The paleolithic diet has been studied in very few human cohorts and there is simply not enough good quality studies to suggest the diet would be advantageous
The paleo diet, also known as the paleolithic diet, hunter-gatherer diet, stone age diet and caveman diet, is fast becoming the most popular dietary trend. The aim of the paleo diet is to support healthy eating by adopting the eating habits of the people from the Paleolithic period (from 2.5million to 10,000 years ago) before the industrial and agricultural revolutions.
The diet limits foods such as dairy, grains and legumes that became common when farming emerged. This is based on the premise that farming introduced additional staples into the human diet which outpaced the body’s ability to adapt and that by eating like our ancestors we may reverse the climbing rates of diseases suffered by modern humans such as obesity, diabetes and cardiovascular disease.
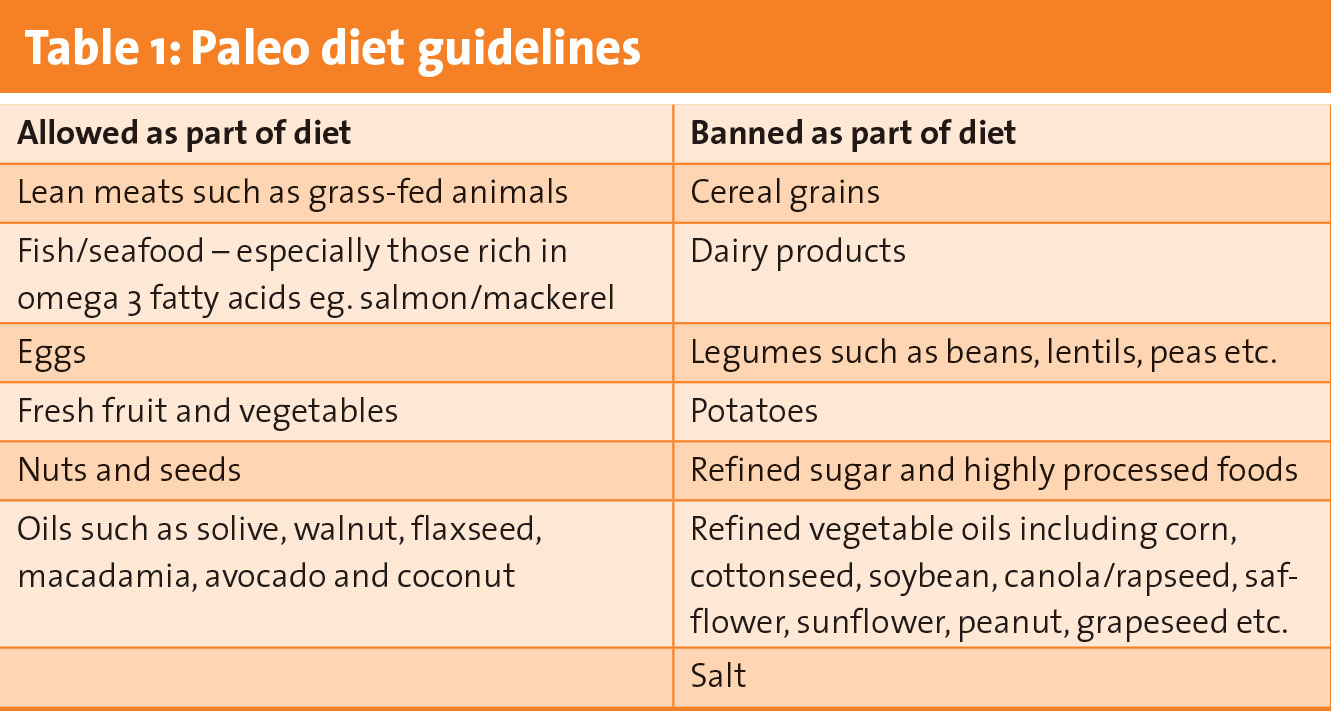
Commercial paleo diets vary and certain plans have stricter recommendations than others, however paleo diets generally follow the guidelines outlined in Table 1.
