A new model of care outlines proposals for a radical change in the way patients with urological conditions are managed, promoting a more community-based approach
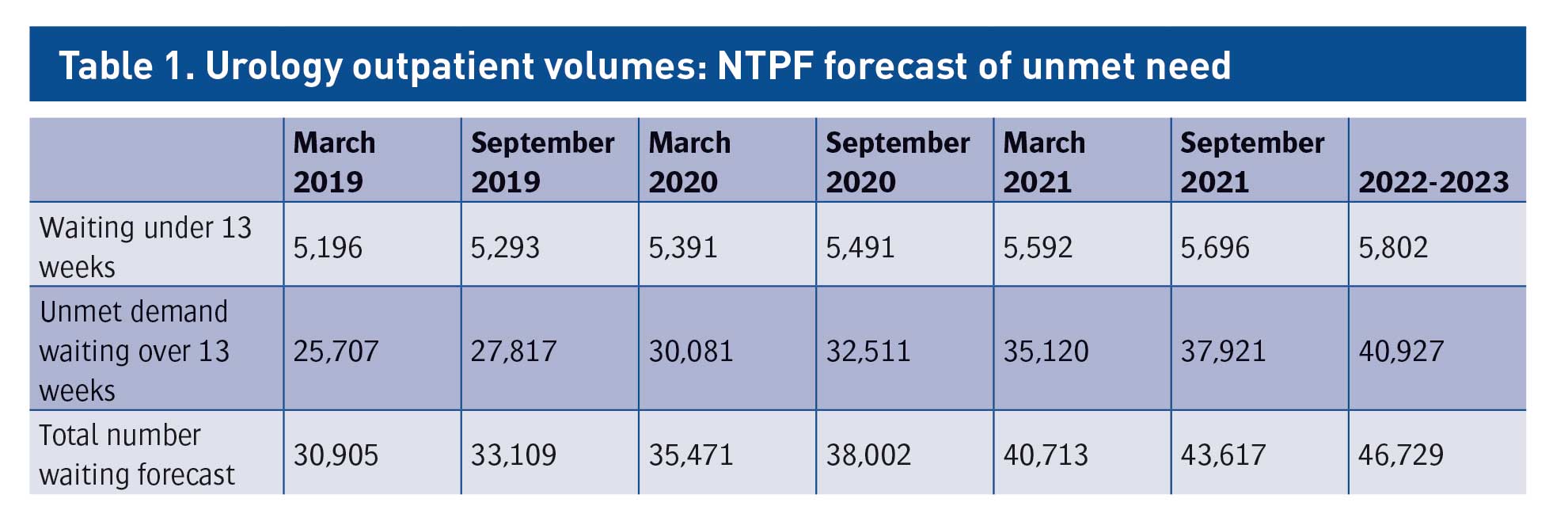
At present, urology is the fourth busiest surgical discipline in Ireland on the basis of surgical discharges. As at March 2019, 30,905 patients were waiting to see a urologist at an outpatient clinic, a figure that is expected to rise over the coming years. To help address this unmet need and shorten waiting lists for urological services, the National Clinical Programme in Surgery (NCPS), in partnership with the RCSI and Acute Operations HSE, has launched a new model of care for the treatment of urological conditions. Urology: A model of care for Ireland outlines a radical change in the delivery of urology care so that the majority of patients are cared for in the community, in local primary care centres or in their local hospital.
NCPS clinical advisor in urology Mr Eamonn Rogers, who was commissioned by the HSE to undertake this work, said: “The frequency of urinary symptoms and pathology increases with age. Ireland’s changing demographics mean that a radical reconsideration of how best to deliver urology services is necessary.
“This model of care must be implemented in full so that we can deliver an efficient and economically viable service which improves the access of patients across Ireland to the services they require as they get older, delivered by a range of healthcare providers including general practitioners, physiotherapists, and clinical nurse specialists, advanced nurse practitioners, physician associates and urologists.”
Service gaps
Not only is the demand for urology services growing, the pattern of disease is changing. There has been a reported increase in the prevalence of urinary incontinence in patients over the age of 50 in Ireland while the incidence of prostate disease is rising sharply, according to the model of care, with requests for prostate-specific antigen (PSA) tests generating a further demand for
urology services.
