Pancreatic adenocarcinoma (PDAC) is the fourth leading cause of cancer related mortality in the US and Europe.1 The five-year survival rate remains less than 10%, with minimal improvements observed in the treatment of the disease over the last 20 years 2.
The insidious nature of the disease and vagueness of associated symptoms mean that most patients present with metastatic or locally advanced disease at the time of diagnosis, excluding safe or complete surgical excision of the disease. Patient performance status and clinical condition often deteriorates rapidly, allowing a sense of nihilism outside of specialist centres. The average life expectancy for patients diagnosed in the UK is limited to three to six months.
Unintentional weight loss is a prominent feature of pancreatic cancer; over 80% of patients report weight loss at the time of diagnosis, with more than one-third experiencing weight loss in excess of 10%.3 Continued, persistent weight loss during treatment has been shown to be an adverse prognostic factor,4 impacting both survival duration and patient-reported quality of life (QOL).5 Progressive, intractable weight loss has been described as one of the most distressing and intractable features of PDAC.6 Despite this, weight loss may be missed or under-reported. Patients with pancreatic cancer are increasingly presenting with a normal BMI despite experiencing significant weight loss, delaying diagnosis and treatment.
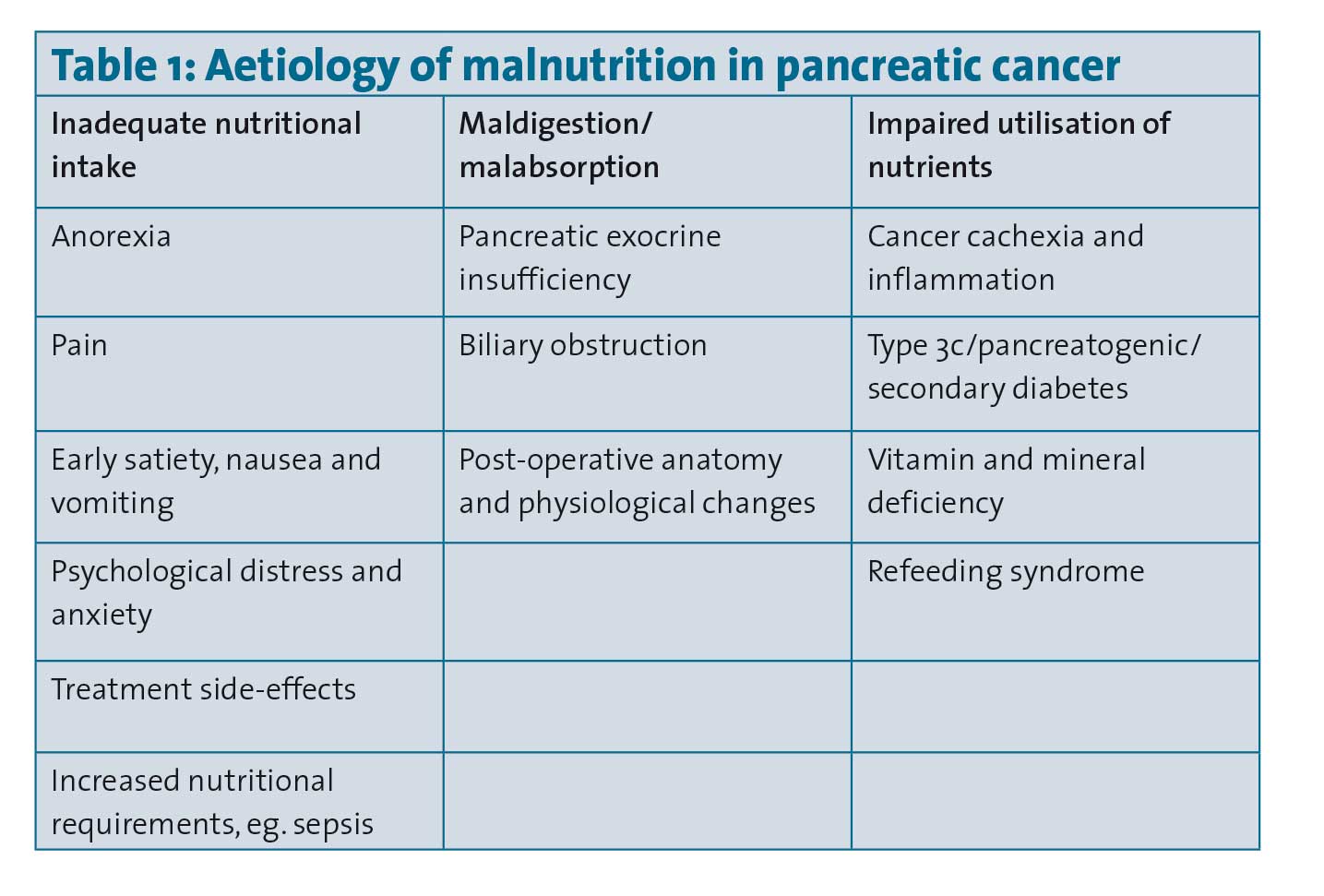
Weight loss and malnutrition in PDAC are caused by many factors (see Table 1), which often occur in combination, including anorexia, cancer cachexia, pancreatic exocrine insufficiency (PEI), obstructive jaundice and gastric outlet obstruction. For many patients, these will be further amplified by treatment-related side-effects.
