Schizophrenia, mental health legislation and human rights
Ongoing revision of mental health legislation is essential, as proposed in the review of the Mental Health Act 2001, however, the most important task is moving mental health to the centre of the public health agenda
Prof Brendan Kelly, Associate Clinical Professor of Psychiatry, Univeristy College Dublin, Dublin
Like all other mental disorders, schizophrenia is mostly treated on a voluntary, outpatient basis. However, schizophrenia is also the single most common diagnosis among people admitted as involuntary patients. In 2013, ‘schizophrenia, schizotypal and delusional disorders’ accounted for 44% of involuntary admissions in Ireland, while affective disorders (for example, depression) accounted for 28% and organic mental disorders accounted for 5%.1 On this basis, issues relating to mental health legislation and human rights are especially important for people with schizophrenia.
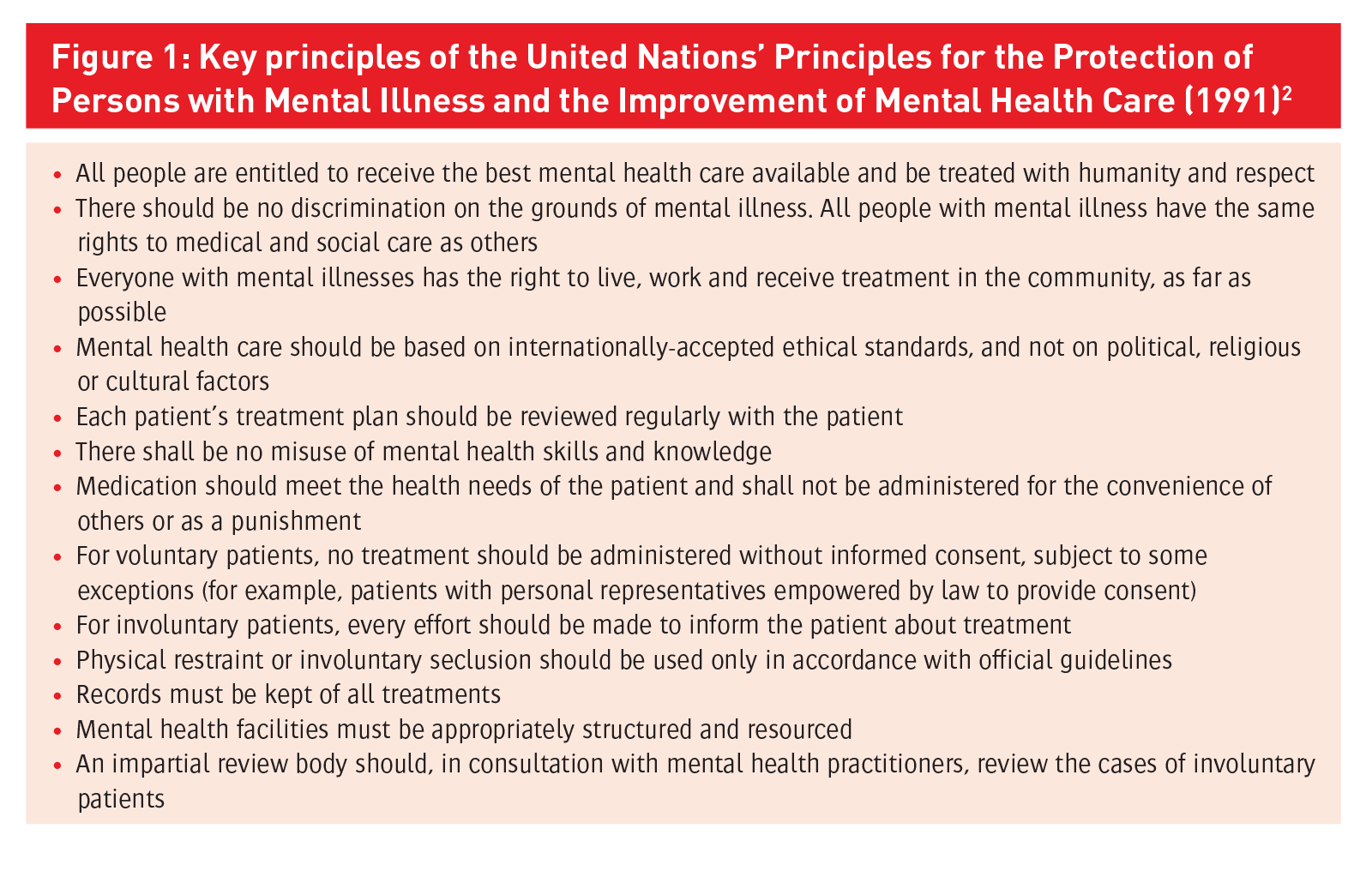
