W Eugene Smith’s iconic photo-essay ‘Country Doctor’, published in Life Magazine in 1948, chronicled Dr Ernest Ceriani’s daily challenges as a rural GP in Kemmling, Colorado, in an era when the ‘house call’ was an integral part of day-to-day duties. While most doctors extol the virtues of home visits, the literature tells a different story. The pattern of decline in home visit rates is well established worldwide, although considerable variation exists between different healthcare systems and within countries themselves, even where the apparent delivery, regulation and governance of health services are uniform across a nation.1
In 1930s America, home visits comprised 40% of doctor-patient contact; by 1980 this had fallen precipitously to less than 1%.2 More recently, UK home visits have fallen from 22% (of all consultations) in 1971 to 4% in 2003.3
In a similar trend, Australian rates decreased from 158 house calls per 1,000 patients/year to 77 per 1,000/year between 1997 and 2007.4 Based on 1993 Medicare data in the US, Meyer and Gibbons2 reported 27 per 1,000/year, dramatically lower than the comparable UK figures of 299 per 1,000/year (equating to approximately 10% of doctor-patient encounters) and 309 per 1,000/year for those older than 85 years.5
In Campion’s commentary on Meyer and Gibbons’ study, he noted that 8.8 of every 1,000 Americans aged 65 or older received a home visit.6 Startlingly, putting this figure in perspective, he went on to point out that more elderly Americans underwent computerised tomography (18.0 per 1,000) and cardiac catheterisation (15.1 per 1,000) that year than “enjoyed the low-technology luxury of having a physician come to see them at home”.6
How frequent is frequent?
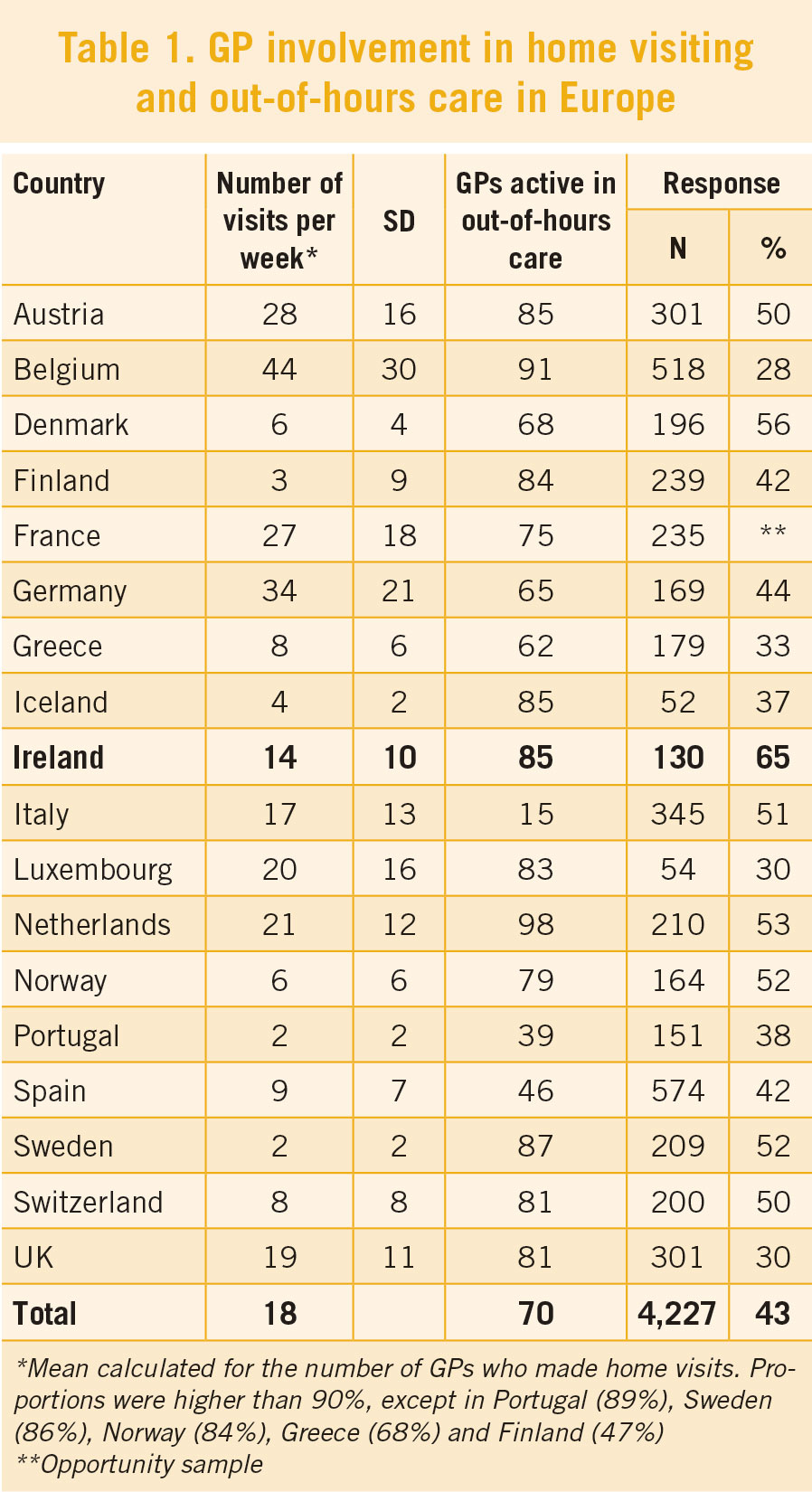
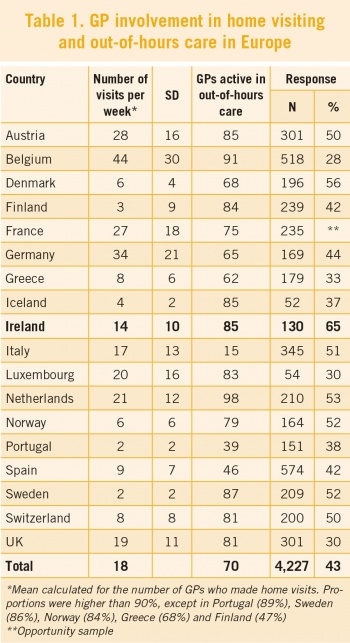
The 2008 American Academy of Family Physicians member survey reported less than one house call per week was made by the average US family physician.7 In contrast, Boerma and Groenewegen,1 examining the issue across 18 European countries, reported an average 18 visits per week (range: 2-44, see Table 1).
