Nutrition in critical care – the latest ESPEN guidelines
While ESPEN’s approach may be more measured, more tailored and less forthright, the goals of ICU nutrition remain the same: to minimise malnutrition while avoiding complications of nutrition provision during and, for some, well after their hospital stay
Ms Lisa Shanahan, Specialist Dietitian in Critical Care, Mater Hospital, Dublin
Working in the ICU is fast-paced and challenging. Providing a quality nutrition service while managing the complex needs of this heterogeneous group of patients requires a dedicated service by a dietitian with highly developed skills, expertise and knowledge in the field of critical care. The need for a dietitian to change and adapt practice is amplified.
Consensus guidelines are an essential resource in the sea of literature produced in critical care nutrition. They help bring clarity to an area of nutrition that is heavily studied, but has a body of evidence with sometimes overwhelming contradictions.
With each research question addressed, more questions arise exponentially. Fundamental principles such as providing enteral nutrition (EN) early, using EN ahead of parenteral nutrition (PN), and using gastric residual volumes (GRVs) to monitor feed tolerance are no longer as clear cut. Often when making decisions on how best to treat a patient, the best way forward is to go back to the consensus guidelines.
New guidelines
The ESPEN guideline1 on clinical nutrition in the ICU1 is an update and extension of previous ESPEN guidelines on enteral nutrition and parenteral nutrition 2006 and 2009 using upgraded guideline methodology. Previous guidelines were based mainly on observational and retrospective data, but the new document incorporates data from large randomised controlled trials (RCTs) since performed. It is accompanied by a position paper ‘Monitoring nutrition in the ICU’2 that summarises theoretical and practical aspects of monitoring medical nutrition therapy (MNT) in critically ill patients.
The aim was to integrate the best most updated knowledge on ICU nutrition using the expertise of professional methodologists, critical care nutrition experts and critical care professionals to help ICUs deliver optimal nutrition and to illuminate gaps in knowledge to guide future research.
For any dietitian involved in the care of critically ill patients, the ESPEN guideline needs a thorough read – and many re-reads – in conjunction with previous critical care nutrition guidelines. I have done a summary of the most relevant guidelines which will soon be available on www.hse.ie under critical care programme documents and resources. You can also email me at: lshanahan@mater.ie for a copy.
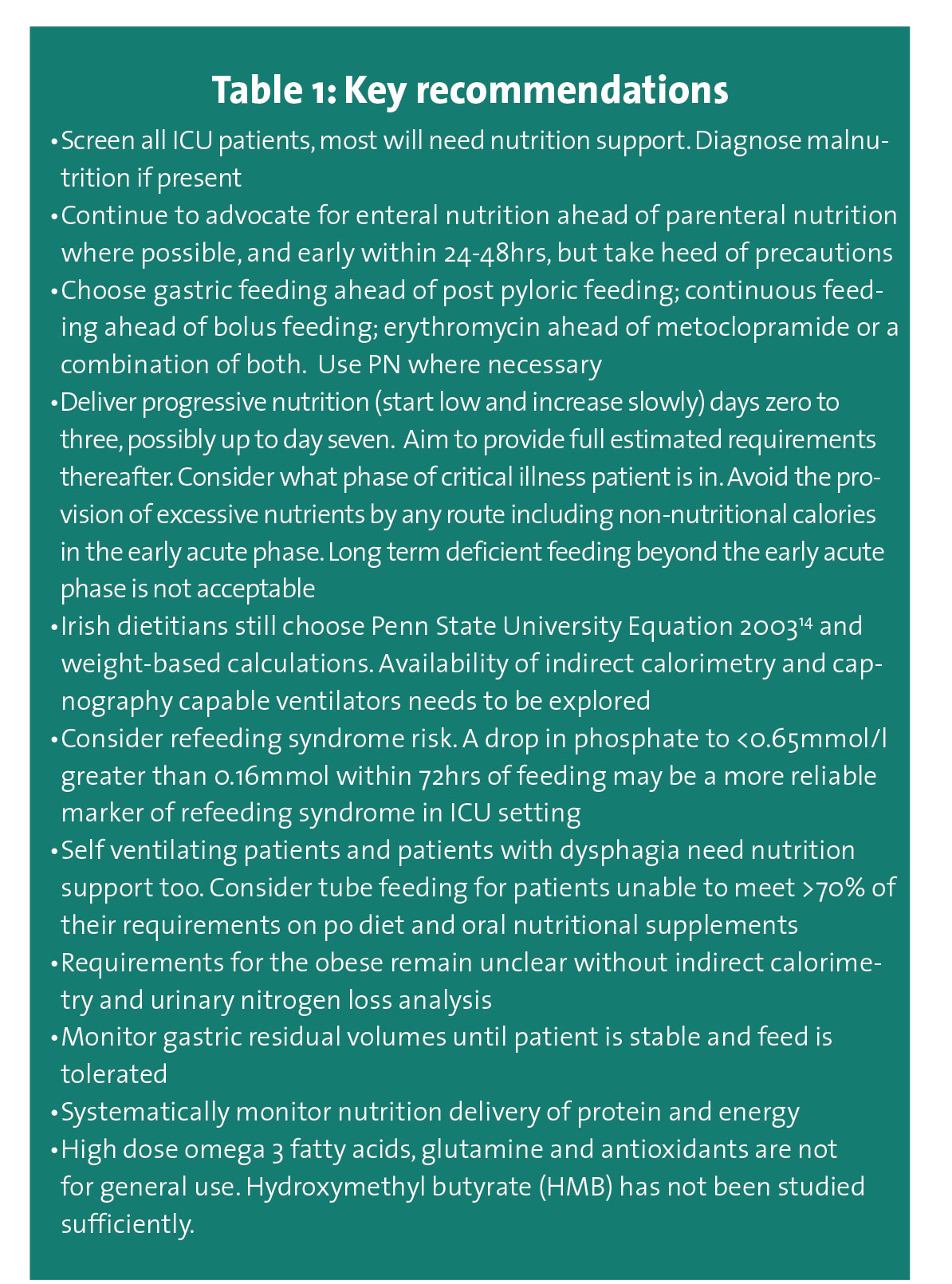