(click to enlarge)
(click to enlarge)
(click to enlarge)
Why is paleo trending?
Data from different forums show that the most popular reasons for joining the paleo movement is for personal fitness and athleticism, for weight loss, or to reduce the risk of diseases such as heart disease, type 2 diabetes and chronic degenerative diseases.
Aversion to modernity has been glamorised by paleo culture – the desire to strip life down to the caveman. The romanticisation for reconnecting ourselves with our ancestors has also allowed the diet to gain popularity.
What does the evidence say?
There have been three randomised controlled trials conducted on the paleo diet.1,2,3 In these studies all participants were either obese or had type 2 diabetes or glucose intolerance. Control groups were instructed to follow either a diabetic diet,2 a Mediterranean diet1 or a low-fat/high-fibre diet.3 The only consistently observed purported benefits of the paleo diet were lower triglyceride levels.2,3
Weight loss and health advantages
Although the paleo diet showed greater weight loss (p = 0.01) and reduction in waist circumference (p = 0.03) compared to the diabetic diet or Mediterranean diet,1,2 these interventions were carried out over a three to six-month period and had a maximum of 29 participants.
A two-year study with 70 participants showed greater weight loss and reduction in waist circumference on the paleo diet compared to the low-fat/high-fibre diet in the short term (three to six months), however the differential was not maintained at two years.3
Inconsistent results were seen for the paleo diet regarding superior glucose tolerance, HDL cholesterol or diastolic blood pressure and superior LDL cholesterol, CRP levels and systolic blood pressure was not observed by participants on the paleo diet.1,2,3
Also, in contrast to the only consistently observed benefit (lower triglycerides) of the paleo diet found in randomised controlled trials, there is evidence that a weight-controlled diet (which includes dairy foods and whole grains) high in protein, moderate in carbohydrate and low in fat (34% energy from protein, 20% from fat [<10% from saturated fat], 46% from carbohydrate) shows a significant reduction in serum triglycerides and can produce weight loss among obese subjects.4
Legumes
The paleo diet excludes legumes as it dictates that raw and undercooked beans are ‘toxic’ and high in anti-nutrients, however it is important to note the following:
• Lectins and protease inhibitors are greatly reduced with cooking therefore the typical standard way in which we modern humans consume legumes essentially eliminates the anti-nutrient effects
• Research has shown that the benefits of legumes far outweigh their anti-nutrient content and people who eat beans have a higher intake of folate, fibre, potassium, iron, magnesium, phosphorus and zinc than those who rarely consume beans5
• Additionally, studies have revealed that legumes were an important part of our Paleolithic ancestor’s diet and legumes have been found at Paleolithic sites all over the world.6,7
Dairy
Dairy is eliminated as the paleo diet claims that we never evolved to digest dairy. However, it must be noted that:
• We are evolving a mutation as a species whereby we continue to produce the lactase enzyme which breaks down lactose and more of us can digest lactose than ever before
• It is true that not everyone can digest lactose well, however studies have shown that people who do not digest lactose well are capable of tolerating an average of 12g of lactose (lactose in one cup/250ml of milk) at a time with few/no symptoms.8
Grains
Grains are eliminated as the paleo diet claims that our Paleolithic ancestors did not consume grains and consumption leads to inflammation and related health problems, however:
• Evidence shows that ancient humans may have consumed grains and cereal grassews almost 30,000 years ago7,9,10 with granules of grains revealed on stone stools
• Observational studies have shown that whole grains may decrease inflammation, whereas refined grains may increase inflammation.11 Therefore the issue is with the processing, not the grain itself.
