Systemic lupus erythematosus (SLE) is a systemic autoimmune disease with a broad spectrum of clinical manifestations. It can affect nearly every organ and tissue. Monitoring patients with such a complex disease can be challenging. There is great variability in the ways clinicians can assess patients with SLE and evaluate their progression over time, especially when assessing organ involvement.1
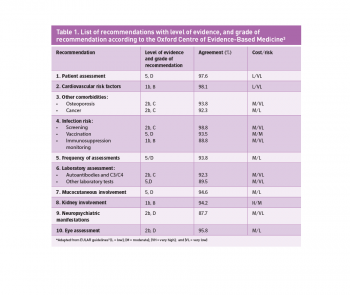
The European League Against Rheumatism (EULAR) published recommendations in 2010 for monitoring patients with SLE.2 Their aim was to develop a standardised set of variables and key points, which would help to unify the assessment of patients with SLE. A multidisciplinary panel elaborated the guidelines and graded the evidence and level of recommendation according to those proposed by the Oxford Centre for Evidence-Based Medicine.3 For each recommendation, the panel approved percentage rate and the estimated cost/benefit rate is included (see Table 1). The guideline includes a total of 10 recommendations for the clinical evaluation of patients with SLE (see Table 1). The aim of this article is to summarise the most relevant information contained in these guidelines emphasising key aspects for optimal assessment of these patients.
(click to enlarge)
General assessment and frequency
The most important aspects to consider when assessing patients with SLE are disease activity, organ damage, quality of life and drug toxicity.4 The clinical presentation of SLE may be influenced by each of these factors independently.
Disease activity
Using one of the validated indexes that assess disease activity, such as the British Isles Lupus Assessment Group (BILAG), the European Consensus Lupus Activity Measurement (ECLAM) or Systemic Lupus International Collaborating Clinics Damage Index (SLICC/ACR), may assist in obtaining a complete picture of the patient’s clinical status. However, there is concern regarding the feasibility of performing such complex indexes in everyday practice due to lack of time or resources. Therefore, routine assessment of disease activity can be made using any validated index and/or a physician global assessment on a scale from 0 to 3.
Organ damage
Organ damage should be evaluated annually by using the SLICC/ACR Damage Index.2
Quality of life
Assessing quality of life (QoL) is complex, subjective and variable, therefore the panel agreed on grading the quality of life from 0-10 using the visual analogue scale (VAS) or by taking in to account the patient’s own impression at every visit. More complex indexes such as the SF-36 have a role in facilitating comparison between centres in observational studies. Administration of these questionnaires in routine clinical practice is unlikely to be feasible.
Drug toxicity and comorbidities
It is equally important to monitor drug toxicity and comorbidities on a routine basis in patients with SLE. A complete list of the patient’s medications should be recorded on every visit to prevent drug interactions.
Follow-up visits
There is no solid evidence with regards to how frequently these patients should be followed up (see Table 1). Six to 12 months’ assessments are advised for patients without signs of disease activity, damage or comorbidity.
Cardiovascular risk factors and comorbidities
There is a well-known association between cardiovascular disease (CVD), premature atherosclerosis and SLE.5 Hypertension and dyslipidaemia are more prevalent in patients with SLE. CVD is an important cause of morbidity and mortality in these patients.6 Furthermore, there is solid evidence (see Table 1) for monitoring patients with SLE for CV risk factors.
EULAR recommends documenting smoking status, prior vascular events, level of physical activity, hormonal therapies and family history of CV disease at the initial visit. It is also recommended that patient BMI or waist circumference and fasting lipid and glucose are monitored initially and yearly thereafter.2 Patients who are receiving long-term glucocorticoids may require more frequent assessment as they are at increased risk of CVD.
Patients suffering from SLE are at increased risk of other comorbidities. Of these, osteoporosis and cancer feature in the EULAR recommendations. Osteoporosis can cause a significant problem in patients with SLE, in particular among patients on long-term steroid treatment and postmenopausal women.7 All patients with SLE should be advised to optimise calcium and vitamin D intake, to exercise regularly and to stop smoking. They should be screened and followed for osteoporosis according to local guidelines.2
Cancer incidence is increased in patients with SLE, particularly haematological malignancies (non-Hodgkin lymphoma), cervical cancer (cervical intraepithelial neoplasm), breast cancer and lung cancer. However, these patients tend to be screened less often than the general population.8 EULAR advises that patients with SLE should undergo cancer screening at the minimum according to local guidelines (for example mammograms, cervical smears and assessment of faecal occult blood).2
Infection risk
Infections are a major cause of death in patients with SLE. Although there isn’t an increased incidence of HIV, hepatitis B or hepatitis C infection in these patients, natural evolution of disease and concomitant immunosuppressive therapy can lead to increased risk of reactivation of these conditions. Screening for HIV, HBV and HCV in SLE patients should be based on the patient’s baseline risk factors, and is highly recommended before starting immunosuppressive (IS) drugs or high-dose steroids. Tuberculosis testing is not recommended as routine in non-endemic areas but should be performed before starting IS treatment or high-dose steroids.
