Closure of patent foramen ovale using percutaneous devices is outlined by the team at Galway University Hospitals
Prof Kieran Daly, Consultant Cardiologist, University Hospital Galway, Galway, Dr Rory Durkan, SHO in Cardiology, Galway University Hospitals, Galway, Dr Roisin Colleran, SpR in Cardiology, Galway University Hospitals, Galway and Dr Briain MacNeill, Consultant Cardiologist, Galway University Hospitals, Galway
A patent foramen ovale (PFO) is a small connection that exists between the left atrium (LA) and right atrium (RA) and results in a haemodynamically insignificant degree of blood shunting through the inter-atrial septum.
It is a normal component of foetal circulation but closes in the majority of individuals shortly after birth. However, PFO persists into adulthood in approximately 25-30% of individuals.1
Introduction
Several studies have indicated an association between a PFO and cryptogenic stroke.2-4 Strokes are classified as cryptogenic when no aetiological agent can be readily identified as the underlying cause. Cryptogenic strokes account for as many as 40% of ischaemic strokes.5
Interestingly, the prevalence of a PFO in cryptogenic stroke patients is three times more common than in patients with stroke of known cause.6 An even stronger association exists between the prevalence of a PFO and concomitant atrial septal aneurysm (ASA) in patients with cryptogenic stroke compared with stroke patients of known cause.6
Furthermore, patients with concomitant ischaemic stroke and PFO are younger (< 55 years) and lack the traditional cardiovascular risk factors for stroke.3 The mechanism responsible for the increased prevalence of ischaemic stroke in patients with PFOs is a paradoxical embolus originating in the venous circulation and traversing into the left systemic circulation via the conduit provided by a PFO. Currently, therapeutic approaches for the prevention of recurrent ischaemic stroke can be divided into medical therapy with antithrombotic agents (warfarin or aspirin), open surgical repair or closure of the PFO with percutaneous devices. Percutaneous PFO closure is an attractive option as it avoids the morbidity associated with long-term anticoagulation.
Diagnosis of a patent foramen ovale
The gold standard investigation for the identification of a PFO is a transoesophageal echocardiogram with a bubble study after a sustained Valsalva manoeuvre. The immediate effect following the Valsalva manoeuvre is to augment venous return to the RA and cause increased right atrial pressure to open the PFO. During this phase, miniature bubbles, created by aerating a saline solution, are injected into the peripheral venous circulation and are carried into the RA. The presence of a PFO is signalled by the identification of the bubbles passing throughout the RA directly into the LA.
Figure 1. Tunnel PFO visible between RA and LA (red arrow)(click to enlarge)
Percutaneous closure devices
The first reported use of a percutaneous closure device for closure of a PFO was in 1992.7 In Europe, at least 12 different PFO closure devices have received the CE marking. The currently approved devices fall into one of four categories: double umbrella designs, suture-based closure, energy-based closure and in-tunnel devices.
Historically, the most commonly utilised devices are the Amplatzer (AGA Medical Corporation, US) and the STARFlex (NMT Medical, US). Devices are inserted by a minimally invasive procedure with a low morbidity. Peri-procedural complications have fallen below 1% in some experienced centres.8 The major reported complications include atrial arrhythmias, early and late thrombosis, device embolisation, endocarditis, vascular injury and cardiac tamponade. However, PFO devices are not all similar and significant differences exist between the Amplatzer and STARFlex occluder with regard to incidence of atrial arrhythmias, peri-procedural complications, PFO closure rates and device thrombus. In one particular study, there was a significantly increased incidence of atrial fibrillation in patients who had the STARFlex implanted compared with Amplatzer device: 10% versus 2.9%, respectively.9 PFO closure rates are better with the Amplatzer occluder compared with the STARFlex occluder; effective closure rate at six months for the Amplatzer device was 93.5% versus 86.1% for the STARFlex device.10,11
Furthermore, the STARFlex occluder is associated with a rate of device thrombus ranging from 7-10%, while the same studies have reported a 0% rate of device thrombus with the Amplatzer device.12,13 There are currently no devices approved by the FDA specifically for PFO closure. Devices are used in an ‘off-label’ manner and have been approved for closure of other atrial or ventricular defects.
