While the stigma associated with epilepsy is well known, the emotional impact of the condition on the individual is less well reported
Dr Ray O'Connor, GP, Kileely, Limerick, Dr Michael Griffin, GP, Limerick City, Ireland, Ms Jennifer Mullen, Enterprise Research Centre, University of Limerick, Limerick, Dr Breda Carroll, Specialist Training Programme in General Practice, , Mid-West, Dr Gerard Garrett, Specialist Training Programme in General Practice, , Mid-West, Dr Sinéad Gavin, Specialist Training Programme in General Practice, , Mid-West, Dr Gráinne McNally, Specialist Training Programme in General Practice, , Mid-West, Dr James Moloney, Specialist Training Programme in General Practice, , Mid-West, Dr Toireas Moriarty, Specialist Training Programme in General Practice, , Mid-West, Dr Ciara O'Riordan, Specialist Training Programme in General Practice, , Mid-West, Dr Ciara O'Sullivan, Specialist Training Programme in General Practice, , Mid-West, Mr Henry Smithson, Department of General Practice, University College, Cork and Dr Michael Griffin, Specialist Training Programme in General Practice, , Mid-West
AN ESTIMATED 37,000 to 40,000 people in Ireland suffer from epilepsy.1 Epilepsy is unique among chronic conditions because of the associated stigma and psychosocial burden in addition to the physical effects of the disease.2 Epilepsy treatment often focuses primarily on seizure control often ignoring the emotional and psychosocial impacts of living with epilepsy. These include a high rate of mental health problems, mood disorders, suicide, social isolation, feelings of shame and guilt, family and social dishonour, poor self-esteem, anxiety, depression and pessimism.3 Evidence suggests that people with epilepsy are at an increased risk of psychosocial problems, lowered self-esteem, low self-confidence and are more likely to be unemployed.4,5