(click to enlarge)
How Ireland compares
Stewart and Stewart looked at 12 GP training practices in Donegal over a two-month period and found a mean home visiting rate of 143/1,000/year (range: 45-305/1,000/year).8
Cunney and O’Kelly9 reported a decrease in average home visiting rates of a Dublin inner-city practice with an approximate patient list of 7,000 and slight (57%) private patient predominance, from 45 per month in 2006 to 35 per month in 2010.
Factors associated with the number of home visits performed
GP home visiting practice is largely considered to be influenced by personal preference, practitioner attitudes, demand characteristics and organisational conditions. Yet a number of systematic factors have been illuminated relating to practice type, patient-list composition (eg. age, socio-economic circumstances), health system features and a GP’s role within the health services, and location, in addition to individual GP characteristics such as age and gender.1
Older GPs tend to make more home visits than younger colleagues (independent of size and age characteristics of patient demographic/practice population).1,10 Male GPs make more visits than their female counterparts (even when part-time working is taken into consideration).1,10
Smaller practices make greater numbers of home visits,11 as do solo practitioners, compared to health centres with multiple GPs.12 Rural GPs undertake more home visits than urban equivalents.1,10,11,13,14 Overall number and variation in home visiting among GPs in countries where they have stronger positions/roles within health systems (ie. acting as gatekeepers) are lower.1
Perhaps surprisingly, where GPs are salaried, fewer home visits are performed compared to countries where GPs are mainly self-employed. Boerma and Gronenewegen1 have hypothesised that this is because the self-employed display more ‘entrepreneurial attitudes’ and emphasise ‘customer relations’.