Increasing cancer survivorship is adding to the burden as urological expertise is required in the rehabilitation of incontinence and sexual dysfunction and the management of radiation comorbidities such as haematuria.
The model of care also deals with the changing face of the specialty and the move away from traditional surgery towards the use of medication as a first-line treatment in conditions such as erectile dysfunction, benign prostatic hyperplasia (BPH), urinary tract infections and urinary incontinence. Where surgery is recommended, procedures tend to be minimally invasive, meaning there is less open surgery taking place.
The model describes the current capacity of urology services as inadequate, stating that existing ways of working within the specialty are insufficient and are resulting in longer waiting lists for outpatient ambulatory and scheduled care. Projections made using data from the National Treatment Purchase Fund (NTPF) are referred to in the model under the section heading ‘Current scale of the problem’ and adapted here in Table 1. They reflect, according to the authors, the unmet needs of many urology patients in Ireland and represent an immediate challenge to which the current service provision is unable to rise.
(click to enlarge)
Identifying problem areas
The stated aim of the model is to establish a system of urology care that serves more patients in the community, while ensuring that appropriate clinical governance remains in place to support a safe, high quality service.
The authors set about gauging the appetite for change within Ireland’s urological community by referring to an Irish Society of Urology (ISU) survey of consultant urologists conducted in 2016 wherein respondents identified their main concerns in relation to the specialty. These concerns were later ranked by the authors of the study in order of priority and organised into two categories – inpatient care and outpatient care.
The top priorities for inpatient care were found to be:
Dedicated urology theatre for inpatient treatment
The creation of a hub and spoke model between Model 4 (hub) and Model 3 (spoke) hospitals
The development of robotic surgery.
The top priorities for outpatient care were found to be the development of:
Rapid access haematuria clinics
Nurse-led urology clinics
Shared care initiatives between primary care and
urology departments in hospitals.
The model establishes the prevalence of various presenting symptoms for which patients are regularly referred to a urology outpatient department. It cites a 2017 study which identified haematuria, male lower urinary tract symptoms (LUTS) and urinary infection with/without urinary incontinence as the three most prevalent presenting symptoms among a sample of 1,000 patients at an Irish Model 3 hospital. A similar study carried out in the same year by the same hospital group at a Model 4 hospital found the same three conditions to be most prevalent, once urological cancers were excluded.
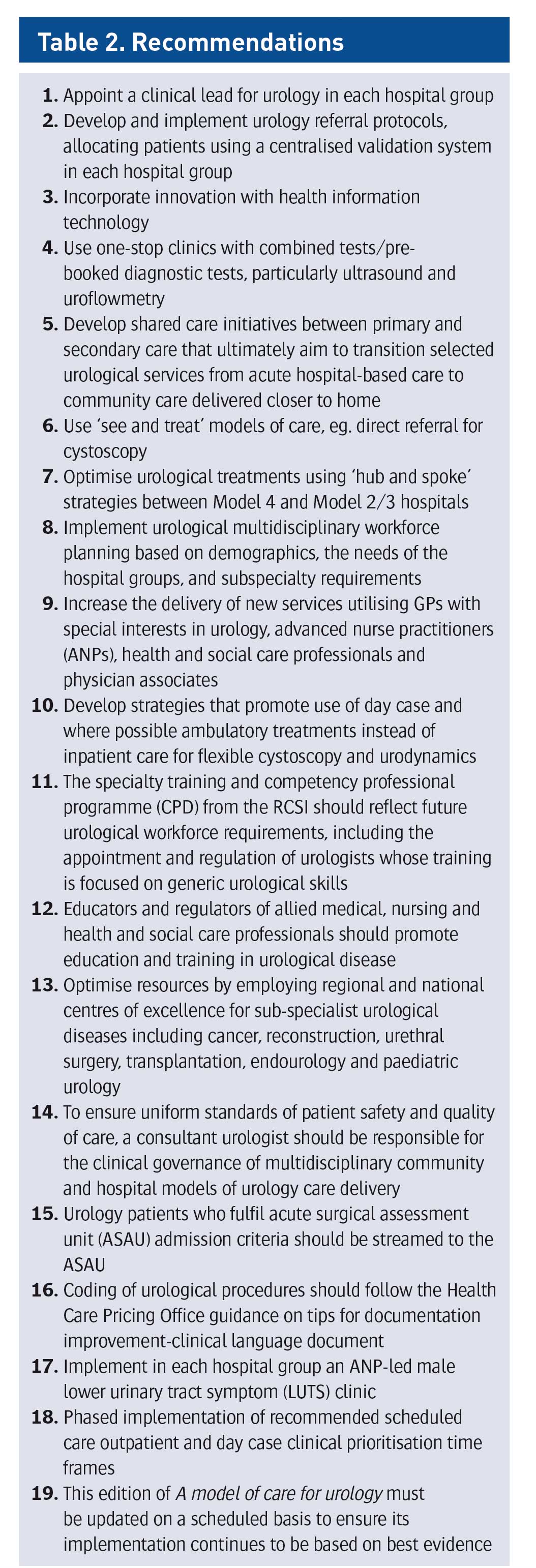
By identifying these areas of greatest demand, the authors believe that devising new strategies and pathways targeting these conditions will prevent patients from requiring hospital access, thus expediting the management of the majority of urological patients awaiting outpatient appointments.