Historically, people with mental disorder, including those with schizophrenia, have experienced high levels of abuse or neglect of human rights, including the rights to liberty and treatment. The first comprehensive statement of the rights of people with mental illness was the United Nations’ (UN) Principles for the Protection of Persons with Mental Illness and the Improvement of Mental Health Care in 1991 (Figure 1).2 This statement of principles from the UN was important not only for its specific provisions, but also its acknowledgement of a particular need to protect the rights of people with mental disorder, especially people with enduring mental disorders (such as certain people with schizophrenia) whose rights have been significantly ignored in the past.
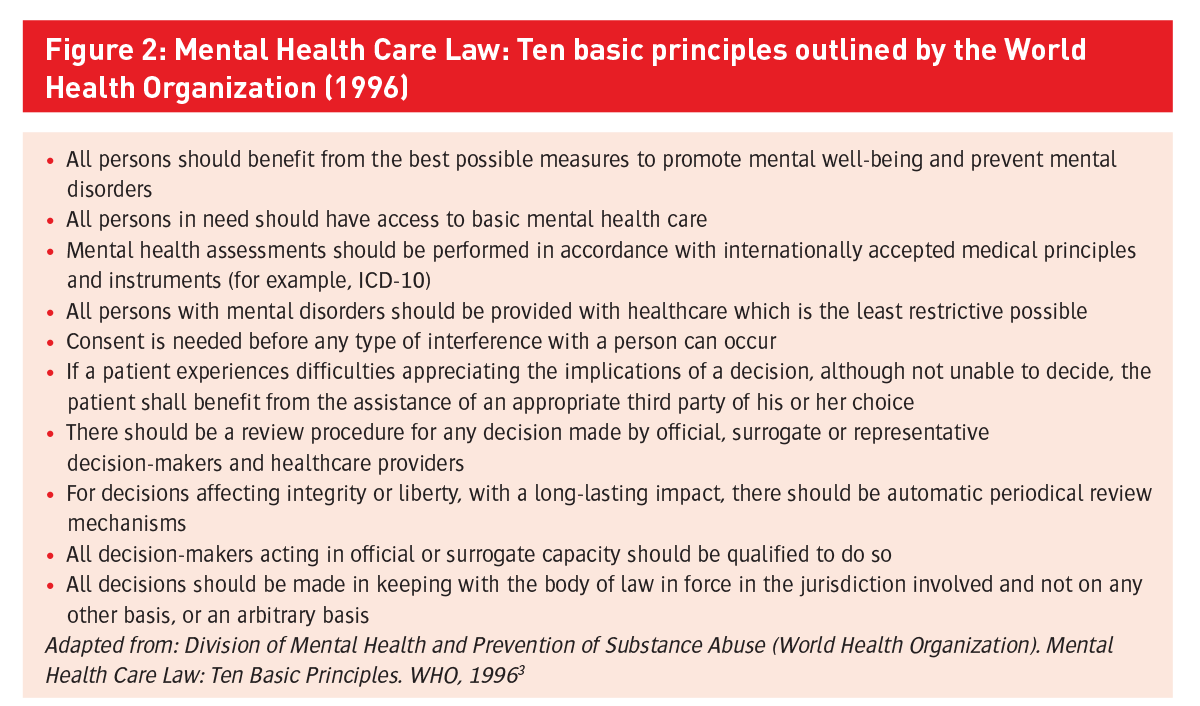
The World Health Organization (WHO) went on to articulate 10 basic principles of mental health care law in 19963 (Figure 2), further emphasising many of the 1991 principles.
