An overview of the assessment and management of this nutritionally challenging condition
Prof Kevin Conlon, Professor of Surgery, Trinity College Dublin; Consultant Surgeon, St Vincent’s University Hospital, Dublin and Ms Sinead Duggan, Non-Clinical Assistant Professor of Surgery, Professorial Surgical Unit, Tallaght Hospital
Chronic pancreatitis (CP) is a progressive inflammatory disease which results in the gradual destruction of pancreatic tissue and progressive exocrine and endocrine dysfunction. The nutritional management of patients with CP tends to be problematic. Issues of concern include vitamin deficiency, osteoporosis, brittle diabetes mellitus (DM) and malabsorption – all of which increase morbidity and affect quality of life (QoL).
Pancreatic exocrine insufficiency
Assessing pancreatic exocrine function
A progressive loss of the exocrine acinar cells in CP results in the reduced production and secretion of pancreatic enzymes, thereby causing nutrient maldigestion and malabsorption (known as pancreatic exocrine insufficiency [PEI]).
Malabsorption of all macronutrients occurs, however fat malabsorption tends to be the most clinically evident. Gross fat malabsorption which results in overt steatorrhoea may only occur in the advanced stages of the disease process.
However, patients may report other symptoms of malabsorption which are less obvious, including bloating, wind, failure to maintain weight, nausea and abdominal pain.
Bloating may be due to the passage of undigested carbohydrate into the colon, where fermentation by the colonic flora results in flatulence and abdominal discomfort.1
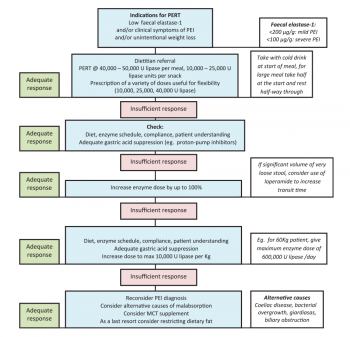
Currently, the gold-standard test for measuring pancreatic exocrine function is the faecal elastase-1 (FE-1) test. FE-1 is a human-specific pancreatic enzyme that is not degraded during intestinal transit, is enriched five to sixfold in the faeces, and is therefore a reliable test of exocrine function.2
Pancreatic enzyme replacement therapy (PERT) does not need to be interrupted for testing pancreatic function, nor does the patient have to ingest a specific fat intake for testing, and therefore the FE-1 test is practical in the clinical setting.
A FE-1 level of <100µg/g indicates severe PEI, and 100-200µg/g indicates moderate PEI. Levels should be evaluated in the context of a full clinical assessment.
Pancreatic enzyme replacement therapy
PERT is the mainstay of treatment for PEI3 and treats overt steatorrhoea as well as the less obvious malabsorptive symptoms (bloating, wind, failure to maintain weight, nausea and abdominal pain). It is also a cost-effective4 and safe5,6 therapy.
Several recent randomised controlled trials have demonstrated an increase in fat and nitrogen absorption, improvements in stool frequency, reduced abdominal pain and reduced flatulence for those taking PERT (up to 80,000 units [U] lipase with main meals) compared to a placebo.5,6
Patients with PEI tend to be undertreated, and PERT tends to be under-prescribed.7 It is usually advisable to start with a dose of 40,000-50,000U lipase per meal and 10,000-25,000U lipase per snack,8,9 and to titrate gradually upwards depending on the patient’s response8,9,10 to a maximum dose11 of 10,000U lipase/kg body weight per day.
Acid-suppression medication may also be required8 as pancreatic enzymes are destroyed at a low pH. Regular and detailed dietary assessment is vital to ensure appropriate and adequate PERT usage and to ensure compliance. Intervention by a pancreatic dietitian is considered essential.11,12Figure 1 details the management of PEI in CP.1
(click to enlarge)
Type 3 diabetes mellitus
DM is a complication of CP in up to 50% of cases.13 The form of DM that develops in CP is termed type 3 DM and, although this form is distinctly different from types 1 and 2, it is often misclassified, usually as type 2 DM.14 Typically, those with type 3 DM are older than those with type 1, but not type 2 diabetes. They have lower BMI than in type 2 DM.15 Many patients with type 3 DM have difficulty with erratic glucose control.