(click to enlarge)
Treatment strategies for malnutrition in pancreatic cancer
It has been recommended that all patients with pancreatic cancer should be seen by a specialist dietitian.6 Dietetic-led interventions in PDAC have been shown to improve weight,5 patient QOL,7 and survival.5 Moreover, the delay or lack of dietetic referral was highlighted as the primary unmet supportive care need among patients and/or their bereaved carers.8
Recent ESPEN consensus guidelines for nutrition in cancer patients recommend daily energy intakes between 25 to 30 kcal/kg/day, and a minimum protein intake of at least 1g/kg/day, ideally aiming for 1.5g/kg/day.9 Individualised patient counselling regarding meal frequency, food choice, distribution, use of PERT and nutritional supplements is needed to achieve this in the context of multiple barriers to adequate nutritional intake and/or absorption.
Pancreatic exocrine insufficiency
PEI, a functional limitation of pancreatic enzyme secretion,10 is a common complication of PDAC which results in malabsorption and malnutrition, and affects 80-90% of patients. The risk of PEI is increased by the proximity of tumour to the duodenum, post-pancreatic surgery, and in head of pancreas lesions where 85% causing main pancreatic duct obstruction.11 PEI negatively impacts quality of life,12 and is associated with poor survival.13
Patients with PEI experience significant, often debilitating, diarrhoea, steatorrhoea, postprandial abdominal pain and nausea. Awareness of PEI among clinicians is poor outside of high volume HPB centres,14 and symptoms are often overlooked or accepted as unavoidable, treatment-related side-effects. Despite the high incidence, a recent study evaluating 4,554 UK patients with PDAC revealed only one-fifth of patients were prescribed PERT,15 and observed that patients who did receive PERT had a significantly longer survival.
Management of PEI involves pancreatic enzyme replacement therapy (PERT), which should be used to maintain weight and improve the symptoms of maldigestion.16 PERT should begin when PEI is diagnosed or when there is the clinical suspicion for PEI.17
Therapy should start with doses of 40,000-50,000 units of lipase with meals, and 10,000-25,000 units with every snack.18,19 Dose escalation and inhibition of gastric acid secretion may be warranted according to response; in patients who fail to respond to treatment, extra-pancreatic causes should be evaluated.18
Failure to treat PEI with PERT causes detrimental effects on nutritional status20 and quality of life.8 Dietary intake and nutritional status should be monitored regularly to maximize patient compliance and specialist dietetic assessment sought in patients with underlying malnutrition.21 Untreated, PEI may lead to multiple micronutrient deficiencies and weight loss, and the consequential gastrointestinal symptoms may be incorrectly attributed to food intolerances, leading to unnecessary restrictions.6
Cancer cachexia and PDAC
Cancer cachexia is as a multifactorial syndrome characterised by an ongoing loss of skeletal muscle mass (with or without loss of fat mass) that cannot be fully reversed by conventional nutritional support and leads to progressive functional impairment.22
Cancer cachexia is driven by a variable combination of anorexia and reduced oral intake, altered macronutrient metabolism, inflammation and muscle wasting.23 PDAC patients have the highest prevalence of cancer cachexia of all cancer patients, experiencing the most severe weight loss.24
Weight loss and cachexia predict poor outcomes in PDAC.25-27 Most patients with PDAC will die with cachexia, and it is estimated that 30% will die of cachexia.6,28,29
Sarcopenia, commonly described as the age-associated loss of muscle, is accelerated in patients with poor nutritional intake, physical inactivity and cachexia -induced inflammation.30 PDAC typically presents in the seventh decade of life, and the associated anorexia, cancer cachexia- induced inflammation, and physical decline combine to increase the risk and rate of sarcopenia.
Assessment of body composition, a direct recommendation of the international consensus group as part of cancer cachexia assessment, has highlighted high levels of sarcopenic obesity (a condition with co-existing low muscle mass and increased adipose tissue levels) among patient with PDAC. Sarcopenic obesity is a negative prognostic factor for patients with PDAC, regardless of disease stage.28
Treatment of cancer cachexia
While weight and muscle loss caused by cancer cachexia cannot be reversed by the provision of nutritional support,22 patients still benefit from individualised assessment to ensure that modifiable nutrition impact symptoms are addressed, and dietary protein intake and dose distribution optimised.31 The therapeutic potential of exercise as a treatment strategy has been suggested by some authors;32,33 both endurance activity to modulate inflammation, and progressive resistance training to maximise muscle mass and function.
No pharmacological agent has to date shown efficacy in counteracting depletion of muscle strength and in attenuating cancer cachexia symptoms.34 Anamorelin, a ghrelin receptor agonist, has shown the most promise, improving QOL and muscle mass in phase three studies.35 No improvement was seen in muscle strength however, and consequently the drug failed to get regulatory approval.
Evidence suggests that omega-3 poly-unsaturated fatty acids (N-3 PUFA) have anti-tumour effects in pancreatic cancer cell lines and animal models.36,37 N-3 PUFA have been shown to downregulate pro-inflammatory cytokines,38,39 and ameliorate elevated resting energy expenditure in pancreatic cancer patients with cachexia.40 Lack of compliance, differing supplement content and type and heterogenous cancer populations have been highlighted as barriers to the systematic evaluation of the impact of N-3 PUFA in cancer cachexia.41,42
While multiple anti-inflammatory substrates have been proposed as a mechanism to overcome the pro-inflammatory, hyper catabolic effects of cancer cachexia, there is increasing acceptance that a multimodal approach is necessary to counteract the multifactorial aetiology of malnutrition in pancreatic cancer.43,44
 (click to enlarge)
(click to enlarge)