Melanoma is the ninth most common invasive cancer diagnosis in Ireland. This article discusses the latest systemic therapies available for metastatic melanoma
Dr Jodie Battley, Medical Oncology Registrar, Cork University Hospital, Cork and Dr Derek Power, Consultant in Medical Oncology, Cork University Hospital, Cork
Malignant melanoma constitutes a serious global epidemic. Over the past 30 years incidence rates of malignant melanoma have been increasing. In Ireland, melanoma is the ninth most common invasive cancer diagnosis. In the past decade incidence rates have increased by 84% in males and 48% in women. The incidence for women in Ireland is one of the highest in Europe (ranking fourth highest of 26 countries tested). The incidence rate for men in Ireland is lower (eighth of 26), but remains above the European average (National Cancer Registry of Ireland, 2011).
Figure 1. RAS-RAF-MAPK pathway(click to enlarge)
Despite improvements in the understanding of risk factors and genetic causes of melanoma the prognosis remained poor for many decades and systemic therapies had no impact on survival. Before 2010, median overall survival was static at six to nine months, and three-year survival rates were 10-15%. However, recent advances in the understanding of cancer biology have seen the development of several new systemic therapies heralding an exciting new era.
BRAF inhibition
One growth factor pathway that has gained considerable attention in recent years is the RAS–RAF–MEK–ERK signalling cascade. In virtually all melanoma cases, there is an alteration at some level in the RAS signalling cascade (see Figure 1). Specifically, 40-60% of melanomas carry an activating mutation in the gene encoding the serine-threonine kinase BRAF.
These mutations are associated with increased growth and proliferation of cancer cells. Ninety per cent of BRAF mutations result in a substitution of glutamic acid for valine at amino acid 600 (the V600E mutation), most of the remainder consists of an alternate substitution at the V600 locus (V to K).
One of the key recent developments over the past decade is targeted agents that selectively or non-selectively inhibit activated BRAF. Vemurafenib, a recently licensed selective BRAF inhibitor, was initially shown to have anti-tumour activity in melanoma cell lines with the BRAF V600E mutation. Phase I and II studies demonstrated that vemurafenib had a high level of activity against advanced melanomas containing the V600E mutation.
A phase II trial in patients treated with the BRAF V600E mutation that had previously been treated with standard chemotherapy showed a response rate of 53%, median duration of response of 6.7 months, and median overall survival of 15.9 months after a median of 12.9 months follow-up.1
The pivotal phase III trial comparing vemurafenib to dacarbazine (DTIC) in treatment-naпve patients with advanced metastatic melanoma (BRIM 3), observed a significant impact on progression-free survival (PFS) and overall survival (OS). In a population of 672 evaluable for overall survival, at six months, overall survival was 84% in the vemurafenib group and 64% in the DTIC group. Response rates were 48% for vemurafenib and 5% for DTIC. In the interim analysis for OS and final analysis for PFS performed at a median of 3.8 months follow-up, vemurafenib was associated with a relative reduction in the risk of death of 63% and of 74% in the risk of either disease-free progression or death, as compared with dacarbazine (p < 0.001 for both comparisons).
Of note, the above benefits were seen in all sub-groups of patients including those with M1c disease and an elevated lactate dehydrogenase.2 However, longer follow-up is required to establish the true impact on overall survival.
Recently released phase III data from the BREAK3 study (comparing another BRAF inhibitor, dabrafenib, with DTIC in patients with BRAF V600E mutation-positive metastatic melanoma) demonstrated a 70% risk reduction in disease progression or death (HR 0.30; p < 0.0001) compared to chemotherapy with a median duration of follow-up of five months.3 The median PFS was 5.1 months in the dabrafenib arm compared to 2.7 months in the DTIC arm. Given the short follow-up overall survival data remain immature, however, the overall survival HR was 0.61 (95% CI 0.25-1.48) in favour of dabrafenib.
The most common significant side-effects reported with BRAF inhibitors are cutaneous, including:
Squamous cell carcinomas
Hyperkeratosis
Photosensitivity.
Other common side-effects include:
Fatigue
Pyrexias
Arthralgia.
In the two randomised studies grade 3 toxicities are seen in less than 10% of patients. Cutaneous toxicity is at least partly explained by the mechanism of these agents and the activation of pre-neoplastic BRAF wild type cells.