In particular, patients are troubled by the unpredictability and severity of their seizures; their medication; the inability to drive; and possible stigma and social consequences.6 People with epilepsy may isolate themselves as a result of the stigma associated with the condition and the fear of having a seizure in public.3 In previous work exploring the experiences of healthcare professionals providing epilepsy care in Ireland, a belief that epilepsy remains a taboo subject, with many patients feeling socially stigmatised, was identified.7 There is a paucity of research that focuses on exploring the individual’s experience of epilepsy in Ireland.
Study design
Our study adopted a qualitative design using interpretative phenomenological analysis (IPA).8 A purposive sample of 12 people with epilepsy was recruited to the study. Participants were recruited from disease registers at seven general practices associated with the HSE Mid-West/University of Limerick Specialist Training Programme in General Practice in June 2014. All were currently on treatment for epilepsy and attended their GP regularly for monitoring purposes and thus were considered to be representative of patients with epilepsy managed in the community. Study inclusion criteria were: aged 18 years or over, diagnosed with epilepsy for at least one year and able to provide written informed consent. The letter of invitation to eligible patients included an information leaflet outlining the aims and objectives of the study together with a consent form. The sample size was at the upper limit of the number of participants advocated for studies employing IPA.9
Qualitative methods
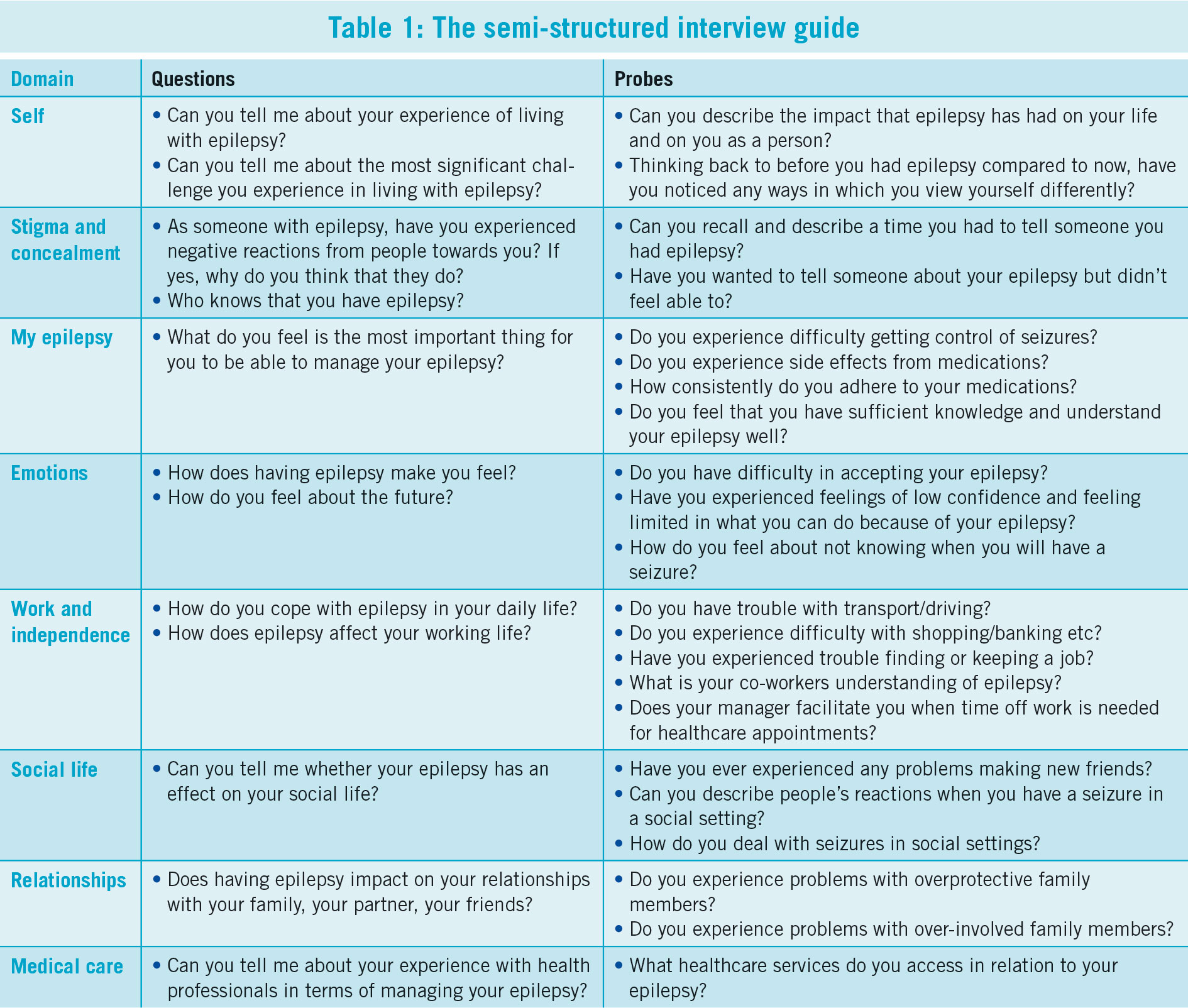
Semi-structured one-to-one interviews were conducted with consenting participants, where the intention was to guide each individual to talk about, and explore as fully as possible the meaning of living with epilepsy. The interview was guided by open-ended questions, and prompts were used, where required, to facilitate disclosure (see Table 1).
(click to enlarge)
Analysis
In line with established IPA methodology,10 the transcripts were read through several times to record initial ideas and reactions to the data. Emergent themes were identified, and illustrated using quotes. Finally, connections amongst themes were described.