CMV infection is common in immunosuppressed patients and may mimic active SLE, so testing for CMV (antigenaemia) should be considered in selected cases, particularly patients with active disease undergoing therapy with high-dose glucocorticoids. Infection prevention is equally important in patients with SLE. Pneumococcal and influenza vaccinations are safe and effective. They should be considered for those on IS drugs, administered if possible when the SLE is inactive. Attenuated live vaccines, on the other hand, are contraindicated in patients in IS drugs or high-dose steroids. However, there is a lack of evidence based recommendations with regards to vaccinations among SLE patients (see Table 1).
Finally, is it important to identify those at high risk of opportunistic infection by monitoring neutrophil count (< 500/mmc), lymphocyte count (< 500/mmc) and serum immunoglobulin subset G (< 500mg/dl) at each visit.
Laboratory assessment
The production of autoantibodies is a key immunological feature of SLE and is a basic part of the diagnostic and prognostic evaluation of these patients. Determination of autoantibody levels may have prognostic value and predict certain organ involvement or disease flares:10
Antinuclear antibodies (ANA) are present in 95% of SLE patients and are diagnostic criteria for SLE
Anti ds-DNA are also diagnostic of SLE and titre changes correlate with disease activity and damage development
Anti-Ro, anti-La and anti-ribonucleoprotein (RNP) antibodies may have prognostic value in SLE. Anti-Ro/Sjögren syndrome antigen A (SSA) and anti-La (SSB) antibodies have been associated with the occurrence of neonatal lupus
Anti-phospholipid (aPL) antibodies have been associated with general disease activity, thrombotic manifestations and the development of organ-damage as well as pregnancy complications.
Based on these findings, EULAR recommends assessment of the following:2•
Baseline monitoring – ANA, anti-dsDNA, anti-Ro, anti-La, anti-RNP, anti-Sm, aPL, C3, C4 (complement levels are associated with active disease)
Re-evaluation in previously negative patients – aPL, Anti-Ro and anti-La Anti-dsDNA, C3, C4 if the situations as listed above arise
Patients with inactive disease – although there is controversy in this particular case (see Table 1), the panel agreed on performing complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), serum albumin, serum creatinine (or eGFR), urinalysis and urine protein/creatinine ratio every six to 12 months.
Mucocutaneous involvement
Mucocutaneous manifestations are common in SLE, and may occur in approximately 80% of patients.11 They are classified histopathologically as SLE-specific and SLE-non-specific skin lesions. However, the diagnosis of cutaneous manifestations in SLE may be difficult, as many conditions and adverse drug reactions may mimic SLE. Difficult or unclear cases should be referred to dermatology and might require skin biopsy to clarify aetiology. The Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI)2 can be helpful to assess cutaneous disease activity and damage and could be considered in clinical practice in patients with extensive cutaneous manifestations.
Kidney disease
Renal involvement is common in patients with SLE and it is an important cause of morbidity and mortality. Up to 25% of patients may develop renal insufficiency and end-stage renal disease (ESRD) despite receiving treatment. Some biochemical markers (serum creatinine, urine sediment analysis, proteinuria) and blood pressure have a predictive value for the presence and outcome of kidney involvement and the occurrence of flares.12 There is strong evidence that recommends serial assessment of renal involvement in patients with SLE (see Table 1):
Patients with a persistently abnormal urinalysis or raised serum creatinine should have urine protein/creatinine ratio (or 24-hour proteinuria), urine microscopy, and be considered for renal ultrasound and biopsy
Patients with established nephropathy should have protein/creatinine ratio (or 24-hour proteinuria) and immunological tests (C3, C4, anti-dsDNA), urinary sediment microscopy and blood pressure at least every three months for the first two to three years
Patients with established chronic renal disease (eGFR < 60ml or stable proteinuria > 0.5mg/24 hours) should be followed according to the National Kidney Foundation guidelines for chronic kidney disease.