Oils and fats
The paleo diet makes recommendations for oils and fats based on three factors:
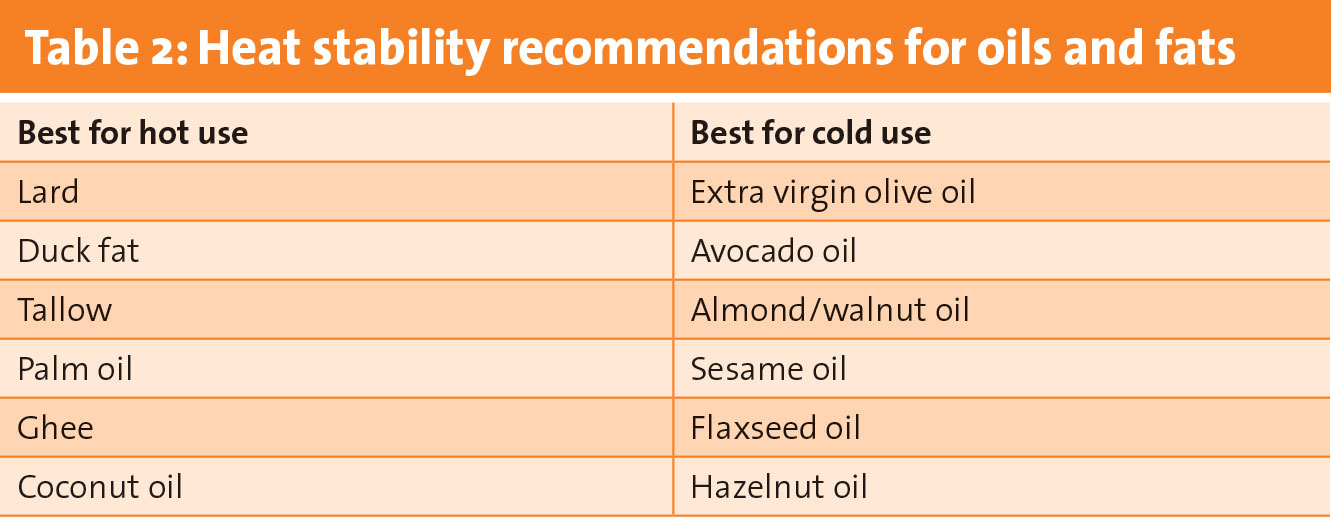
• Heat stability: Saturated fats are embraced because they are typically more heat stable and less prone to oxidation than monounsaturated or polyunsaturated fats. This makes them more suitable for frying and other high temperature cooking. Nut oils and olive oil are recommended to be used unheated to retain antioxidants, vitamins and flavour (see Table 2)
• Omega 6 to omega 3 fatty acid ratio: Paleo recommends using only vegetable oils which have an omega 6 to omega 3 ratio of less than three, eg. flaxseed oil. A high omega 6 to omega 3 ratio limits the amount of omega 3 which we can absorb and is believed to promote the pathogenesis of many diseases, including cardiovascular disease, cancer, and inflammatory and autoimmune diseases.12 Canola oil and mustard seed oil also have a low ratio, however they contain erucic acid so the diet does not recommend these oils
• Erucic acid content: Vegetable oils containing high concentrations of erucic acid (20-50%) such as rapeseed oil and mustard seed oil are not recommended on the paleo diet. The refined oil from the rape plant – canola oil – has a low erucic acid content, but paleo references rat studies that show even low concentrations of canola oil could still elicit cardiac tissue scarring.
Take-home message
The paleolithic diet has been studied in very few human cohorts and not over a long-term period. Therefore there are simply not enough good quality studies to suggest that the paleo diet would be advantageous.
How does this affect dietetic practice?