Hypoglycaemia is a particular concern due to enhanced peripheral insulin sensitivity and a decrease in glucagon production.15 The risk of hypoglycaemia is similar to that of type 1 DM, exacerbated in pancreatogenic DM by (frequently) poor dietary intake, malabsorption and, for some, persistent alcoholism.14 There has been little guidance for the management of patients with type 3 DM to date, particularly around diet and lifestyle. Nevertheless, the prevention of episodes of hypoglycaemia is a priority, as well as a reduction in erratic swings in blood glucose control.1
Vitamin D and bone health
Patients with CP may have low serum 25-OHD (vitamin D) levels compared to controls,16 resulting in a reduction in the absorption of dietary calcium and thereby negatively affecting bone mineral density. Furthermore, smoking, poor physical activity, suboptimal diet and malabsorption all contribute to bone demineralisation. Studies have reported a high prevalence of osteoporosis and osteopenia in CP, ranging from 39-74%.17,18,19 The American Gastroenterological Association recommended that patients with specific gastrointestinal (GI) conditions (inflammatory bowel disease, coeliac disease and post-gastrectomy) should have routine dual-energy x-ray absorptiometry (DXA) if they have at least one additional osteoporosis risk factor.20 Therefore, as the risk of osteoporosis and fracture21 is as high in CP as in other comparable GI conditions, the same recommendations could apply. At the very least, a DXA scan should be ordered for those who have had a previous low-trauma fracture, are post-menopausal, > 50 years of age for men, and/or have intractable malabsorption.22
Basic preventative measures should also be applied, including ensuring adequate dietary calcium and vitamin D, the use of supplementation, where appropriate, and follow-up to ensure that serum vitamin D levels are optimally repleted.1
Fat-soluble vitamin deficiency
Published guidelines on the nutritional management of CP have advised that fat-soluble vitamin deficiency is common in CP.23,24 However, the studies to support this view were largely published in the 1980s and 1990s,25,26 and a more recently published Dutch study found a lower prevalence of deficiency for vitamin A (3%) and vitamin E (10%).27 Consequently, biochemical assessment of serum fat-soluble vitamin levels is advised and “blind” routine supplementation should be avoided.
There is little guidance on dosage for fat-soluble vitamin replacement for those who have detectable clinical or subclinical deficiencies, again due to a gap in the research. Particular caution is advised in the administration of mega-doses of fat-soluble vitamins.1
Diet and nutrition support
Resting energy expenditure is raised in those with CP (by up to 50%), especially in underweight patients and in those with sepsis28,29 and, therefore, a high calorie intake (35kcal/kg/day) is usually warranted.24 Extreme low-fat or fat-free diets are not recommended for patients with CP (although frequently advised) and, in fact, 30% of calories may be given as fat. This should be facilitated by adequate administration of PERT to counteract any fat malabsorption.23 There is no evidence that vegetable fat is better tolerated than animal fat.20,23 Protein intake of 1-1.5g/kg/day should be provided.24 In general, a high-carbohydrate diet is recommended, although this may need modification in the patient with DM.1,23 A high-fibre diet may reduce the efficacy of pancreatic enzymes and therefore patients should avoid very high-fibre diets if PERT control is not optimal.23,30 Small, frequent meals should be taken, and oral nutritional supplements (ONS) may be required for some patients.24 About 5% of patients will require tube feeding,24 specifically those who are unable to take sufficient calories, who are losing weight despite apparently adequate diet, during acute complications, and for some patients pre-surgery.
Total parenteral nutrition (TPN) will be necessary in a minority of situations (< 1% of cases),24 usually in complicated cases such as gastric outlet obstruction (without jejunal access), complex pancreatic fistulae, and in the severely malnourished patient pre-surgery (where enteral feeding is not possible).
Antioxidant therapy
Constant, debilitating pain is a major problem for patients with CP which greatly reduces QoL, and for which there is no effective medical treatment. The theory that free radical-induced pancreatic damage resulting in intractable pancreatic pain may be alleviated by taking an antioxidant preparation showed initial promise; improvements were demonstrated in QoL, pain and working days lost.31 However, a more recent trial showed that, despite an increase in blood antioxidant levels, QoL and pain did not improve in the antioxidant-treated arm compared to the placebo group.32 More research is required before definitive clinical recommendations can be made.
(click to enlarge)
Conclusion
Given the risk factors for malnutrition in patients with CP, a structured nutritional evaluation is crucial. Figure 21,23 provides an evidence-based framework for use in the assessment and management of this nutritionally challenging condition.