Results
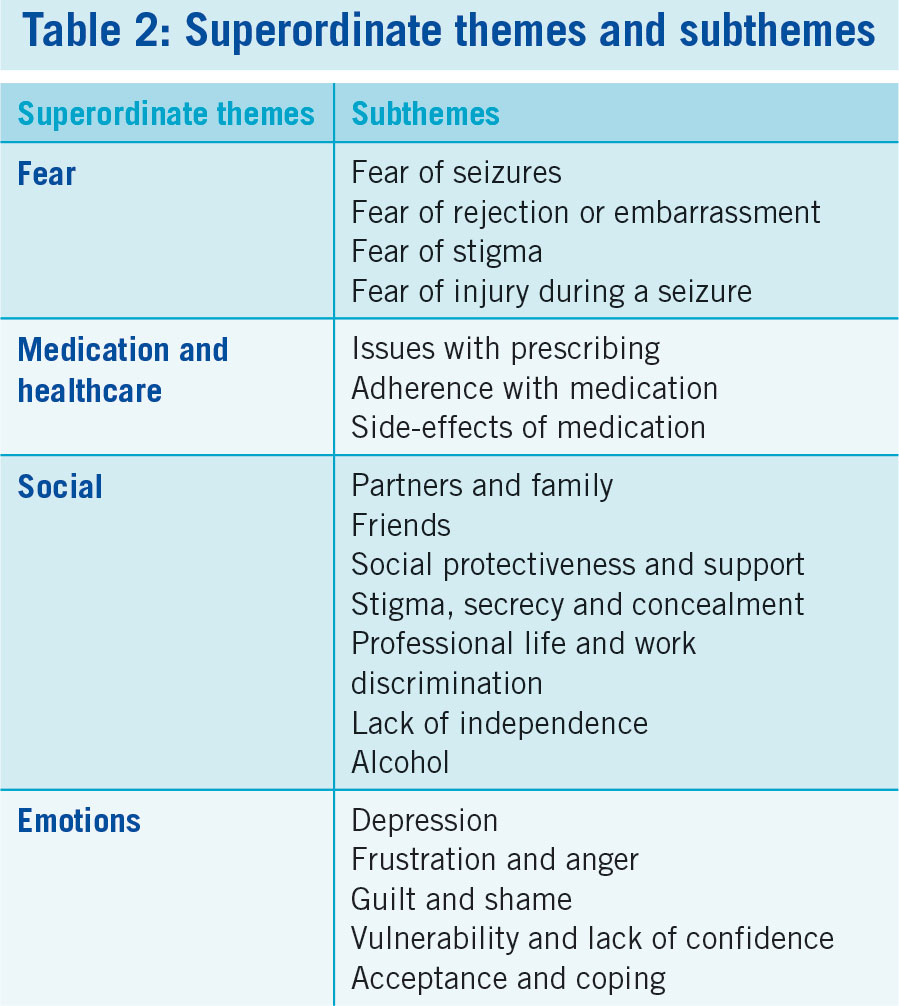
Analysis of the transcripts identified superordinate themes and their sub-themes and these are summarised in Table 2. Fear was a recurrent theme in all of the interviews and extended across many areas. Fear of seizures was the predominant fear expressed and was closely associated with the fear of being alone during a seizure: “It’s a frightening sensation knowing it could come on you at the spur of the moment.”
(click to enlarge)
All of the participants expressed a fear of rejection and many were selective about whom they disclosed their diagnosis to: “No, my family knows alright but I don’t want to mention it to anybody else.” Feelings of embarrassment or fear of being embarrassed by having a seizure were common.
The third most common fear expressed by our participants was a fear of the stigma surrounding epilepsy. Many having noted that they experienced stigma due to their diagnosis: “it’s called ‘the fits’. Years ago they would say ‘you are mad’ wouldn’t they, that you have the fits”.
Fear of injury during a seizure was a concern for more than half of the participants especially if they were alone: “I could fall down the stairs, you know, anything could happen”.
Medication
Medication and its complications was a major theme. The perceived importance of the doctors’ role regarding medication was evident in most interviews: “I would love to reduce them [medication] but I do not want to without getting the doctor’s advice”. Most appeared aware of the importance of medication adherence “[it’s] habit at this stage to take my medication.” The severity with which participants suffered negatively from side effects varied. Despite this, many were unwilling to make medication changes.
Social
Epilepsy affected many participant’s relationships whether personal, socially or professionally.
Female participants were especially concerned about how their condition would affect their children “the three kids, you know, they are the ones that are reminding me to take my tablets and they are the ones that are actually finding me having a seizure so I’m hurting them and I’m scaring them.” Participants often felt they were a burden or worry for close family members “I don’t feel my seizures, but my family… (it’s) a lot of stress for them when they see me with the seizures.” Some mentioned that they were anxious about telling potential partners, for fear of being rejected. In most cases people had been more understanding than had been anticipated “I think having to tell my wife was probably the biggest thing I had to do… it was great the way that she took it.”
Nearly all reported that close friends knew about their epilepsy. Some did not tell friends at once, but waited for a suitable time and the reactions from friends tended to be positive “my friends, I wouldn’t tell them… but when the time is right, you know, you would fit it into conversation then.”