MEK inhibitors
The MAP-kinase pathway regulates proliferation and survival of melanoma tumour cells. Activated BRAF in turn activates MEK proteins which then activate downstream MAP kinases. Preclinical models have shown that MEK-inhibitors can induce cell death in melanoma cells that harbour BRAF activating mutations. The phase III METRIC study combined the oral MEK inhibitor trametinib with dacarbazine in patients with BRAF V600E or K mutation-positive metastatic melanoma.4
In an intention-to-treat population of 322 patients, median PFS of 4.8 months in the trametinib arm was significantly greater than the 1.5-month median PFS in the chemotherapy arm. This translated into a 55% reduction in risk of disease progression or death (HR 0.45; p < 0.0001) in the trametinib arm. Response rates were 22% and 8%, respectively (p = 0.01). A significant OS benefit was noted at the interim analysis (HR 0.54; p = 0.0136), however, the median overall survival was not yet reached.
The six-month overall survival rate in the intention-to-treat population was 81% and 67% for the trametinib and chemotherapy arms, respectively. The most commonly reported (20%) adverse effects in the trametinib arm were:
Rash (57%)
Diarrhoea (43%)
Fatigue (26%)
Peripheral oedema (26%).
Grade 3 toxicities were rare, however, two patients in the trametinib group had grade 3 cardiac-related events that were considered to be drug-related, resulting in permanent discontinuation of the study drug.4
BRAF + MEK inhibition combinations
One of the limitations of BRAF inhibitor monotherapy is the development of resistance due to downstream activation of the RAS-MAP kinase pathway. The rationale behind combination of BRAF inhibitors and MEK inhibitors in BRAF-mutant tumours includes:
Potential synergy in combination
Overcoming monotherapy resistance
Potentially reducing the incidence of BRAF inhibitor-induced hyperproliferative skin changes.
KIT
Melanomas arising in the mucosal, acral and chronic sun-damaged sites may harbour mutations and amplifications of the receptor tyrosine kinase, kit. A recent phase II trial reported 23% of patients with any of these melanoma subtypes harbour these genetic alterations.5
Preclinical and anecdotal activity has been reported with imatinib in kit-mutant melanoma. In this trial Carvajal and colleagues reported a durable response (over 52 weeks) rate of 16% with a median time to progression of 12 weeks and median OS of 46.3 weeks. The authors conclude that significant numbers of patients with advanced melanoma display a kit oncogene addition and can derive a meaningful clinical benefit from imatinib.
Immunotherapy
The immunogenicity of melanoma cells and the efficacy of high-dose interferon in some patients has led to ongoing exploration of immunotherapeutic agents. Ipilimumab is a human monoclonal antibody targeting the ligand CTLA-4 (cytotoxic T-lymphocyte-associated antigen 4), an immunological checkpoint on cytotoxic T-lymphocytes thought to play a critical role in regulating immune responses.
A phase III study has demonstrated improvement in OS with a median survival of 10 months in advanced melanoma patients treated with ipilimumab with or without a glycoprotein 100 (gp100) peptide vaccine, compared to 6.4 months for those treated with gp100 alone (HR for death 0.68, p < 0.001).6
There was no difference in survival in both ipilimumab groups. The use of gp100 vaccine in this study is explained by the fact that previous studies showed combination gp100 and high-dose interleukin-2 improved efficacy of the latter in advanced melanoma. It was therefore felt that gp100 was a reasonable active control given there was no accepted standard of care in advanced melanoma.
A further phase III study comparing ipilimumab with or without standard chemotherapy (DTIC) in previously untreated patients also demonstrated a significant survival benefit (11.2 versus 9.1 months, HR for death 0.72, p < 0.001) for the combination arm.7 The survival benefit was durable with prolonged survival noted in 20.8% of patients at three years in the combination arm.
Adverse events associated with ipilimumab fit with the hypothesis that blockade of CTLA-4 impairs immunologic tolerance. Defined as ‘immune-related (IR) adverse events’ these include inflammatory conditions of:
The skin (pruritis, rash, liver (hepatitis)
GI tract (colitis)
Endocrine system (hypophysitis).