Patient factors demonstrated by O’Sullivan et al15 in their 2004 study of 349,505 patients in England and Wales are broadly consistent with other research4,5,10 and showed increasing age, lower socio-economic status, higher morbidity class, and female gender increased the likelihood of receiving a home visit.
The case for home visits – Why such a decline?
While there is ongoing debate on the necessity and benefits of home visits, it is clear that patients value them. A number of factors have been proffered as to the advantages of home visiting for patients, including convenience – avoidance of waiting rooms, sparing potential discomfort of travel; fostering a closer patient-doctor relationship; and carer reassurance.
“The power and wizardry of modern medicine are impressive, but there is perhaps nothing that patients and families appreciate more than a house call. Almost everyone recognises that in making a house call, the physician is going the extra mile for the patient6.”
From the physicians’ perspective, house calls purportedly provide an opportunity to gain insight into a patient’s personal circumstances – their support structures and autonomy, evaluate home safety, collect collateral histories, and understand carers’ experiences. Theile et al16 interviewed 24 German GPs in relation to home visiting practice. All participants advocated house calls for vulnerable, elderly populations. Although most GPs frequently undertook home visits, many were not convinced of their benefit or felt particularly motivated to do so, some felt obliged to.
Low physician compensation, the time-consuming nature of house calls, lack of facilities (ie. unavailability of equipment, sub-optimal examination environment), disruption to ordinary practice schedule, and loss of revenue have all been documented as probable factors contributing to the decline of the practice.
Historically, from an ‘evolution-of-practice’ perspective, probable contributors to decline such as the introduction of appointment systems to practices, the development of out-of-hours co-operatives, and improvements in telecommunications (itself facilitating ‘telephone triage’) – all contributors to greater levels of efficiency or ‘productivity’ – cannot be overlooked.17 Yet these also speak something of the difficulty of finding satisfactory metrics of what good care provision comprises.
Others point to the wider phenomenon and trend whereby technology increasingly encroaches on our lives in the name of progress, coupled with a heightened litigious predisposition across society at large. Leff and Burton,18 and Kao et al19 have aptly articulated such issues:
“The shift in site of care delivery from the home to clinics and hospitals was the result of an explosion of biomedical knowledge and technology, increased access of patients to a growing medical system, the growth of third-party payers, and heightened liability concerns18.”