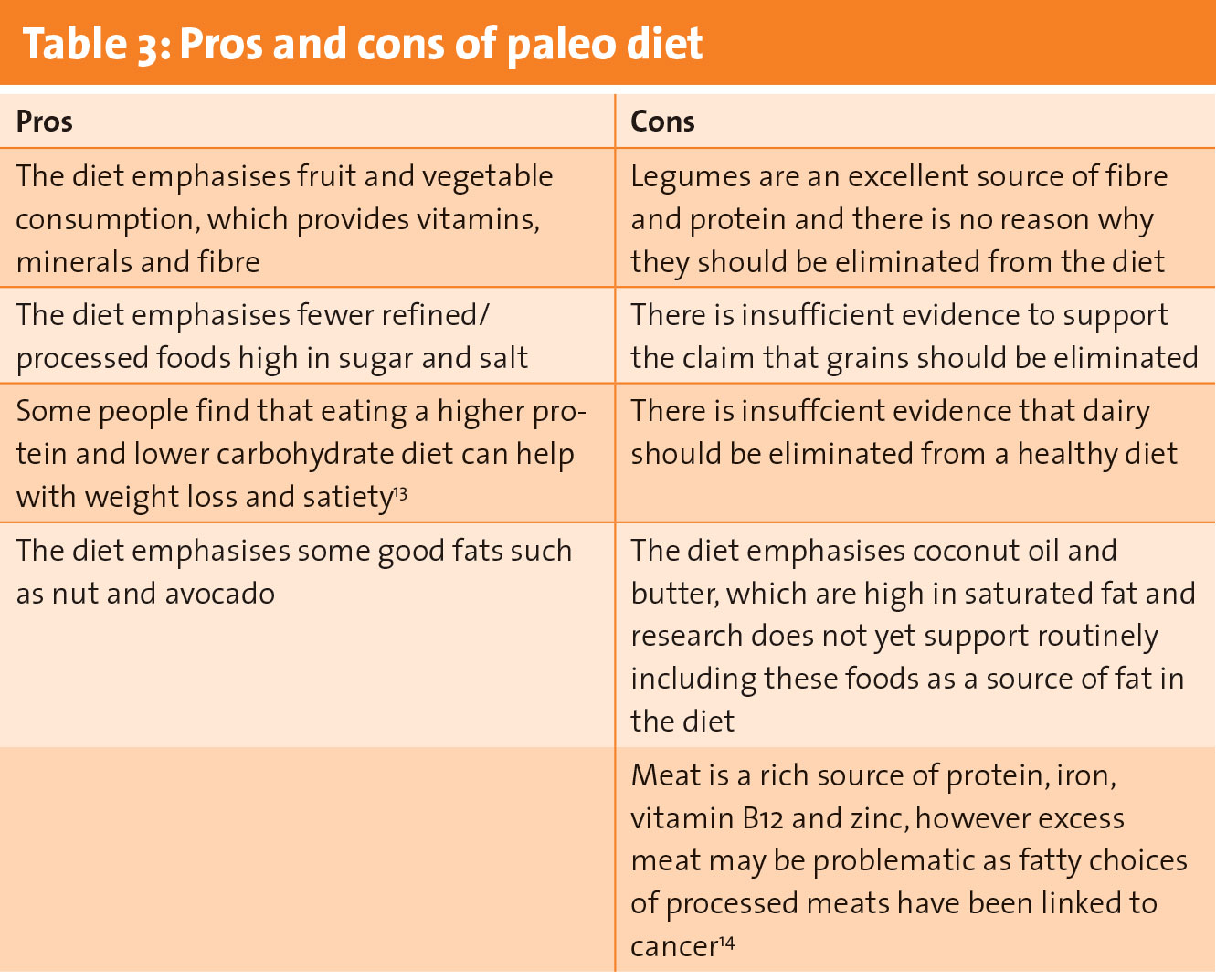
It is important to focus more on the positive aspects for successful dietary intervention and not solely on the negatives of emerging diets. For example, if we look at the positives of the paleo diet and highlight the decrease in processed and refined foods and increase in fruit, vegetable and fish consumption, this is a huge step in a positive direction for clients working towards optimal health.
Acknowledging this would also show clients that as dietitians, we have actively listened to their point of view and are approaching the diet objectively and fairly. Not only that, it puts dietitans in a good position to then explain the evidence-based benefits of including whole grains, dairy products and legumes, which are not traditionally part of paleo.