Rather than repeating each recommendation I will discuss the more general recommendations here with a focus on some tools that are useful for integrating the guideline into practice (See Table 1).
(click to enlarge)
ESPEN continues to recognise the need for early enteral nutrition within 24-48hrs in all patients at risk of malnutrition or with malnutrition if po diet is inadequate (<70% of requirements). It does not endorse any specific screening tool or malnutrition diagnosis tool.
For the first time ESPEN ICU guidelines specify precautions to commencing enteral nutrition and endorse the progressive enteral feeding approach recommended by the European Society for Intensive Care Medicine (ESICM) 2017 clinical practice guidelines3 on early enteral nutrition in critically ill patients.
This cautious approach to EN involves commencing feeding at 10-20mls/hr and increasing feed rate with close monitoring of GI symptoms over the subsequent three to seven days. It is in contrast to aggressive feeding practices such as starting feed at target rate or PEP-uP type feeding protocols encouraged in the past five to 10 years. ESPEN recommends hypocaloric feeding to <70% of estimated energy requirements for up to one week after ICU admission. This is new and is based on a number of concepts:
Energy and protein overfeeding may inhibit autophagy. Autophagy is the body’s way of dealing with destroyed cell components by degrading and recycling them for new cell formation. Autophagy is upscaled during stress
Energy and protein overfeeding may cause mitochondrial dysfunction. Mitochondria have many functions including generating ATP or energy for cells
Endogenous glucose production, once thought to be a short lived glycogenolysis post insult is now believed to be as much as 500-1400 kcals per day over the first 48-72hours of critical illness. Endogenous glucose production is not reduced by provision of exogenous nutrition therefore overfeeding ensues
Increased recognition of the incidence and implications of refeeding syndrome in critically ill patients. The Refeeding Syndrome Trial (RCT) by Doig et al4 and high quality retrospective observational data by Olthof et al5 show benefits to caloric restriction in ICU patients with refeeding syndrome (defined by a drop in phosphate to </= 0.65mmol by at least 0.16mmol within the first 72 hours of feeding).
Studies
These concepts could explain why RCTs of trophic and hypocaloric feeding versus standard feeding (INTACT,6 EDEN,7 PermiT8) show no difference in outcomes and why trials of aggressive feeding strategies versus standard care (EAT-ICU,9 NUTRIREA-2,10 EPaNIC,11 TARGET12) also show no benefits to patients, and in some cases raise the question of harm. For those of us who have focused on delivering full energy requirements as early as possible, cautious progressive feeding is a shift in mindset. It does also require further validation.