Again, these principles provide important background to revisions of mental health legislation in relevant states, including Ireland.
Figure 1: Key principles of the United Nations’ Principles for the Protection of Persons with Mental Illness and the Improvement of Mental Health Care (1991)2(click to enlarge)
Figure 2: Mental Health Care Law: Ten basic principles outlined by the World Health Organization (1996)(click to enlarge)
The Mental Health Act 2001 in Ireland
Involuntary psychiatric admission and treatment in Ireland are governed by the Mental Health Act 2001, which replaced the Mental Treatment Act 1945. The 2001 legislation:
Revised involuntary admission procedures
Introduced new provisions for treatment of involuntary patients
Created mental health tribunals and the Mental Health Commission to promote high standards of care and protect the interests of involuntary patients.
Definition of mental disorder
With regard to involuntary admission, a person can be detained to an ‘approved centre’ on the grounds that he or she is suffering from a ‘mental disorder’ (for example, schizophrenia), but cannot be so detained solely on the basis that he or she has a personality disorder, is ‘socially deviant’, or is addicted to drugs or intoxicants (Section 8(1)).
‘Mental disorder’ means: “mental illness, severe dementia or significant intellectual disability where (a) because of the illness, disability or dementia, there is a serious likelihood of the person concerned causing immediate and serious harm to himself or herself or to other people, or (b) (i) because of the severity of the illness, disability or dementia, the judgment of the person concerned is so impaired that failure to admit the person to an approved centre would be likely to lead to a serious deterioration in his or her condition, or would prevent the administration of appropriate treatment that could be given only by such admission, and (ii) the reception, detention and treatment of the person concerned in an approved centre would be likely to benefit or alleviate the condition of that person to a material extent” (Section 3(1)).
Mental illness is “a state of mind of a person which affects the person’s thinking, perceiving, emotion or judgment, and which seriously impairs the mental function of the person to the extent that he or she requires care or medical treatment in his or her own interest or in the interest of other people” (Section 3(2)).
Severe dementia is “a deterioration of the brain of a person which significantly impairs the intellectual function of the person thereby affecting thought, comprehension and memory and which includes severe psychiatric or behavioural symptoms such as physical aggression”.
Significant intellectual disability is “a state of arrested or incomplete development of mind of a person which includes significant impairment of intelligence and social functioning and abnormally aggressive or seriously irresponsible conduct on the part of the person”.
Involuntary admission
In order for an involuntary admission to occur, an ‘application’ is made by a spouse, relative, health service officer, member of the police force or other person (Section 9(2)), who must have observed the patient within the previous 48 hours.
Then, the person must be examined by a doctor (for example, a GP) within 24 hours of the doctor receiving the completed application. The doctor may then complete a ‘recommendation’ on a prescribed form, and this remains valid for a period of seven days (Section 10).
At this point, the applicant arranges for the individual to be brought to a psychiatric inpatient facility. If the applicant cannot do so, the clinical director of the approved centre can arrange for the removal of the individual to the approved centre by staff of the approved centre (Section 13(2)).
If “there is a serious likelihood of the person concerned causing immediate and serious harm to himself or herself or to other people”, the police may be requested “to assist the members of the staff of the approved centre in the removal by the staff of the person to that centre” (Section 13(3)).
Once the person is in the approved centre, they must be examined by a consultant psychiatrist within 24 hours (Section 14(2)). If the consultant agrees that involuntary admission is appropriate, they complete an ‘admission order’.
If the consultant does not agree that involuntary admission is appropriate, he or she does not complete such an order. In this circumstance, the patient either leaves the approved centre or remains as a voluntary patient. An admission order, if completed, permits “the reception, detention and treatment of the patient” for up to 21 days (Section 15(1)).
