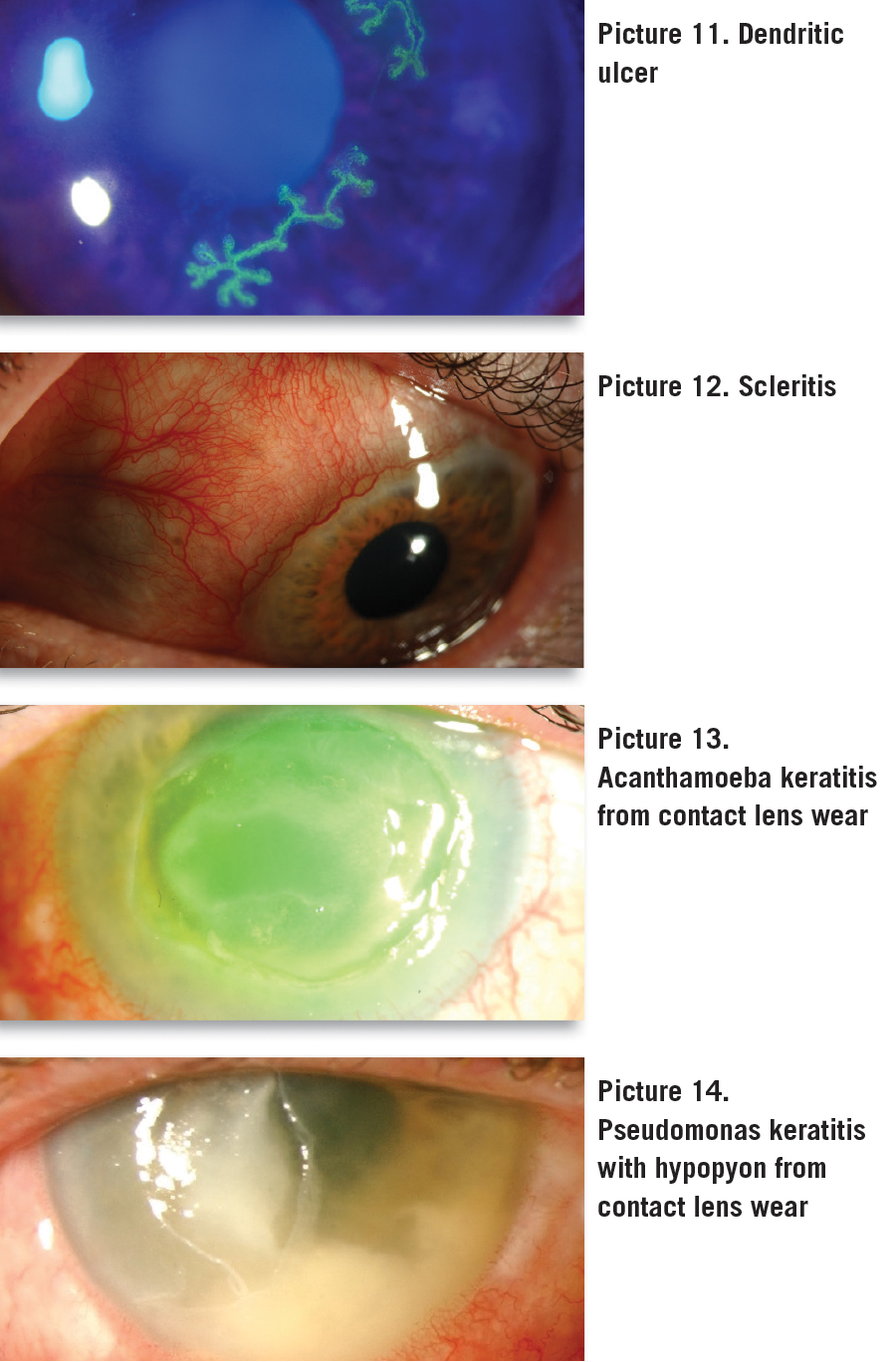
This is caused by herpes simplex infection of the corneal epithelium and displays the characteristic branch-like elongated ulcer (see Picture 11). Symptoms include a prolonged painful red eye with photophobia and occasionally blurred vision. It can be diagnosed by instilling an anaesthetic eye drop followed by fluorescein application which shows up this very obvious dendritic epithelial defect when illuminated by a bright blue light. Unless the condition is complicated it can be treated successfully by acyclovir eye ointment which should be instilled five times daily for 14 days.
Chronic recurrence can be complicated by herpes simplex uveitis and urgent treatment with systemic antiviral agents and sometimes steroid topical treatment is indicated. Occasionally ocular hypertension accompanies uveitis and this needs to be treated by temporary pressure-lowering drops to prevent secondary glaucoma. These cases will be attending an ophthalmologist and shared care with a GP is often instituted.
Scleritis
Scleritis is a rare and painful inflammation of the sclera. It is a serious eye condition that needs to be diagnosed and treated early to prevent visual loss. It can be differentiated from episcleritis by significant pain and tenderness with deeper redness due to the involvement of the scleral blood vessels (see Picture 12).
About half of the cases of scleritis are associated with systemic conditions such as connective tissue and autoimmune diseases and certain forms of vasculitis. Some cases of scleritis are idiopathic and others are caused by infections. In the unlikely event of coming across a case of scleritis, urgent referral is required.
Contact lens conditions
Beware of infections associated with contact lenses. Corneal infections from contact lens wear can occasionally be visually disastrous in young healthy adults who never had any eye problems previously. Contact lens hygiene is often very poor and most modern ‘sterilising’ solutions are almost useless. In the past, solutions such as isopropyl alcohol 20% and hydrogen peroxide 3%, when used in combination as a cleaning and storage solution guaranteed bactericidal and trophocidal outcomes. These solutions are almost never used nowadays because of the slight extra work involved in preparing the solutions and cleaning and rinsing the lens.
Most current ‘sterilising’ solutions are also used as wetting solutions. It doesn’t take much logic to work out that if you can put the solution into your eye without adverse effects it couldn’t be killing too many bacteria or acanthamoeba. The result of poor contact lens hygiene is that occasionally infective keratitis will occur. Sudden deterioration of acanthamoeba keratitis (see Picture 13) or pseudomonas keratitis (see Picture 14) occurs occasionally causing severe pain and a sharp drop in vision.
Pseudomonas keratitis is particularly jeopardous because even as little as 12 hours before severe damage occurs to cornea, the condition may look fairly benign. Sometimes the loss of vision is permanent due to corneal scarring and eventual corneal transplantation is occasionally indicated. GPs should never put themselves in the position where they take medical responsibility for contact lens infections. Urgent referral to an ophthalmologist is always the safest strategy in a contact lens wearer who develops a red or painful eye.
Garry Treacy is an ophthalmologist and director of Medical Optics Community Eye Clinics based in Bray, Co Wicklow and in Fairview, Dublin. www.medicaloptics.ie
The author would like to thank Prof Conor Murphy and Dr Marylyn Harris for supplying most of the images used in this article.
 (click to enlarge)
(click to enlarge)