“...As more advanced technology was used for diagnosis and treatment of illness, physicians and patients alike came to expect high-technology medicine. With this expectation was the association of ‘good medicine’ with hospitals and clinics. House calls became ‘old fashioned’... “19
What evidence exists of home care effectiveness
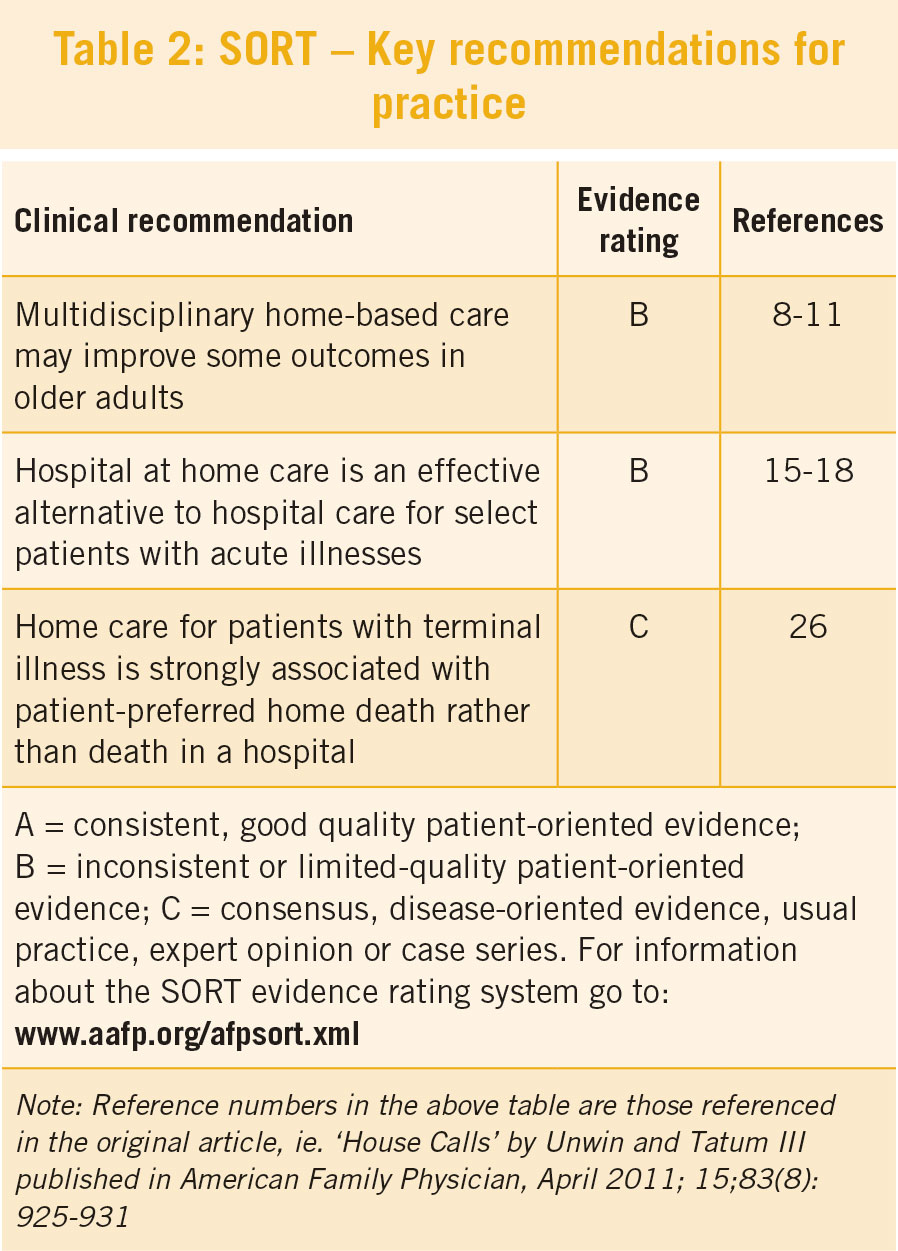
Studies examining effectiveness of home visit programmes for the elderly have reached conflicting conclusions. A summary of the analysis by Unwin and Tatum III7 is presented in Table 2.
(click to enlarge)
Difficulties in comparison and evaluation of the evidence-base relate to issues surrounding: variation in the clinical (‘primary care’ v ‘home care’) team composition, especially inclusion of a doctor; the baseline degree of frailty of participants; and the different outcomes measured.
However, Kao et al in their comprehensive 2009 review of the literature,19 unequivocally endorse home visiting as favourable and testify to the growing body of evidence demonstrating house calls as beneficial to a range of health outcomes including improved physical function, reduced nursing home use and hospitalisation, and even mortality in select cohorts.
The future of house calls – where do we go from here?
The decrease in home visiting rates is undisputed, but how this decline must be evaluated is still up for debate. Is the trend indicative of improved service provision efficiency, with GPs spending decreasing time on less urgent house calls, leaving more time to treat patients in practice settings? Van den Berg et al10 found evidence to suggest that the decline is not necessarily problematic and most likely reflected a sharpening of GPs’ criteria for home visits.
“There seems to be no reason to assume that GPs take unacceptable risks since medical factors are still taken into consideration. In urgent cases, most GPs still visit their patients.”10
However, some concern remains among stakeholders that an essential component of general practice is fast disappearing. Given that the evidence points to older populations as prime recipients of house calls, it’s not unreasonable to expect more pressure on home visits in view of changing demographics.20 Potential solutions for the ongoing provision of effective home visiting practice appear to lie beyond the individual practitioner level. Multidimensional and interdisciplinary home visiting practice may hold promise in managing older patient demographics, their chronic disease burden, and when applicable facilitating smooth patient transition home from acute hospital admissions, rehabilitation, and/or convalescent facilities.