It is worth noting that studies of hypocaloric feeding have flaws and that prescribed nutrition is often not achieved due to feed interruptions and intolerance. Further, due to ethical issues, malnourished patients are rarely included in feeding trials and research on the impact of nutrition on long-term outcomes other than mortality such as quality of life and functional status is in its infancy.
Also, there are no RCTs addressing the effect of duration of starvation on patient outcome. Prospective evidence to confirm that full target nutrition improves outcomes is frustratingly lacking.
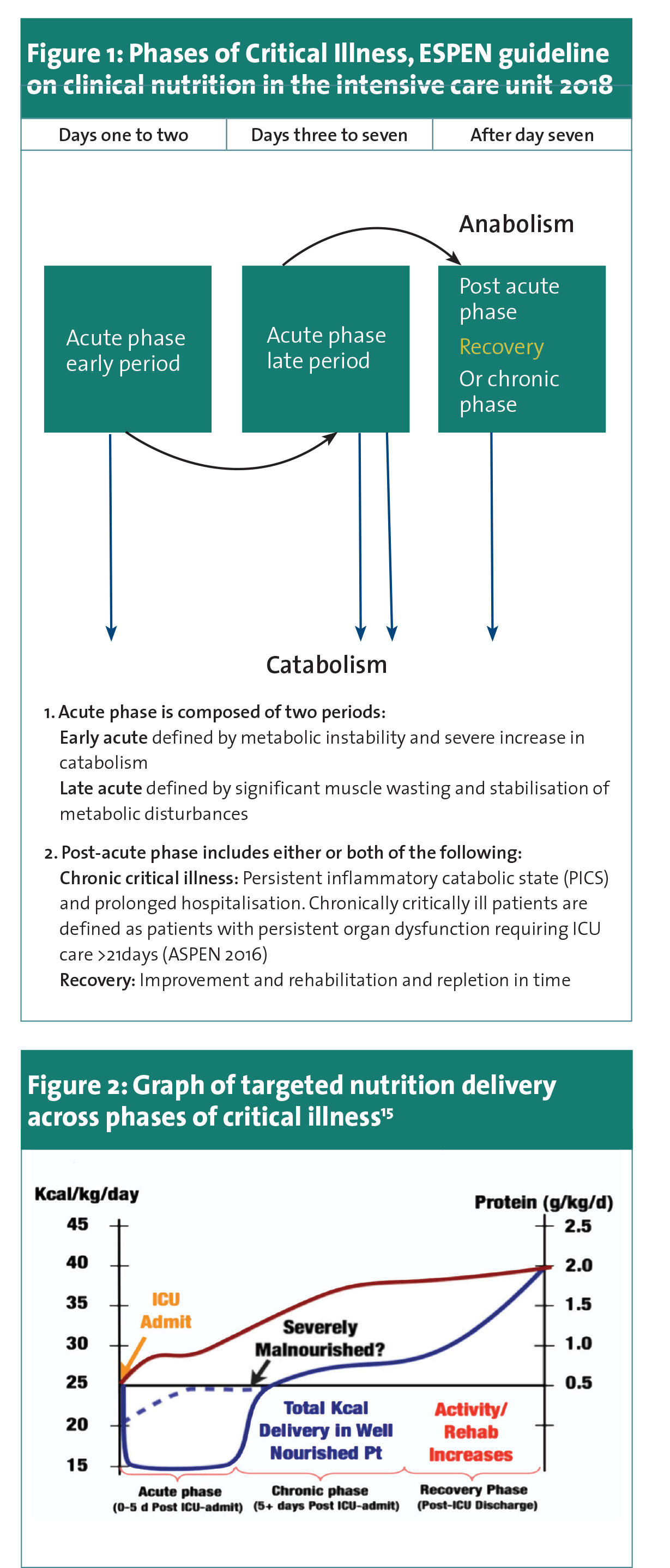
ESPEN highlights that “at a certain time, caloric delivery should likely match expended energy. Optimal timing likely differs between patients and is not settled yet” (after three and before seven days). It is imperative to consider where the patient is in their critical illness journey (ie. how sick are they, how many organ supports are they on, are they requiring vasopressors and if so what dose, are they clinically improving, clinically stable/static or disimproving). This is not easy, varies from patient to patient and requires experience.