(click to enlarge)
Specific pathways
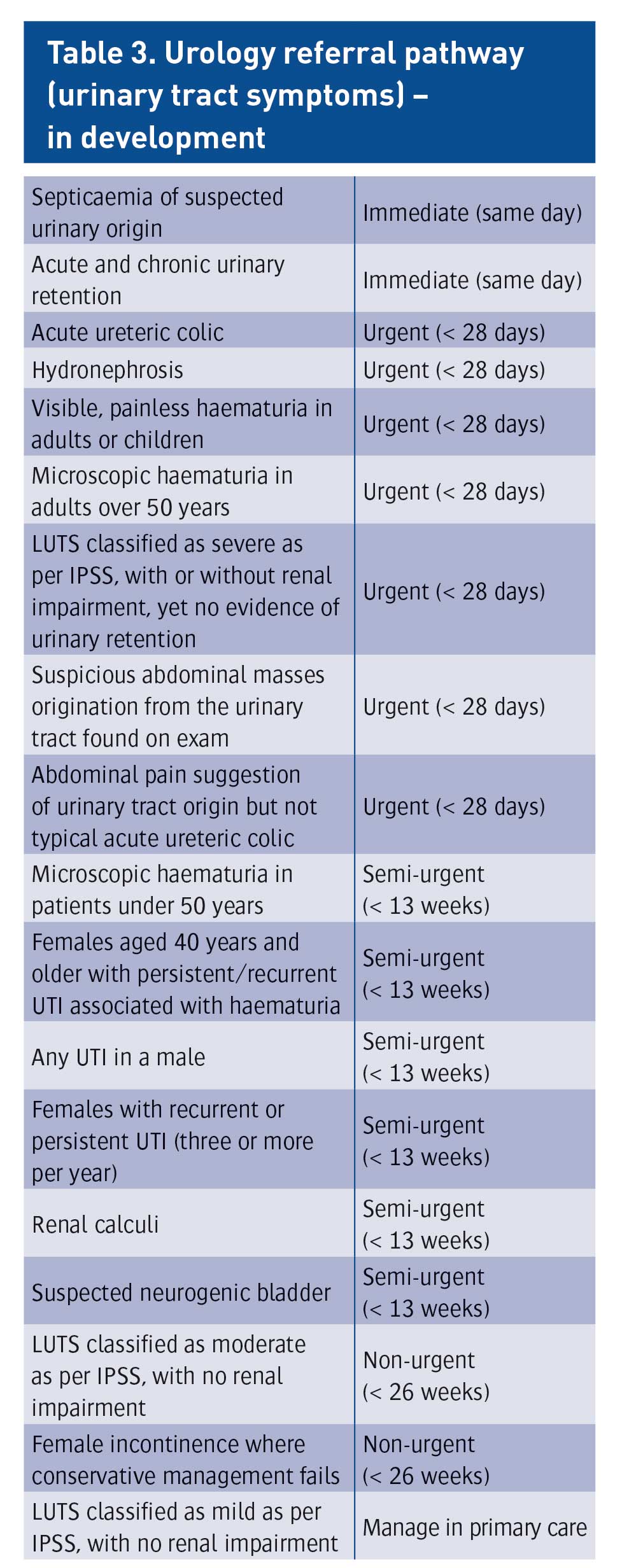
This section deals with various initiatives, either in operation or in development, designed as direct responses to the recommendations. It includes a urology referral pathway that classifies symptoms based on clinical priority and recommended timeframe (see Table 3). This pathway, in outlining aspirations for treatment and review times, reflects the need for a reorganisation of service delivery, according to the model. It also notes that all trauma should be classified as immediate (same day).