Ironically, medical technology, once seemingly a threat to the very survival of home visits, may revolutionise the capabilities of house calls, eg. portable point-of-care blood testing, outpatient IV infusion, etc. Furthermore, telemedicine/eHealth holds promise for greater efficiencies in doctor-patient interaction and expanded ‘hospital-at-home’ services.
Without exception, discussion on the future of home visits within the literature acknowledges the necessity of sustainable funding solutions (for service providers) underlying continued practice – a salient issue in the Irish context given the January 2011 reduction in General Medical Services (GMS) reimbursement, especially since removal of patient domiciliary distance for capitation payment determination. Cunney and O’Kelly9 have rightly noted that further “discussion, audit, support and appropriate remuneration will be required if all primary care staff are to safely carry out this (home visit) function in an ageing society”.
References
Boerma WGW, Groenewegen PP. GP home visiting in 18 European countries adding the role of health system features. European J Gen Pract 2001; 7: 132-7
Meyer GS, Gibbons RV. House Calls to the Elderly – A Vanishing Practice among Physicians. N Engl J Med. 1997; 337: 1815-1820
Carew N. Are home visits still worthwhile? Forum 2007; 24(9): 28-29
Joyce C, Piterman L. Trends in GP home visits. Aust Fam Physician. 2008; 37(12): 1039-1042
Aylin P, Majeed FA, Cook DG. Home visiting by general practitioners in England and Wales. BMJ 1996; 313: 207-210
Campion EW. Can house calls survive? N Engl J Med 1997; 337: 1840-1841
Unwin BK, Tatum III PE. House Calls. Am Fam Physician. 2011; 83(8): 925-931
Stewart P, Stewart R. Home Visits: Why do rates vary so much? Ir Med J. 2012; 105(3): 83-84
Cunney A, O’Kelly FD. Housecalls in General Practice. Ir Med J. 2012; 105(6): 170-171
Van den Berg MJ, Cardol M, Bongers FJ, de Bakker DH. Changing patterns of home visiting in general practice: an analysis of electronic medical records. BMC Fam Pract. 2006; 7: 58
Calnan M, Butler JR. The economy of time in general practice: an assessment of the influence of list size. Soc Sci Med. 1988; 26: 435-441
Groenewegen PP, Hutten JBF. The influence of supply-related characteristics on general practitioners’ workload. Soc Sci Med. 1995; 40: 349-358
Boerma WGW, Groenewegen PP, van der Zee J. General Practice in urban and rural Europe: the range of curative services. Soc Sci Med 1998; 47: 445-453
Nakar S, Vinker S, Weingarten MA. The place of home visiting in family practice: a multicentre comparison between rural and urban physicians. British Journal of General Practice. 1999; 49: 621-625
O Sullivan C, Omar, R, Forrest C, Majeed, A. Adjusting for case mix and social class in examining variation in home visits between practices. Family Practice. 2004; 21(4): 355-363
Theile G, Kruschinski C, Buck M, Müller CA, Hummers-Pradier E. Home visits - central to primary care, tradition or an obligation? A qualitative study. BMC Fam Pract. 2011; 12:24
Van Royen P, De Lepeleire J, Maes R. Home visits in general practice: an exploration by focus groups. Arch Public Health. 2002; 60: 371-384
Leff B, Burton JR. The Future History of Home Care and Physician House Calls in the United States. J Gerontol A Biol Sci Med Sci. 2001; 56(10): 603-608
Kao H, Conant R, Soriano T, McCormick W. The past, present and future of housecalls. Clinics in Geriatric Medicine. 2009; 25(1): 19-34
World report on ageing and health. World Health Organization 2015 as accessed on: http://www.who.int/ageing/publications/world-report-2015/en/
 (click to enlarge)
(click to enlarge)