External beam therapy, hormonal therapy and brachytherapy are different treatment options for prostate cancer patients. This article discusses the patient eligibility criteria for each treatment
Dr Ciara Lyons, Specialist Registrar in Radiation Oncology, St Luke’s Radiation Oncology Network, Dublin and Dr Brian O'Neill, Consultant Radiation Oncologist, Beaumont Hospital, Dublin
The incidence of prostate cancer has risen dramatically in Ireland in recent years, from 1,097 cases in 1994 to 2,859 cases in 2009. A further increase in incidence is expected with an ageing Irish population and increasing rates of screen-detected cancers. Rapid access prostate clinics have been established in the eight specialist cancer centres located throughout the country, facilitating prompt diagnosis and allowing direct access to multidisciplinary teams.
Risk group classification
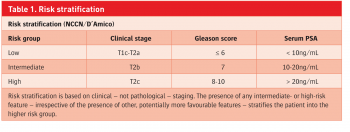
Men with biopsy-proven prostate cancer are stratified into risk groups based on three primary factors: clinical stage, pre-biopsy PSA and Gleason score (see Table 1).1 This classification is ideal for patient counselling as it is simple, validated, prognostic and indicates appropriate treatment options. Nomograms are available free online to indicate survival based on diagnostic criteria and treatment option chosen.2 Although staging varies between centres, intermediate- and high-risk patients are generally staged with MR pelvis and isotope bone scan. A CT thorax/abdomen is often considered for high-risk patients.
(click to enlarge)
(click to enlarge)
Men with prostate cancer have a number of radical treatment options open to them. Decisions on management are made in a multidisciplinary setting and are based on a number of factors, including patient preference, risk category, age and projected life expectancy, comorbidities and performance status. Established options for radical management include radical prostatectomy, radiotherapy with or without hormonal therapy, and active surveillance (as distinct to watchful waiting). There are advantages and disadvantages to all modalities of treatment and patients will require a number of discussions with the multidisciplinary team and GP prior to making a decision on their management.
Radical prostatectomy is appropriate for low- and intermediate-risk categories, and selected high-risk patients. Advantages include effective long-term control, more precise pathological staging, option of a pelvic lymph node sampling, timing convenience compared to external beam radiotherapy and, for intermediate-risk patients, the opportunity to avoid hormonal therapy. Disadvantages are general anaesthesia, operative risks, impotence risk and a small risk of long-term urinary incontinence (2-5%).
Active surveillance is based upon meticulous observation for carefully selected low-risk patients. The eligibility criteria for active surveillance at Beaumont Hospital are:
cT1c only
Initial PSA < 10ng/ml
Gleason score ≤ 6 in one or two cores only and < 50% of most involved core
PSA density < 0.2
Age between 55 and 75 years.
Patients are required to attend regularly for examination, PSA monitoring and repeat biopsy. Advantages are a reduction in over-treatment, with the potential to avoid or at least postpone radical treatment and thereby categorically preserve potency and continence. Disadvantages are the necessity for regular review and repeat biopsy, the possibility of an undetected higher grade lesion, and for some patients this process is psychologically difficult.
The eligibility, risks and benefits of radiotherapy options are summarised in Table 2. Multiple retrospective reviews confirm similar overall control rates (using modern radiotherapy techniques, at doses > 72Gy) for radiotherapy and radical prostatectomy. Although randomised comparisons between modalities are lacking, the PROTECT study in the UK has successfully and uniquely randomised over 1,500 patients to surgery, radiotherapy or ‘active monitoring’. As these results mature over 10-15 years they will provide a valuable insight.
(click to enlarge)
Sexual function and lower urinary tract symptoms (LUTS) should be evaluated at presentation and both during and after treatment. A tool developed by the American Urological Association (AUA) – the International Prostate Symptom Score (IPSS)3 quantifies the severity of LUTS and is one of the criteria used for assessment of suitability for brachytherapy. Recovery of sexual function post-therapy is dependent on a number of factors, especially baseline function, comorbidities, age and the use of hormone therapy.
External beam radiotherapy
External beam radiotherapy (EBRT) is delivered at a standard dose of 74 Gray in 37 daily 10-minute fractions over 7.5 weeks (excluding weekends). Unlike other tumour sites, chemotherapy is never delivered with radical radiotherapy. EBRT uses CT-based planning to precisely target the prostate and seminal vesicles while ensuring that the dose the surrounding normal tissues, especially the rectum and bladder, remain within safe limits (see Figure 1).
Figure 1. An axial slice through a standard 3D conformal CT plan delivering radical radiotherapy for prostate cancer. The highest doses are represented in red (seen encircling the targeted prostate) and the lowest in blue(click to enlarge)
MRI is carefully referenced to ensure extra-prostatic disease is encompassed (extra-capsular extension, seminal vesicle involvement, malignant lymph nodes).
Figure 1 is an axial slice through a standard 3D conformal CT plan delivering radical radiotherapy for prostate cancer. The highest doses are represented in red (seen encircling the targeted prostate) and the lowest in blue.
There have been a number of advances in the planning and delivery of radiotherapy that allow the delivery of higher radiation doses to the tumour while sparing surrounding normal tissue, thus reducing the risk of short- and long-term toxicity.
Intensity-modulated radiation therapy (IMRT) exploits multiple small beams of variable intensity to very accurately target complex tumour volumes, while again sparing normal tissues. A CT scanner, known as a cone-beam CT, is a feature of modern linear accelerators. At regular intervals immediately prior to delivery of treatment a cone-beam CT is taken, allowing fine-tuning to account for prostate movement due to factors such as changes in rectal volume. This is known as image-guided radiation therapy (IGRT).