Provided specific criteria are met, this admission order may be renewed for a period of up to three months (Section 15(2)); then for up to six months; and then for to 12 months (Section 15(3)). Following completion of the admission order, the consultant must inform the Mental Health Commission, triggering a mental health tribunal within 21 days.
Involuntary treatment
The Mental Health Act 2001 defines treatment as “the administration of physical, psychological and other remedies relating to the care and rehabilitation of a patient under medical supervision, intended for the purposes of ameliorating a mental disorder” (Section 2(1)).
The consent of an involuntary patient is “required for treatment except where, in the opinion of the consultant psychiatrist responsible for the care and treatment of the patient, the treatment is necessary to safeguard the life of the patient, to restore his or her health, to alleviate his or her condition, or to relieve his or her suffering, and by reason of his or her mental disorder the patient concerned is incapable of giving such consent” (Section 57(1)).
Psycho-surgery can only be performed if the patient consents in writing and surgery is authorised by a mental health tribunal (Section 58). Electroconvulsive therapy can be administered to an involuntary patient only if they consent in writing, or, if they are “unable or unwilling” to consent, if it is approved by the treating consultant psychiatrist and another psychiatrist (Section 59(1)).
Medication can be administered to an involuntary patient “for a continuous period of three months” only if the patient consents in writing, or, if the patient is “unable or unwilling” to consent, if it is approved by the treating consultant psychiatrist and another psychiatrist (Section 60).
The 2001 Act also specifies that “a person shall not place a patient in seclusion or apply mechanical means of bodily restraint to the patient unless such seclusion or restraint is determined, in accordance with the rules made under subsection (2), to be necessary for the purposes of treatment or to prevent the patient from injuring himself or herself or others and unless the seclusion or restraint complies with such rules” (Section 69(1)).
Relevant rules are published by the Mental Health Commission and are available on its website,
www.mhcirl.ie.
Mental health tribunals
Once the Mental Health Commission is notified about an involuntary admission, the Commission refers the matter to a tribunal, assigns a free legal representative to the patient, and engages an independent psychiatrist to examine the patient.
Each tribunal comprises three members: one consultant psychiatrist, one solicitor or barrister (of not fewer than seven years’ experience) and one layperson.
Within 21 days of each detention order, a tribunal reviews the order and, if satisfied that appropriate procedures were followed and the patient still has a mental disorder, affirms the order (Section 18(1)). If the tribunal is not so satisfied, it revokes the order and directs that the patient be discharged, although the patient can remain as a voluntary patient if the patient so chooses (Section 29).
Regarding appeal, a patient can appeal a tribunal decision to the Circuit Court, only “on the grounds that he or she is not suffering from a mental disorder” (Section 19(1)). A High Court appeal can proceed only “on a point of law” (Section 19(16)).
Overall, “no civil proceedings shall be instituted in respect of an act purporting to have been done in pursuance of this Act save by leave of the High Court and such leave shall not be refused unless the High Court is satisfied (a) that the proceedings are frivolous or vexatious, or (b) that there are no reasonable grounds for contending that the person against whom the proceedings are brought acted in bad faith or without reasonable care” (Section 73).
Effects of the Mental Health Act 2001
The introduction of the Mental Health Act 2001 generated significant concern among different stakeholders in Irish mental health services, most notably in terms of its apparent resource implications.
Since the 2001 Act was fully enacted in 2006, there is evidence that its requirements have indeed increased workloads for doctors, reduced time available to spend with patients, and are considered by some as not user-friendly. There is also, however, evidence that training can assist in addressing at least some of these matters.4
Notwithstanding these concerns, it is increasingly clear that the Mental Health Act 2001 increased observance of human rights and patient dignity in relation to involuntary psychiatric admission. In particular, the Act has improved Ireland’s compliance with various international human rights standards including the UN’s Principles for the Protection of people with Mental Illness and the Improvement of Mental Health Care (1991).2
More specifically, the 2001 Act fulfils some, but not all, of the human rights standards outlined by the WHO in the WHO Resource Book on Mental Health, Human Rights and Legislation.5
Areas of high compliance include the 2001 Act’s definitions of mental disorder, and robust, revised procedures for involuntary admission and treatment.