Many participants described instances where they felt over- protected by family and partners, however, the majority perceived this as a benevolent gesture “I mean my mother is always looking out for me, my mother and father, but not too overprotective, just make sure I’m OK … I suppose looking out for me.” Approximately two-thirds of participants felt the impact of epilepsy as a stigma on their lives. It often correlated with the attitudes and opinions of others “I was very popular, got the first seizure and it was like then suddenly overnight everything changed.”
The majority of study participants felt epilepsy had no effect on their working lives: “I have never been restricted in work at all, I tell everybody at work.” However, a minority that did experience discrimination were greatly affected. The negative impact on employment often stemmed from the perceived stigma associated with the disease “I got a seizure… then I was called up and they said ‘you never told us you had epilepsy’… everyone saw the seizure… so I left.”
For many participants,having epilepsy meant their independence was limited: “I think the most significant challenge with epilepsy is that it takes away your independence because I can’t drive and I am depending on people.”
A minority of participants experienced negative reactions to a public seizure, where the public assumed a link with alcohol: “People have laughed and then just assumed I was drunk on the street.” All participants reacted emotionally to living with epilepsy: “you get over the sickness part of it, you know … but it’s the emotional long-term effect for me … that really affected my childhood, my adult life, everything.”
Participants’ feelings of depression were mainly attributed to their seizures: “I was getting depressed… it affected everything” and was often linked with a lack of confidence: “It [epilepsy] knocked down my confidence, then I’d get a bit depressed, so it was like one feeding the other.”
Anger and frustration were frequently associated with the fear of having a seizure: “the anger would still be there. Why is this happening to me?” Participants were particularly frustrated when they experienced a seizure following a seizure-free interval.
Participants experienced feelings of guilt and shame: “I remember the first time … the doctor said ‘you know you’ve epilepsy’, my mother started roaring and crying, and I said ‘I’m sorry’”. The unpredictability of seizures led to feelings of vulnerability for some: “totally vulnerable, because when you’re in the middle of that seizure, anyone could do anything to you, you’re totally vulnerable.”
Often the degree of acceptance was related to seizure-free duration and epilepsy control: “My day-to-day life hasn’t changed at all.” The lack of understanding in the general population, including their families, often hindered open acceptance of diagnosis: “I have a sister and she won’t even come into town with me. It’s an embarrassment.”
Discussion
Our findings highlight several themes which have not been extensively reported. While the stigma associated with epilepsy is well established,11 the emotional impact is less well defined in the literature. Fear of seizures, rejection, embarrassment and stigma arose in all patient interviews we conducted, a finding which no doubt impacts negatively on a person’s mental health and explains why people with epilepsy have a higher rate of mental illness.12
Strengths of the study were that all selected patients fully participated in the study process and the sample size was at the upper limit of the number of participants advocated for studies employing IPA.9 One important limitation is the sourcing of patients from a single region in Ireland. However as all patients selected were living in the community, attending their GP and being regularly monitored for their epilepsy, we believe that their experiences and our findings are readily transferable to the general population.
Traditionally, the measure of quality of life for people with epilepsy has focused on seizure frequency and severity.13,14 Recently, there have been increasing numbers of studies addressing the emotional and psychological impact of the condition, with the CREST project being one of several attempting to address the stigma associated with epilepsy internationally.15 Our study is the first to evaluate the above factors in an Irish population. One of the aims was to examine these intangible aspects of epilepsy with a view to informing an update of the current guidelines of the ICGP.16
An important overlap is noted between feelings of fear and issues affecting medication adherence and side effects. Due to the adverse impact of medicine non-adherence, this presents an important area to explore in future research, particularly in light of the Irish data showing a preference to adherence, despite a recent study showing that non-adherence depends on balancing the perceived necessity of taking anti-epileptic drugs (AED) and the concern about long term use of AED.17 Further prospective exploration may determine if medicines attitudes in an Irish population differ from other European data. Of note also was a relationship between feelings of stigma, the perceived need for secrecy and concealment felt by some patients, and feelings of discrimination, both socially and in a work life context. Discrimination against epilepsy patients is well documented in the literature,11 and our study is no exception. Many interviewees perceived themselves to be a ‘burden’ to their families and stated that epilepsy affected them in forming relationships.