Grade 3-4 IR toxicity was seen in up to 38% of patients and the most common adverse effect was increased hepatic transaminases. Grade 3-4 IR enterocolitis was seen in 12% of patients and no gastrointestinal perforations were noted. IR toxicity was generally reversible with treatment according to protocols including the administration of glucocorticoids or other immune-suppressant drugs. No treatment-related deaths were observed in the more recent randomised study.7
More recently, investigation of ‘programmed-death’ protein 1 (PD-1), a T-cell co-inhibitory receptor, and one of its ligands, PD-L1, has led to the development of antibodies that block this interaction and result in impairment of the tumour cell’s ability to evade the host’s immune system. Use of these novel antibodies may lead to durable responses in advanced melanoma.8
Brain metastases
Brain metastases commonly develop in patients with melanoma. Post-mortem studies suggest the incidence may be as high as 70%. Melanoma brain metastases confer a worse prognosis and patients are often excluded from clinical trials on this basis. Recent data have reported clinical benefit in this sub-group of patients treated with either ipilimumab or dabrafenib.9,10
Abscopal effect
Anecdotal reports of an abscopal effect suggesting a synergistic relationship between ipilimumab and radiotherapy have been reported in the recent literature. The abscopal effect is a phenomenon in which local radiotherapy is associated with regression of metastatic cancer away from the irradiated site. It is thought to be mediated by activation of the immune system with loss of stimulatory and/or immunosuppressive factors from the tumour. Postow et al report a case of a complete response in all disease sites in a patient with melanoma treated with ipilimumab and radiotherapy.11 Other anecdotes have followed this case. A trial is currently under way to further evaluate this effect (www.clinicaltrials.gov-NCT01449279)
Conclusion
Melanoma, heretofore a therapeutic desert, has become an unlikely poster child for targeted therapy.12 Many systemic therapies that provide a meaningful clinical benefit are now available for patients with advanced disease. However, many issues remain to be resolved:
Sequencing of these agents
Biomarkers for immunotherapy approaches
Potential ‘preoperative’, neoadjuvant and adjuvant approaches and finally, but probably most importantly
And finally, but probably most importantly, the cost of these agents.
Given that melanoma is a rare disease, is society prepared to pay for expensive therapies that truly benefit a few? This question is relevant to many other diseases also and raises important fiscal, ethical and therapeutic issues which urgently need to be addressed.
References
Sosman JA, Kim KB, Schuchter L et al. Survival in BRAF V600-mutant advanced melanoma treated with vemurafenib. NEJM 2012; 366: 707‑714
Chapman PB, Hauschild A, Robert C et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. NEJM 2011; 364: 2507-2516
Hauschild A, Grob JJ, Demidov LV et al. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet 2012
Flaherty KT, Robert C, Hersey P et al. Improved survival with MEK inhibition in BRAF-mutated melanoma. The New England Journal of Medicine 2012; 367: 107-114
Carvajal RD, Antonescu CR, Wolchok JD et al. KIT as a therapeutic target in metastatic melanoma. JAMA 2011; 305: 2327-2334
Hodi FS, O’Day SJ, McDermott DF et al. Improved survival with ipilimumab in patients with metastatic melanoma. NEJM 2010; 363: 711-723
Robert C, Thomas L, Bondarenko I et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. NEJM 2011; 364: 2517‑2526
Brahmer JR, Tykodi SS, Chow LQ et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. NEJM 2012; 366: 2455‑2465
Falchook GS, Long GV, Kurzrock R et al. Dabrafenib in patients with melanoma, untreated brain metastases, and other solid tumours: a phase 1 dose-escalation trial. Lancet 2012; 379: 1893-1901
Margolin K, Ernstoff MS, Hamid O et al. Ipilimumab in patients with melanoma and brain metastases: an open-label, phase 2 trial. Lancet Oncol 2012; 13: 459-465
Postow MA, Callahan MK, Barker CA et al. Immunologic correlates of the abscopal effect in a patient with melanoma. NEJM 2012; 366: 925‑931
Smalley KS, Sondak VK. Melanoma – an unlikely poster child for personalized cancer therapy. NEJM 2010; 363: 876-878
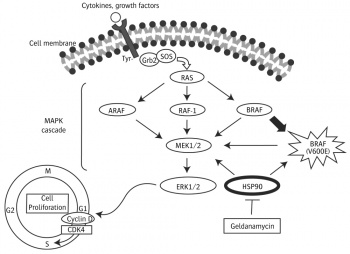 Figure 1. RAS-RAF-MAPK pathway(click to enlarge)
Figure 1. RAS-RAF-MAPK pathway(click to enlarge)