Areas of moderate compliance relate to:
Issues of competence, capacity and consent (the chief difficulties stemming from the absence of capacity legislation in Ireland)
Certain elements of mechanisms for oversight and review (which exclude long-term voluntary patients and lack robust complaints procedures).6
On the other hand, areas of low compliance with WHO standards relate to:
A general commitment to promoting rights (which affects other areas within the legislation, such as information management)
The situation pertaining to voluntary patients (especially non-protesting, incapacitated patients)
Protection of vulnerable groups and emergency treatments.
The greatest single deficit in the legislation relates to economic and social rights, which are not addressed in the legislation in any substantive fashion. These are especially relevant to people with enduring mental illness (for example, certain people with schizophrenia).
The challenge of protecting vulnerable groups through mental health legislation is an especially important one, and Irish mental health legislation does not offer specific, additional protections to the vulnerable groups highlighted by the WHO,5 including minors, women, and members of minority groups who develop mental disorders.6
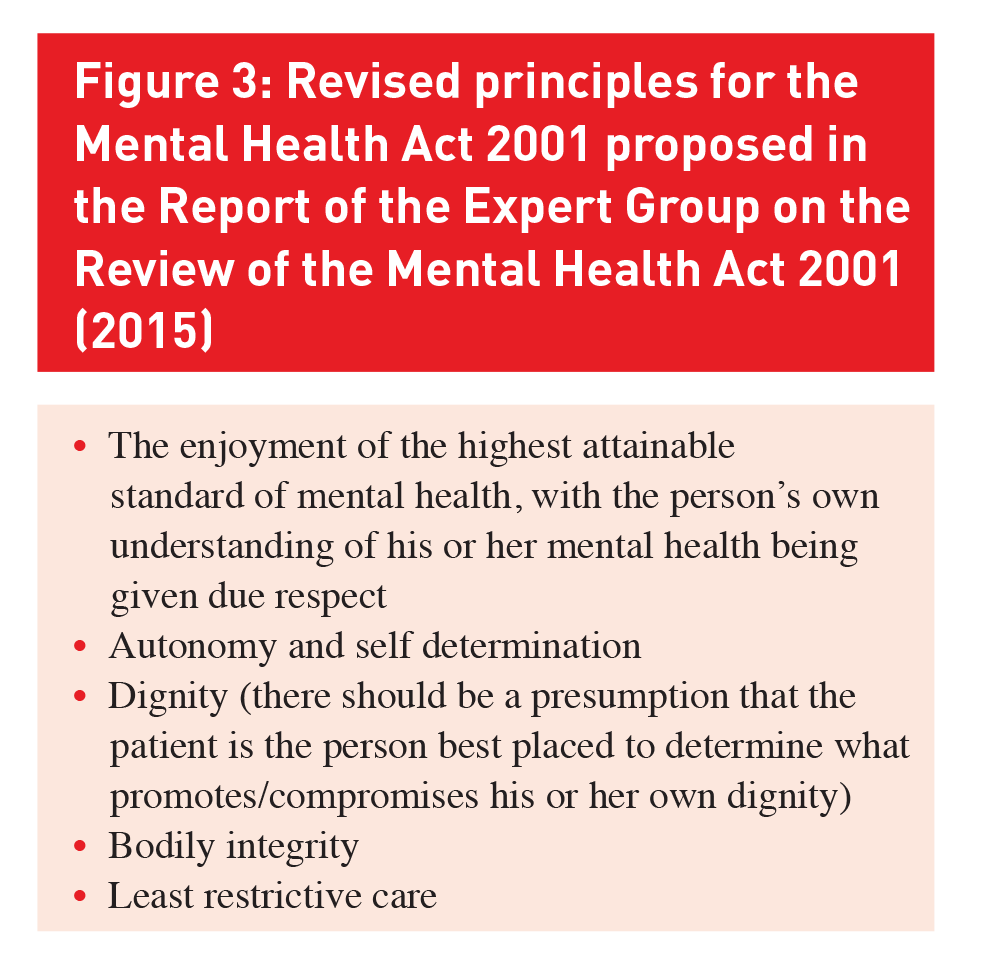
Figure 3: Revised principles for the Mental Health Act 2001 proposed in the Report of the Expert Group on the Review of the Mental Health Act 2001 (2015)(click to enlarge)
Figure 4: Revised Criteria for Involuntary Admission proposed in the Report of the Expert Group on the Review of the Mental Health Act 2001 (2015)(click to enlarge)
Proposed revisions to the Mental Health Act 2001
In July 2011 the Irish government announced a review of the Mental Health Act 2001. The review would begin with the formation of a steering group tasked with identifying key areas of the 2001 Act to be examined in more detail during the second and more detailed phase of the review. The Interim Report of the Steering Group on the Review of the Mental Health Act 2001 was published in June 2012, and informed the work of the subsequent Expert Group on the Review of the Mental Health Act 2001, which met 13 times between September 2012 and September 2014.