References
Duggan SN, Conlon, KC. A practical guide to the nutritional management of chronic pancreatitis. Practical Gastroenterology 2013; 118 (Nutrition Series): 24-32
Lankisch PG, Schmidt I, Konig H et al. Faecal elastase 1: not helpful in diagnosing chronic pancreatitis associated with mild to moderate exocrine pancreatic insufficiency. Gut 1998; 42(4): 551-554
Toouli J, Biankin AV, Oliver MR et al. Management of pancreatic exocrine insufficiency: Australasian Pancreatic Club recommendations. Med J Aust 2010; 193(8): 461-467
Morawski JH, Prufert A, van Engen A et al. Cost-effectiveness analysis of pancreatin minimicrospheres in patients with pancreatic exocrine insufficiency due to chronic pancreatitis. J Med Econ 2012; 15(1): 15-25
Whitcomb DC, Lehman GA, Vasileva G et al. Pancrelipase delayed-release capsules (CREON) for exocrine pancreatic insufficiency due to chronic pancreatitis or pancreatic surgery: A double-blind randomized trial. Am J Gastroenterol 2010; 105(10): 2276-2286
Thorat V, Reddy N, Bhatia S et al. Randomised clinical trial: the efficacy and safety of pancreatin enteric-coated minimicrospheres (Creon 40000 MMS) in patients with pancreatic exocrine insufficiency due to chronic pancreatitis – a double-blind, placebo-controlled study. Aliment Pharmacol Ther 2012; 36(5): 426-436
Sikkens EC, Cahen DL, van Eijck C et al. The daily practice of pancreatic enzyme replacement therapy after pancreatic surgery: a northern European survey: enzyme replacement after surgery. J Gastrointest Surg 2012; 16(8): 1487-1492
Imrie CW, Connett G, Hall RI et al. Review article: enzyme supplementation in cystic fibrosis, chronic pancreatitis, pancreatic and periampullary cancer. Aliment Pharmacol Ther 2010; 32(1): 1-25
Dominguez-Munoz JE. Pancreatic enzyme replacement therapy for pancreatic exocrine insufficiency: when is it indicated, what is the goal and how to do it? Adv Med Sci 2011; 56(1): 1-5
Layer P, Keller J. Lipase supplementation therapy: standards, alternatives, and perspectives. Pancreas 2003; 26(1): 1-7
Sikkens EC, Cahen DL, Kuipers EJ et al. Pancreatic enzyme replacement therapy in chronic pancreatitis. Best Pract Res Clin Gastroenterol 2010; 24(3): 337-347
Sikkens EC, Cahen DL, van Eijck C et al. Patients with exocrine insufficiency due to chronic pancreatitis are undertreated: a Dutch national survey. Pancreatology 2012; 12(1): 71-73
Lankisch PG, Lohr-Happe A, Otto J, et al. Natural course in chronic pancreatitis. Pain, exocrine and endocrine pancreatic insufficiency and prognosis of the disease. Digestion 1993; 54(3): 148-155
Ewald N, Kaufmann C, Raspe A et al. Prevalence of diabetes mellitus secondary to pancreatic diseases (type 3c). Diabetes Metab Res Rev 2012; 28(4): 338-342
Cui Y, Andersen DK. Pancreatogenic diabetes: special considerations for management. Pancreatology 2011; 11(3): 279-294
Teichmann J, Mann ST, Stracke H et al. Alterations of vitamin D3 metabolism in young women with various grades of chronic pancreatitis. Eur J Med Res 2007; 12(8): 347-350
Dujsikova H, Dite P, Tomandl J et al. Occurrence of metabolic osteopathy in patients with chronic pancreatitis. Pancreatology 2008; 8(6): 583-586
Duggan SN, O’Sullivan M, Hamilton S et al. Patients with chronic pancreatitis are at increased risk for osteoporosis. Pancreas 2012; 41(7): 1119-1124
Duggan SN, Smyth ND, Murphy A et al. High prevalence of osteoporosis in patients with chronic pancreatitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2013
American Gastroenterological Association medical position statement: guidelines on osteoporosis in gastrointestinal diseases. Gastroenterology 2003; 124(3): 791-794
Tignor AS, Wu BU, Whitlock TL et al. High prevalence of low-trauma fracture in chronic pancreatitis. Am J Gastroenterol 2010; 105(12): 2680-2686
Duggan SN, Conlon KC. Bone health guidelines for patients with chronic pancreatitis. Gastroenterology 2013
Duggan S, O’Sullivan M, Feehan S et al. Nutrition treatment of deficiency and malnutrition in chronic pancreatitis: a review. Nutr Clin Pract 2010; 25(4): 362-370
Meier R, Ockenga J, Pertkiewicz M et al. ESPEN Guidelines on Enteral Nutrition: Pancreas. Clin Nutr 2006; 25(2): 275-284
Nakamura T, Takebe K, Imamura K et al. Fat-soluble vitamins in patients with chronic pancreatitis (pancreatic insufficiency). Acta Gastroenterol Belg 1996; 59(1): 10-14
Kalvaria I, Labadarios D, Shephard GS et al. Biochemical vitamin E deficiency in chronic pancreatitis. Int J Pancreatol 1986; 1(2): 119-128
Sikkens ECC DL, Arjun DK, Braa H et al. The prevalence of fat-soluble vitamin deficiencies and a decreased bone mass in patients with chronic pancreatitis. Pancreatology 2013
Dickerson RN, Vehe KL, Mullen JL et al. Resting energy expenditure in patients with pancreatitis. Crit Care Med 1991; 19(4): 484-490
Hebuterne X, Hastier P, Peroux JL et al. Resting energy expenditure in patients with alcoholic chronic pancreatitis. Dig Dis Sci 1996; 41(3): 533-539
Giger U, Stanga Z, DeLegge MH. Management of chronic pancreatitis. Nutr Clin Pract 2004; 19(1): 37-49
Bhardwaj P, Garg PK, Maulik SK et al. A randomized controlled trial of antioxidant supplementation for pain relief in patients with chronic pancreatitis. Gastroenterology 2009; 136(1): 149-159 e142
Siriwardena AK, Mason JM, Sheen AJ et al. Antioxidant therapy does not reduce pain in patients with chronic pancreatitis: the ANTICIPATE study. Gastroenterology 2012; 143(3): 655-663 e651
 (click to enlarge)
(click to enlarge)