(click to enlarge)
LUTS
The pathway for the care of patients with LUTS represents recommendation 17 in action (implement in each hospital group an ANP-led male LUTS clinic) and aims to reduce these patients’ need for hospital access, as well as waiting times for assessment. Based on the use of the International Prostate Symptom Score (IPSS), this shared-care initiative sees patients undergo assessment and prostate exam in primary care and lab tests to assess for prostate cancer, renal impairment and haematuria. If an abnormality is flagged in any of these tests, the patient is not enrolled in the initiative. The initiative uses the IPSS to triage patients who require hospital access. All that is required for the establishment of such a clinic, according to the model, is an ANP, a clinic room with toilet access and an examination couch, as well as additional supports such as GP blood tests and access to booking and reviewing of radiology and lab results.
This section expands on recommendation 7 (optimise urological treatments using ‘hub and spoke’ strategies between Model 4 and Model 2/3 hospitals), highlighting the importance of embracing new technologies that show equivalence with transurethral resection of the prostate (TURP), the current ‘gold standard’ in the surgical management of BPH, and the need for the development of a national policy for the insertion of suprapubic catheters where urethral catheters are contraindicated. Such procedures are subject to strict guidelines and are therefore not suitable for use in the community.
Haematuria
Blood in the urine, whether visible or microscopic, is one of the most prevalent presenting symptoms among patients attending outpatient clinics in Ireland, according to the model, with 13% of the HSE waiting list accounted for by patients with haematuria. As such, the NCCP and the NCPS have developed an initiative described in the model as “a standardised network of ‘one-stop’ rapid access haematuria pathway (RAHP)”. Reflective of recommendation 4 (use one-stop clinics with combined tests/pre-booked diagnostic tests, particularly ultrasound and uroflowmetry), the RAHP is to focus on visible frank haematuria and will have a presence at one site per hospital group. The pilot site for this initiative is Roscommon University Hospital. The RAHP aims to provide access to diagnostics for patients who have symptoms of haematuria with procedures and investigations carried out within 28 days. The RAHP clinics are one of the key improvement initiatives described within the new model. This pathway involves:
The patient attending for their ‘see and treat’ appointment as a day-case, avoiding attendance at outpatients altogether
Access to the most appropriate diagnostic imaging test (ultrasound or CT)
Access to cystoscopy
Clinical review with the cross-sectional imaging report and discharge or referral on to an appropriate service
Follow up MDTs to discuss the management of patients with cancer.
It is hoped that results from the pilot will provide evidence that this pathway will reduce patient waiting times, increase early diagnosis, improve communication with GPs and ultimately ease the burden on outpatient departments and Model 4 cancer centres.
Other pathways
This section of the model of care addresses a continence care pathway aimed at assessing incontinence in primary care and referring patients to a nurse-led one stop clinic for management and follow up.
A scrotal care pathway is also described, in which the importance of timely access to diagnostic ultrasound is stressed, and the availability of such a screening tool in the community is recommended to reduce the burden on outpatient clinics.
A section dealing with sub-specialties describes initiatives aiming to improve the management of patients with urological cancers, highlighting key points of the National Cancer Strategy 2017-2026 such as prioritising prevention, increasing symptom awareness and early diagnosis.
Further reading
The model of care, including the tables adapted here, is available in full at www.hse.ie
Reference
National Clinical Programme in Surgery 2019. Urology: A model of care for Ireland. Available at www.hse.ie
 (click to enlarge)
(click to enlarge)