Kathleen Lynch, Minister for Primary Care, Social Care (Disabilities and Older People) and Mental Health, published the Report of the Expert Group on the Review of the Mental Health Act 2001 on March 5, 2015. The report presented 165 recommendations, the bulk of which relate to changes to mental health legislation.
Welcoming the thrust of the review’s recommendations, Minister Lynch said that “while the 2001 Act has served us well, we must remember that it was enacted five years before the publication of A Vision for Change (the 2006 national mental health policy) and six years before the publication of the Convention on the Rights of People with Disabilities. Both of these landmark documents have set standards based on the concept of recovery and on individuals with mental health problems having autonomy to the greatest extent possible to make their own admission and treatment decisions.”
The Minister welcomed “the recognition that, in line with our proposed capacity legislation, every effort must be made to respect decisions made by individuals with capacity who have mental health problems… The review now charts a way forward which aims to give a stronger voice to the individual and an acknowledgement that such individuals may need support to exercise their wishes.” In addition, the Minister stated she was “pleased to see that the strengthening of existing safeguards provided under the Act for those who require involuntary admission and treatment is recommended.”
The expert group recommended that revised mental health legislation should be informed by the inclusion of a revised set of principles which would replace the current legislative principal consideration of best interests (Figure 3).
The expert group also recommended that it should no longer be possible to detain someone purely because they had a significant intellectual disability. The definition of mental illness should explicitly acknowledge that it is a complex and changeable condition, with due respect for a person’s own understanding of their mental illness. It should also acknowledge that certain key decisions under the revised legislation (for example, admission of involuntary patients) should involve an assessment by at least two mental health professionals.
Revised criteria for involuntary admission were also proposed (Figure 4).
Capacity
Regarding capacity, the expert group noted that, while capacity was to be presumed for all individuals, where a formal capacity assessment determined that a person lacked capacity, this should be monitored on an ongoing basis by the treating clinicians. This was to ensure that as soon as a person regained capacity, they would be afforded the opportunity to make their treatment decisions.
It was noted that the Assisted Decision-Making (Capacity) Bill had significant proposals for all individuals in terms of capacity. This included:
The provision of support for a person to make their own decisions whenever possible
Where mental health was concerned, assessment of whether or not a person had a mental illness would, in future, be clearly separated from assessment of capacity.
The expert group recommended that a voluntary patient should be defined as a person who had capacity to make their own decisions about admission and treatment, and who gave informed consent to that admission and treatment. The 2001 Act currently regards a patient as voluntary only if that person is not subject of an admission or renewal order.
The report suggested that a new category of intermediate patient be introduced. It would ensure that people who may not warrant detention, but did not have the capacity to give informed consent may be admitted for treatment in a ‘voluntary’ capacity. They would have all the safeguards available to involuntary patients.
With regard to involuntary admission, it was recommended that the role of the ‘authorised officer’ should be expanded to include examining alternatives to inpatient treatment if available and required. Where appropriate they should initiate applications for involuntary admission.