There is no doubt that many new diets will continue to trend, and we cannot prevent fad diets from becoming popular. However, dietitians must consider if we would be better served by favouring this objective, ‘pros and cons’ approach to critically appraising these new diets. It’s interesting, it keeps our research skills sharp, and allows us to have a perfectly formed answer ready the next time our friend asks us whether or not they should follow the diet everyone is talking about.
This article was previously published in Nutricia’s Best Practice newsletter
References
Lindeberg S, Jönsson T, Granfeldt Y, Borgstrand E, Soffman J, Sjöström K, et al. A Palaeolithic diet improves glucose tolerance more than a Mediterranean-like diet in individuals with ischaemic heart disease. Diabetologia 2007; 50(9): 1795-807
Jönsson T, Granfeldt Y, Ahrén B, Branell UC, Pålsson G, Hansson A, et al. Beneficial effects of a Paleolithic diet on cardiovascular risk factors in type 2 diabetes: a randomized cross-over pilot study. Cardiovasc Diabetol 2009; 8: 35
Mellberg C, Sandberg S, Ryberg M, Eriksson M, Brage S, Larsson C, et al. Long-term effects of a Palaeolithic-type diet in obese postmenopausal women: a 2-year randomized trial. Eur J Clin Nutr 2014; 68(3): 350-7
Noakes M, Keogh JB, Foster PR, Clifton PM. Effect of an energy-restricted, high-protein, low-fat diet relative to a conventional high-carbohydrate, low-fat diet on weight loss, body composition, nutritional status, and markers of cardiovascular health in obese women. Am J Clin Nutr 2005; 81(6): 1298-306
Mudryj AN, Yu N, Hartman TJ, Mitchell DC, Lawrence FR, Aukema HM. Pulse consumption in Canadian adults influences nutrient intakes. Br J Nutr 2012; 108(Suppl 1): S27-36
Lister PR, Holford P, Haigh T, Morrison DA. Acacia in Australia: Ethnobotany and potential food crop. In: Janick J (ed.), Progress in new crops. ASHS Press, Alexandria, VA. 1996, pp 228-236
Henry AG, Brooks AS, Piperno DR. Microfossils in calculus demonstrate consumption of plants and cooked foods in Neanderthal diets (Shanidar III, Iraq; Spy I and II, Belgium). Proc Natl Acad Sci USA 2011; 108(2): 486-91
Almeida CC, et al. Beneficial effects of long-term consumption of a probiotic combination of Lactobacillus casei Shirota and Bifidobacterium breve Yakult may persist after suspension of therapy in lactose-intolerant patients. Nutr Clin Pract 2012; 27(2): 247-51
Hardy K, Buckley S, Collins MJ, Estalrrich A, Brothwell D, Copeland L, et al. Neanderthal medics? Evidence for food, cooking, and medicinal plants entrapped in dental calculus. Naturwissenschaften 2012; 99(8): 617-26
Revedin A, Aranguren B, Becattini R, Longo L, Marconi E, Lippi MM, et al. Thirty thousand-year-old evidence of plant food processing. Proc Natl Acad Sci USA 2010; 107(44): 18815-9
Anderson A, et al. Whole-grain foods do not affect insulin sensitivity or markers of lipid peroxidation and inflammation in healthy, moderately overweight subjects. J Nutr 2007; 137(6): 1401-1407
Simopoulos AP. The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed Pharmacother 2002; 56(8): 365-79
Brehm BJ & D’Alessio DA. Benefits of high-protein weight loss diets: enough evidence for practice? Curr Opin Endocrinol Diabetes Obes 2008: 15(5): 416-21
Bouvard V, Loomis D, Guyton KZ, et al. Carcinogenicity of consumption of red and processed meat. Lancet Oncol 2015; 16(16): 1599-600
 (click to enlarge)
(click to enlarge)