See Figure 1, a description of phases of critical illness as a useful guide. See Figure 2 and Table 2 for proposed nutrition delivery according to critical illness phase.
(click to enlarge)
(click to enlarge)
Protein provision
ESPEN sits on the fence when it comes to protein provision, recommending progressive delivery to 1.3g/kg actual weight (or adjusted body weight in obese patients, though how to calculate this is ambiguous). This is the midpoint of ASPEN 201613 recommendation for 1.2-1.5g/kg. They do not specify requirements in continuous renal replacement therapy or other protein-losing conditions, except for advising us to consider 1.5-2g/kg in trauma patients. Why? Observational data may tempt us to give higher protein, but there is little RCT research to support these targets. Presier14 describes upcoming trials on protein which will hopefully shed some light on this topic.
In conclusion, while ESPEN’s approach may be more measured, more tailored and less forthright, the goals of ICU nutrition remain the same: to minimise malnutrition while avoiding complications of nutrition provision during and, for some, well after their hospital stay.
References
Singer P, et al., ESPEN guideline on clinical nutrition in the intensive care unit, Clinical Nutrition (2018), https:// doi.org/10.1016/j.clnu.2018.08.037
Berger MM, et al., Monitoring nutrition in the ICU, Clinical Nutrition (2018), https://doi.org/10.1016/j.clnu.2018.07.009
Blaser AR, et al., Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines, Intensive Care Med (2017) 43:380–398, doi.org/ 10.1007/s00134-016-4665-0
Doig G, et al., Restricted versus continued standard caloric intake during the management of refeeding syndrome in critically ill adults: a randomised, parallel-group, multicentre, single-blind controlled trial, Lancet (2015) 3:943-952, doi.org/10.1016/S2213-2600(15)00418-X
Olthof LE, et al., Impact of caloric intake in critically ill patients with, and without, refeeding syndrome: a retrospective study, Clinical Nutrition (2017), doi.org/10.1016/j.clnu.2017.08.001
Braunschweig CA, et al., Intensive Nutrition in Acute Lung Injury: A Clinical Trial (INTACT), JPEN J Parenter Enteral Nutr (2014), doi.org/: 10.1177/0148607114528541
Rice T, et al., Initial Trophic vs Full Enteral Feeding in Patients With Acute Lung Injury The EDEN Randomized Trial, JAMA (2012), doi.org/10.1001/jama.2012.137
Arabi YM, et al., Permissive Underfeeding or Standard Enteral Feeding in Critically Ill Adults, N Engl J Med (2015) 372:2398-408. doi/org 10.1056/NEJMoa1502826
Allingstrup M, et al., Early goal-directed nutrition versus standard of care in adult intensive care patients: the single-centre, randomised, outcome assessor-blinded EAT-ICU trial, Intensive Care Med (2017) 43:1637-1647. doi.org/ 10.1007/s00134-017-4880-3
Reignier J, et al., Enteral versus parenteral early nutrition in ventilated adults with shock: a randomised, controlled, multicentre, open-label, parallel-group study (NUTRIREA-2), Lancet (2017). doi.org/10.1016/S0140-6736(17)32146-3
Casaer MP, et al., Early versus Late Parenteral Nutrition in Critically Ill Adults. N Engl J Med (2011). doi.org/ 10.1056/nejmoa1102662
Chapman M, Peake S, et al., Energy-Dense versus Routine Enteral Nutrition in the Critically Ill, N Engl J Med (2018). doi.org/ 10.1056/NEJMoa1811687
McClave SA, Taylor BE, Martindale RG et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N), JPEN J Parenter Enteral Nutr 2016 Feb; 40(2):159-211. doi: 10.1177/0148607115621863
Presier JC. High protein intake during the early phase of critical illness: yes or no? Crit Care 2019; 22:261 doi.org/10.1186/s13054-018-2196-5
Wischmeyer PE, et al., Tailoring nutrition therapy to illness and recovery, Critical Care (2017), doi.org/ 10.1186/s13054-017-1906-8
 (click to enlarge)
(click to enlarge)