It was recommended that mental health tribunals should be renamed Mental Health Review Boards. They should review detention orders after 14 days rather than 21 days. In addition, a psychosocial report should be carried out by a member of the multidisciplinary team for the review board.
ECT and capacity
It should no longer be possible to administer ECT to a person who has capacity and does not consent to such treatment. ECT may still be administered in future, but in all cases where a person has capacity, they must consent to such treatment. Where a person lacks capacity a substitute decision-maker appointed under the proposed Assisted Decision-Making (Capacity) Bill can also authorise such treatment.
Where a patient does not have capacity and a decision-making representative does not give consent to ECT, such treatment may only take place where it is required as a life-saving treatment, for a patient where there is a threat to the lives of others or where the condition is otherwise treatment resistant. Such ECT may then only be administered subject to approval by a Mental Health Review Board, which must convene within three days of the decision being taken.
Other recommended measures include that:
Renewal orders should be for three or six months only, and that the current 12-month renewal orders should no longer be possible
Children should have a standalone section of the Act with child-appropriate guiding principles
Children aged 16 or 17 should be presumed to have capacity to consent to or refuse admission and treatment
On a phased basis, there should be registration of all community mental health teams and inspection of services now being provided in the community, eg. day hospitals, day centres, and residential services
Revised legislation should proactively encourage and support patients to involve family and carers in the admission process and development of care and treatment plans, including discharge planning.
College of Psychiatrists of Ireland
The College of Psychiatrists of Ireland welcomed the expert group report, noting that the proposals would “advance the rights of those patients with mental illness who are involuntarily detained. It is also welcome that the review recommends changes to protect those who lack capacity but who do not fulfil criteria for involuntary detention”. However, the College, also “saw this as a missed opportunity to improve appropriate access to multifaceted assessment and intervention for the majority of people with mental health problems. Most contacts for mental health problems occur in primary care and in community-based mental health services. Issues such as poor access to counselling and lack of 24/7 access to multidisciplinary assessments and interventions still affect the rights of people with mental distress. The College had hoped the Review would make recommendations in this regard and as regards statutory monitoring of the implementation of A Vision for Change.”
Structural violence and schizophrenia
These legislative developments have clear implications for people with schizophrenia, especially if they experience involuntary admission. While these measures give important protections of the right to liberty, it is important to note that there are many other rights that are relevant in the context of mental disorders such as schizophrenia, and that these other rights are often violated.
In the first instance, despite clear evidence of a substantial biological basis to schizophrenia, there is strong evidence that social, economic and political factors are highly relevant to the clinical features, treatment and outcome of schizophrenia.7 People from lower socioeconomic groups have an earlier age at first presentation with schizophrenia, and longer durations of untreated illness, both of which are associated with poor outcomes.
People with schizophrenia are also over-represented in the homeless population. Intriguingly, migration is associated with increased rates of mental disorder, including schizophrenia. This relationship appears to be mediated by psycho-social factors, including difficulties establishing social capital in smaller migrant groups.
People with schizophrenia are over-represented among prison populations, and imprisonment clearly increases the disability and stigma associated with schizophrenia, and impedes recovery.
The persistent and negative effects of these social, economic and societal factors, combined with the social stigma of mental disorder, constitute a form of ‘structural violence’ which impairs access to psychiatric and social services and greatly amplifies the effects of schizophrenia in the lives of sufferers and their families.
As a direct result of these over-arching social and economic factors, many people with schizophrenia are systematically excluded from full participation in civic and social life. They are constrained to live lives that are shaped by stigma, isolation, homelessness and denial of rights.
The solutions to these complex, multilayered problems must also be complex and multilayered. In the first instance, ongoing development of mental health services is essential, as are ongoing revisions of mental health legislation, as recently proposed in relation to Ireland’s Mental Health Act 2001.
However, the most important task is moving mental health to the very centre of public health and political agendas in Ireland. This is an especially challenging undertaking, but it is a crucial one that underpins all other efforts to address violations and neglect of the rights of the mentally ill.
This is relevant not only in Ireland, but around the world: globally, the WHO reports that most people affected by mental, neurological and substance use disorders, including up to 75% of those in many low-income countries, have no access to treatment of any type.