Comparison of medical therapy with patent foramen ovale closure
Multiple studies have been published assessing the efficacy of percutaneous foramen ovale closure against medical therapy. These studies utilise a variety of different percutaneous PFO closure devices. Khairy et al performed a literature review of non-randomised studies analysing secondary stroke prevention in patients with a PFO over an 18-year period. It found the annual recurrence of a stroke/ transient ischaemic attack (TIA) following a PFO closure varied from 0-4.9% in the device closure group to 3.8-12% in the medical therapy group.14
Similarly, Wahl et al conducted an observational, propensity, score-matched study over 15 years which demonstrated that percutaneous PFO closure was more effective than medical therapy at preventing recurrent cerebrovascular events.15 The primary event point (composite of stroke, TIA or peripheral embolism) occurred in 11% of the closure group versus 21% of the medical therapy group (hazard ratio 0.43; 95% confidence interval 0.20-0.94; p = 0.033).
Although numerous non-randomised, single-centre trials have been published, only recently have multicentre, randomised trials been reported. The CLOSURE-1 trial and the RESPECT trials were the first prospective randomised trials designed to assess the true therapeutic role of percutaneous PFO closure.10,11
The CLOSURE-1 trial randomised patients with a cryptogenic stroke or TIA to PFO closure with a STARFlex device or medical therapy.10 The primary endpoint was stroke or TIA during two years of follow-up, death from any cause during the first 30 days, or death from neurological causes between 31 days and two years.
The primary endpoint was 5.5% in the closure group compared with 6.8% in the medical therapy group (adjusted hazard ratio 0.78%; 95% CI 0.45-1.35; p = 0.37). The rate of stroke in the device group was 2.9% versus 3.1% in the medical therapy group (p = 0.79), similarly the rate of TIA in the device group was 3.1% versus 4.1% in the medical therapy group (p = 0.44).
The rate of procedural success was 90% and effective closure, defined as trace or no residual shunt by TOE, was achieved in 86% of cases with the STARFlex device. Interestingly, the incidence of atrial fibrillation was significantly higher in the device arm compared to the medical arm (5.7% versus 0.7%, p = 0.001), and thrombosis associated with the device was seen in 1% of patients, suggesting the device was imperfect.
Nonetheless, the CLOSURE-1 trial concluded that there was no statistical difference between device closure with the STARFlex septal closure system versus medical therapy alone at preventing recurrent stroke or TIA in patients with cryptogenic stroke or TIA who have a PFO.
The RESPECT trial randomised patients aged 18-60 with a PFO and cryptogenic stroke to PFO closure with an Amplatzer device or medical therapy.11
The primary endpoints were recurrence of non-fatal ischaemic stroke, fatal ischaemic stroke and early post-randomisation death defined as all-cause mortality.
The results of the trial showed that two-year event rates were low in both groups, in the device group 1.6% versus 3% in the medical therapy group. However, there was a trend towards a long-term reduction in events in the device group: 2.21% versus 6.4% in the medical group. The study also showed a clinical risk reduction of stroke using the Amplatzer device: 46.6% versus 72.7% in the medical therapy group.
Notably, there was a favourable trend towards PFO closure in patients with a substantial right-to-left shunt and concomitant PFO and ASA. The RESPECT trial concluded that in a carefully selected group of patients with a cryptogenic stroke and PFO, there was evidence of benefit in stroke risk reduction from closure with the Amplatzer PFO occluder over medical therapy, with very low device and procedural related risks.
Figure 2. Positive bubble study, with opacification of RA and RV, showing flow of contrast from RA into LA directly across PFO in IAS (indicated by arrow)(click to enlarge)
Interpretation of the clinical trials
Several limitations have been identified in relation to the CLOSURE-1 trial. These limitations primarily relate to the study design, device implanted and patient inclusion criteria. Slow enrolment into the CLOSURE-1 trial resulted in a change in the number of patients from 1,600 to 900, which may have caused the study to be underpowered. There was a difference in the medical therapy offered to the PFO closure group and control arm introducing a confounding effect on the study endpoints.
Furthermore, patients were followed up for two years for a life-long structural abnormality, a relatively shorter period of time compared with the eight-year follow-up in the RESPECT trial. The clinical significance of the size of the shunt was questionable in the CLOSURE-1 trial, with 42% of the shunt being trivial. However, the RESPECT trial found that closure of a substantial right-to-left shunt was associated favourably with a reduction in cryptogenic stroke recurrence compared with medical therapy. The primary endpoint in the RESPECT trial was stricter than the CLOSURE-1 trial, requiring radiological evidence of stroke.
Meanwhile, the CLOSURE-1 trial allowed a clinical definition of a TIA, but not image-confirmed, as a primary endpoint. Overall, 86% of patients in the CLOSURE-1 trial had alternative explanation for their TIA or stroke, including new-onset atrial fibrillation, thrombus in LA etc. This implies a significant proportion of the primary endpoints in the CLOSURE trial was of mixed aetiology and not cryptogenic in nature.