The further development of epilepsy services in Ireland is outlined in ‘The Draft National Model of Epilepsy Care Programme in Ireland’.18 Our findings highlight that the implementation of a model of care that addresses complex biopsychosocial needs, and does so on a basis that is accessible to all, is a priority.
Conclusion
Our findings highlights themes which have not been extensively reported. While the stigma associated with epilepsy is well established,11 the emotional impact is less well defined in the literature. Fear of seizures, rejection, embarrassment and stigma arose in all patient interviews we conducted, a finding which no doubt impacts negatively on a person’s mental health and explains why people with epilepsy have a higher rate of mental health illnesses.12
An important overlap is noted between feelings of fear and issues affecting medication adherence and side effects. This presents an interesting avenue to explore in future research. Of note also was a relationship between feelings of stigma, the perceived need for secrecy and concealment felt by some patients and feelings of discrimination both socially and in a work-life context. Discrimination against people with epilepsy is well documented in the literature,11 and our study is no exception.
(This study was approved by the Research Ethics Committee of University Hospital Limerick and was financially supported by a grant from the ICGP Research and Education Foundation).
References
Linehan C, Kerr MP, Walsh PN, Brady G, Kelleher C, Delanty N, Dawson F, Glynn M: Examining the prevalence of epilepsy and delivery of epilepsy care in Ireland. Epilepsia 2010, 51(5):845-852.
Kale R: Bringing epilepsy out of the shadows. BMJ : British Medical Journal 1997, 315(7099):2-3.
McCagh J, Fisk JE, Baker GA: Epilepsy, psychosocial and cognitive functioning. Epilepsy Research 2009, 86(1):1-14.
Jacoby A: Stigma, epilepsy, and quality of life. Epilepsy & Behavior 2002, 3(6, Supplement 2):10-20.
Jacoby A, Austin JK: Social stigma for adults and children with epilepsy. Epilepsia 2007, 48:6-9.
Moore PM, Baker GA: The neuropsychological and emotional consequences of living with intractable temporal lobe epilepsy: implications for clinical management. Seizure 2002, 11(4):224-230.
Varley J, Delanty N, Normand C, Coyne I, McQuaid L, Collins C, Boland M, Grimson J, Fitzsimons M: Epilepsy in Ireland: Towards the primary–tertiary care continuum. Seizure 2010, 19(1):47-52.
Smith JA, Flowers P, Larkin M: Interpretative Phenomenological Analysis: Theory Method and Research. London: Sage; 2009.
Brocki JM, Wearden AJ: A critical evaluation of the use of interpretative phenomenological analysis (IPA) in health psychology. Psychology & Health 2006, 21(1):87-108.
Smith J, Osborn M: Interpretative phenomenological analysis. In Qualitative Psychology: A Practical Guide to Methods. Edited by Smith J. London: Sage; 2003.
Fernandes PT, Snape DA, Beran RG, Jacoby A: Epilepsy stigma: What do we know and where next? Epilepsy & Behavior 2011, 22(1):55-62.
WHO: Neurological Disorders: Public Health Challenges. Geneva: WHO Press; 2006. http://www.who.int/mental_health/publications/neurological_disorders_ph_challenges/en/. Accessed 15 Jan 2015.
Leidy N, Elixhauser A, Vickrey B, Means E, Willian M: Seizure frequency and the health-related quality of life of adults with epilepsy. Neurology 1999, 53:162-166.
Mulhern B, Rowen D, Jacoby A, Marson T, Snape D, Hughes D, Latimer N, Baker GA, Brazier JE: The development of a QALY measure for epilepsy: NEWQOL-6D. Epilepsy & Behavior 2012, 24(1):36-43.
Collaborative Research on Epilepsy Stigma (CREST). http://www.globalcampaignagainstepilepsy.org/activities/other-initiatives/crest/. Accessed 12 Jan 2015.
O'Connor R, Cox J, Coughlan M: Guidelines for the diagnosis and management of epilepsy in general practice. Irish College of General Practitioners (ICGP); 2001.
Chapman S, Horne R, Chater A, Hukins D, Smithson WH. Patients' perspectives on antiepileptic medication: Relationships between beliefs about medicines and adherence among patients with epilepsy in UK primary care. Epilepsy and Behavior Vol 31 Feb 2014 312-320
 (click to enlarge)
(click to enlarge)