Schizophrenia and social justice
Several measures are needed in order to achieve social justice for people with schizophrenia and other mental disorders, and their families.
Effective and evidence-based
First, mental health policies need to be effective, evidence-based and free from ideological distortions. Carefully planned outpatient programmes are essential to reduce symptoms, promote recovery and enhance reintegration.
Well-run inpatient facilities, which respect and promote human rights through effective treatment, are another important part of the solution. However, this has been neglected in recent years owing chiefly to ideological objections to inpatient care dating from experiences of previous decades. Certainly, the psychiatric institutions of the past must not be re-created, but new models for sustained care must still be developed, centred on meeting the needs and promoting the dignity of the mentally ill, and their families.
Linked to social policy
Second, mental health policy needs to be linked explicitly with social policy, in recognition of the close association between mental disorder and social exclusion. Housing, welfare benefits and support in employment are all key elements in promoting recovery and need to be delivered hand in hand with more traditional mental health care.
More extensive social engagement
Third, there needs to be social engagement well beyond the arenas of mental health care and social policy. Mental illness is an all-of-society issue requiring all-of-government responses, cutting across traditional departmental and sectoral boundaries. Close cooperation is needed between governmental, non-governmental and civic organisations to create a functioning network of care and support.
Political will
But, most of all, these solutions require political will if they are to be implemented effectively. Mental health care is chronically underfunded and is commonly and shamefully excluded from programmes of societal development, such as the UN’s Millennium Development Goals. This can and must change, especially for people affected by illnesses that can recur over the course of a lifetime, such as schizophrenia.
Change will occur only when the mentally ill, their families, mental health professionals, and all who care about this issue exert sufficient political pressure to drive change. This is by no means impossible: mental health reform formed a key element of President John F Kennedy’s New Frontier. One of the last pieces of legislation he signed in 1963 was the Community Mental Health Act, which was innovative for its era. It is time now for another new frontier on mental health for the globalised world of the 21st century. Reform needs to focus not only on the delivery of effective mental health care to individuals, but also on:
Galvanising social and political constituencies to acknowledge the societal and global challenges presented by mental illness
Develop and sustain programmes of care that promote health and dignity
End the social and political exclusion of people with schizophrenia and other mental illnesses, and their families.
In the words of Rudolf Virchow (1821-1902), German doctor, anthropologist and politician: “Medicine is a social science, and politics nothing but medicine on a large scale”.
Declaration of Interest
There is no conflict of interest. Prof Kelly was a member of the Expert Group on the Review of the Mental Health Act 2001; this article is written in a personal capacity.
References
Daly A, Walsh D. Activities of Irish Psychiatric Units and Hospitals 2013 (HRB Statistics Series 25). Health Research Board, 2014
United Nations. Principles for the Protection of Persons with Mental Illness and the Improvement of Mental Health Care. United Nations Secretariat Centre For Human Rights, 1991.
Division of Mental Health and Prevention of Substance Abuse (World Health Organisation). Mental Health Care Law: Ten Basic Principles. World Health Organisation, 1996.
Ng XT, Kelly BD. Voluntary and involuntary care: Three-year study of demographic and diagnostic admission statistics at an inner-city adult psychiatry unit. International Journal of Law and Psychiatry 2012; 35: 317-26
World Health Organisation. WHO Resource Book on Mental Health, Human Rights and Legislation. World Health Organisation, 2005.
Kelly BD. Mental health legislation and human rights in England, Wales and the Republic of Ireland. International Journal of Law and Psychiatry 2011; 34: 439-54
Kelly BD. Structural violence and schizophrenia. Social Science and Medicine 2005; 61: 721-30
 Figure 1: Key principles of the United Nations’ Principles for the Protection of Persons with Mental Illness and the Improvement of Mental Health Care (1991)2(click to enlarge)
Figure 1: Key principles of the United Nations’ Principles for the Protection of Persons with Mental Illness and the Improvement of Mental Health Care (1991)2(click to enlarge)