More sophisticated methods of treatment delivery require increased input in the planning stages and, often, longer times for treatment delivery.
Eligibility for EBRT is summarised in Table 2. There is no PSA limit once disease has not metastasised, as recently two large randomised trials have confirmed a survival advantage for the addition of EBRT to hormonal therapy, even for very high-risk patients.4,5
IMRT has allowed even node positive patients to be treated with very acceptable toxicity. Side-effects during treatment are typically mild and build up on a cumulative basis peaking toward the end and just after completion of treatment. Most patients report mild proctitis, increased urinary frequency and dysuria. Up to 30% of men will experience rectal bleeding months after treatment, though this is treatable and very rarely clinically significant.
Radiotherapy has been proven to improve survival in the post-operative setting for men with high-risk features post radical prostatectomy. In some cases if post-operative PSA is undetectable, radiotherapy may be reserved for a ‘salvage’ setting if PSA starts to rise.
Hormonal therapy
Hormonal manipulation plays a critical role in the management of locally advanced and metastatic prostate cancer. Like the majority of breast cancers, prostate cancer is exquisitely hormone-sensitive, in this case to testosterone. Multiple agents may be used to suppress its endogenous production. Commonly used agents include anti-androgens and LHRH analogues, which interrupt both the production and action of testosterone.
There are specific systemic toxicities associated with their use, particularly in the longer term. Common toxicities include vasomotor symptoms, weight gain, loss of libido and impotence. Concerns have been raised regarding an increased risk of cardiovascular disease with the use of hormone therapy. A large US randomised trial – RTOG 94-08 – showed no excess deaths from cardiac causes in almost 2,000 men randomised to radiotherapy with four months hormonal therapy versus radiotherapy alone.6
These results are confirmed by a recent meta-analysis.7 An increased risk of osteoporosis occurs with longer-term therapy and the US National Comprehensive Cancer Network currently recommends a baseline DEXA scan along with calcium and bisphosphonate supplementation as required. Low-risk patients are treated with radiotherapy or brachytherapy alone.
Intermediate-risk patients are generally treated with radical radiotherapy and hormonal therapy for a total of six months. Typically combined therapy with an LHRH analogue and an anti-androgen will start two to four months prior to radiotherapy. High-risk patients benefit from longer-term hormonal therapy for two to three years. These strategies have demonstrated profound survival advantages within multiple large-scale randomised trials. For example, in RTOG 94-08 5% more men were alive at 10-year follow-up in the arm that received hormonal therapy, although this benefit was not seen in low-risk patients.
Brachytherapy
Brachytherapy is a form of radiation therapy where radioactive sources are implanted directly into the tumour and surrounding prostate tissue. It is primarily indicated for patients with organ-confined low-risk cancers. It may also be an option in combination with EBRT for higher-risk tumours. It maximises radiation dose directly to the tumour, while minimising doses delivered to surrounding normal tissues. Unlike EBRT, it generally requires only two visits, for initial assessment and subsequent transperineal implantation of radioactive sources, under general anaesthetic (see Figure 2).
Figure 2. The placement of radioactive seeds directly into the prostate under transrectal ultrasound guidance via a standard transperineal approach (courtesy of Dr Jerome Coffey, Consultant Radiation Oncologist, St Luke’s Radiation Oncology Network)(click to enlarge)
Either low-dose rate or high-dose rate therapy may be used. Low-dose rate therapy is more commonly available; seeds of iodine-125 or palladium-103 are permanently implanted into the prostate under ultrasound guidance. These isotopes emit low energy radiation with a very short range. This allows delivery of high doses to the prostate while minimising the dose delivered to the bladder and rectum. Alternatively, a high-dose rate source, iridium-192, can be temporarily introduced into the prostate (via hollow transperineal catheters).
Selected patients are considered for brachytherapy based on both patient and tumour characteristics. In summary, men with low-risk cancers, relatively low prostate volumes and low rates of LUTS are considered suitable. Occasionally, a short course of androgen deprivation therapy may be used to shrink the prostate volume to a technically acceptable level. Control rates with brachytherapy are extremely impressive. Its relative convenience is a major advantage, while usually preserving continence and causing erectile dysfunction less frequently than surgery or EBRT.
Conclusion
The incidence of prostate cancer is expected to rise further in coming years, with widespread PSA screening, rapid diagnosis and an ageing population. There are a number of treatment options open to patients who present with non-metastatic disease. Men require counselling by the multidisciplinary team and the GP before making management decisions. This article summarises current radiotherapy options and recent advances in treatment delivery.
Warde P, Mason MD, Sydes MR et al. Intergroup randomised phase III study of androgen deprivation therapy (ADT) + radiation therapy (RT) in locally advanced prostate cancer (CaP) (NCIC-CTG, SWOG, MRC-UK, INT: T94-0110; NCT00002633) (abstract #4504). J Clin Oncol 2010; 28: 18s
Widmark A, Klepp O, Solberg A et al. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7)/SFUO-3): an open randomised phase III trial. Lancet 2009; 373(9660): 301
Efstathiou E, Paulus R, Smith R et al. Cardiovascular mortality following short-term androgen deprivation in clinically localized prostate cancer: an analysis of RTOG 94-08 ASTRO 2011; Abstract 82
Nguyen PL, Schutz FA, Hoffman KE et al. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: a meta-analysis of prospective trials. JAMA 2011; 306(21): 2382-2383
 (click to enlarge)
(click to enlarge)