Neuropsychiatric manifestations
Neurological involvement (central, peripheral or autonomic) occurs frequently in patients with SLE. Prevalence is very variable in the literature; headaches, mood disorders, seizures, cognitive impairment (CI) and cerebrovascular disease are the most frequent manifestations.13
Patients should be monitored for the presence of neuropsychological symptoms by means of medical history and physical examination. Cognitive impairment should also be assessed by evaluating attention, concentration, word finding and memory difficulties.
Eye assessment
Antimalarial drugs such as hydroxychloroquine (Plaquenil) are widely used in SLE management and have a relatively low risk of retinopathy (0.5%).14 A baseline eye examination is recommended before starting therapy with antimalarial drugs. Thereafter, in low-risk patients, no further testing is required for the next five years. After the first five years of treatment, eye assessment is recommended yearly. In high-risk patients, an eye assessment is recommended yearly.2 Systemic glucocorticoids can cause cataracts and increase intraocular pressure favouring the development of glaucoma. A baseline eye examination is recommended in patients taking glucocorticoids, and should be repeated in follow-up visits in patients with high risk of developing these complications. In conclusion, if symptoms develop suggesting eye involvement by lupus, patients should be referred to ophthalmology.
Conclusion
Patients with SLE require periodic and extensive assessment to prevent the development of complications, minimise drug toxicity and improve therapy response and clinical outcome. The EULAR recommendations for clinical monitoring provide an evidence-based practical guide to help clinicians optimise their assessment and follow-up of patients with SLE. There is solid evidence to support monitoring patients with SLE for CV risk factors and renal involvement.
The EULAR guidelines highlight the importance of autoantibody screening and thorough assessment for other comorbidities and signs of immunosuppression. However, other aspects, such as the frequency of assessments, vaccinations or the use of other routine laboratory tests in SLE patients are still controversial and may require further investigation.
References
Demas KL, Costenbader KH. Disparities in lupus care and outcomes. Curr Opin Rheumatol 2009; 21: 102–109
Mosca M, Tani C, Aringer M et al. European League Against Rheumatism recommendations for monitoring patients with systemic lupus erythematosus in clinical practice and in observational studies. Ann Rheum Dis 2010; 69(7): 1269-1274
Centre for Evidence-Based Medicine. EBM Tools. Finding the Evidence. Levels of Evidence. University of Oxford, 2001.
Strand V, Gladman D, Isenberg D et al. Outcome measures to be used in clinical trials in systemic lupus erythematosus. J Rheumatol 1999; 26: 490–497
Manzi S, Selzer F, Sutton-Tyrrell K et al. Prevalence and risk factors of carotid plaque in women with systemic lupus erythematosus. Arthritis Rheum 1999: 42: 51- 60
Doria A, Iaccarino L, Ghirardello A et al. Long-term prognosis and causes of death in systemic lupus erythematosus. Am J Med 2006; 119: 1497-1499
Becker A, Fischer R, Scherbaum WA, Schneider M. Osteoporosis screening in systemic lupus erythematosus: impact of disease duration and organ damage. Lupus 2001; 10: 809- 814
Bernatsky SR, Cooper GS, Mill C et al. Cancer screening in patients with systemic lupus erythematosus. J Rheumatol 2006; 33: 45–49
Erdozain JG, Ruiz-Irastorza G, Egurbide M et al. High risk of tuberculosis in systemic lupus erythematosus? Lupus 2006; 15: 232–235
10. Bertsias G, Ioannidis JP, Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics et al. EULAR recommendations for the management of systemic lupus erythematosus. Report of a Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics. Ann Rheum Dis 2008; 67: 195–205
Rothfi eld N, Sontheimer RD, Bernstein M. Lupus erythematosus: systemic andcutaneous manifestations. Clin Dermatol 2006; 24: 348–362
Williams RC Jr, Harmon ME, Burlingame R et al. Studies of serum C-reactive protein in systemic lupus erythematosus. J Rheumatol 2005; 32: 454–461
Hanly JG, Urowitz MB, Sanchez-Guerrero J et al. Systemic Lupus International Collaborating Clinics. Neuropsychiatric events at the time of diagnosis of systemic lupus erythematosus: an international inception cohort study. Arthritis Rheum 2007;56:265–73.
Mavrikakis I, Sfi kakis PP, Mavrikakis E et al. The incidence of irreversible retinal toxicity in patients treated with hydroxychloroquine: a reappraisal. Ophthalmology 2003; 110: 1321–1326
 (click to enlarge)
(click to enlarge)