Figure 3. Amplatzer device visualised on IAS obliterating PFO (indicated by arrow)(click to enlarge)
Figure 4. Negative bubble study: RA and RV opacified by contrast (agitated saline) with elimination of flow across IAS(click to enlarge)
Conclusion
The clinical decision to proceed and offer a patient a percutaneous PFO device closure is not straightforward. The recently presented results of the RESPECT trial demonstrate that in a carefully selected group of patients with cryptogenic stroke, percutaneous PFO closure with Amplatzer device may be beneficial over best medical therapy in the long term.
However, suitable patients must be identified only after extensive investigation and exclusion of other stroke mechanisms.
Close consultation between the stroke physician, the cardiologist and the patient is imperative. Patients need to have informed consent regarding the small but real long-term stroke risk reduction with percutaneous closure over medical therapy, as well as the potential device and procedural complications which may occur.
References
Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale during the first 10 decades of life: an autopsy study of 965 normal hearts. Mayo Clin Proc 1984; 59(1): 17-20
Alsheikh-Ali AA, Thaler DE, Kent DM. Patent foramen ovale in cryptogenic stroke: incidental or pathogenic? Stroke 2009; 40(7): 2349-2355
Lamy C, Giannesini C, Zuber M et al. Clinical and imaging findings in cryptogenic stroke patients with and without patent foramen ovale: the PFO-ASA Study. Atrial Septal Aneurysm. Stroke 2002; 33(3): 706-711
Kristensen B, Malm J, Carlberg B et al. Epidemiology and etiology of ischemic stroke in young adults aged 18 to 44 years in northern Sweden. Stroke 1997; 28 (9): 1702-1709
Sacco RL, Ellenberg JH, Mohr JP et al. Infarcts of undetermined cause: the NINCDS Stroke Data Bank. Ann Neurol 1989; 25(4): 382-390
Handke M, Harloff A, Hetzel A et al. Patent foramen ovale and cryptogenic stroke in older patients. N Engl J Med 2007; 357(22): 2262-2268
Bridges ND, Hellenbrand W, Latson L et al. Transcatheter closure of patent foramen ovale after presumed paradoxical embolism. Circulation 1992; 86 (6): 1902-1908
Harms V, Reisman M, Fuller CJ et al. Outcomes after transcatheter closure of patent foramen ovale in patients with paradoxical embolism. Am J Cardiol 2007; 99(9): 1312-1315
Staubach S, Steinberg DH, Zimmerman W et al. New onset atrial fibrillation after patent foramen ovale closure. Catheter Cardiovasc Interv 2009; 74(6): 889-895
Furlan A, Reisman M, Mauri L et al. Closure or medical therapy for cryptogenic stroke with patent foramen ovale. N Engl J Med 2012; 366(11): 991-999
Carroll JD, Saver JL et al. RESPECT Clinical Trial: Randomized Evaluation of Recurrent Stroke Comparing PFO Closure to Established Current Standard of Care Treatment. Available at: http://www.sjm.com/respect-data.aspx [accessed 24 Jan 2013]
Von Bardeleben RS, Richter C, Schnabel R et al. Long term follow up after percutaneous closure of PFO in 357 patients with paradoxical embolism: Difference in occlusion systems and influence of atrial septum aneurysm. Int J Cardiol 2009; 134(1): 33-41
Krumsdorf U, Ostermayer S, Bilinger K et al. Incidence and clinical course of thrombus formation on atrial septal defect and patient foramen ovale closure devices in 1,000 consecutive patients. J Am Coll Cardiol 2004; 43(2): 302-309
Khairy P, O’Donnell CP, Lanzberg MJ et al. Transcatheter closure versus medical therapy of patent foramen ovale and presumed paradoxical thromboemboli: a systematic review. Ann Intern Med 2003; 139 (9): 753-760
Wahl A, Jüni P, Praz F et al. Long-term propensity score-matched comparison of percutaneous closure of patent foramen ovale with medical treatment after paradoxical embolism. Circulation 2012; 125(6): 803-812
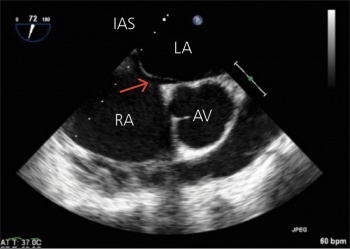 Figure 1. Tunnel PFO visible between RA and LA (red arrow)(click to enlarge)
Figure 1. Tunnel PFO visible between RA and LA (red arrow)(click to enlarge)


