Undergraduate paediatric teaching in a regional hospital
A study to evaluate undergraduate paediatric teaching in a regional hospital found that input by clinical teachers in the observation of clinical skills by medical students is vital
Dr Birendra Rai, Paediatric Registrar, Midland Regional Hospital, Mullingar, Prof Farhana Sharif, Consultant Paediatrician; Clinical Associate Professor, Midland Regional Hospital; Royal College of Surgeons, Mullingar, Dublin and Dr Jayne Hopewell, Consultant Paediatrician, Department of Child Health, Blackpool Teaching Hospital, Lancashire, England
Clinical training predominantly occurs in large teaching hospitals, with formal and informal teaching. The recent rise in medical student numbers along with reduced hospital stays by patients, has brought challenges to clinical training in Ireland. There has been a need for increased teaching in the ambulatory care setting, eg. outpatient department and peripheral hospitals. The teaching in this setting can vary from that in tertiary teaching hospitals.1
Clinical teaching is usually given by consultants and NCHDs (non-consultant hospital doctors), with the majority doing so without recognition and formal training, on a voluntary basis, and in addition to full time clinical work which poses significant demands.2 Teaching is often opportunistic, unplanned and didactic.3 Hence, students take on a passive rather than active role, encouraging superficial rather than deep learning.4
Teaching should allow students to develop clinical skills such as professionalism, communication skills, history taking and patient physical examination, all of which are necessary for preparing students for their futures as doctors.5 There are a variety of different methods, ranging from bedside teaching to teaching in the outpatient department. Independent patient contact is an important part of clinical skills learning. Ideally, students should be observed taking a history or performing an examination so that feedback can be given.6 Individual students can have very different learning experiences, especially with regards to the number of different cases and patients seen.7
Paediatric clinical attachments can be difficult for medical students, as children behave differently to adult patients. Therefore, supervision, observation and feedback are vital.8 Performing developmental assessments of children is one of the core learning outcomes, however it is an area that medical students find difficult and in which they lack confidence.9
Recent changes to undergraduate clinical training bring the need to assess what is being done with regards to clinical teaching and the effect of changes made. Previous studies have found regional hospitals to be favourable for student education.1,10 The aim of this study was therefore to evaluate medical students’ opinions on the overall teaching received during their paediatric attachment at the Regional Hospital Mullingar, which is a peripheral hospital. In particular, to gain feedback on the type and quality of teaching received and to identify whether students received adequate practice of patient history taking and clinical examinations, and if these skills were observed. In addition, we aimed to receive feedback on the recently-introduced developmental teaching module.
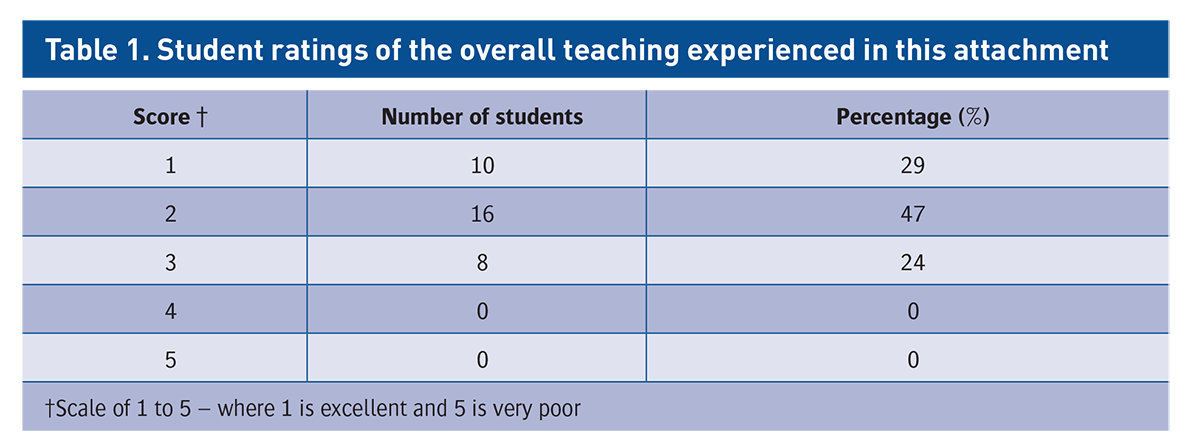
Table 1. Student ratings of the overall teaching experienced in this attachment(click to enlarge)
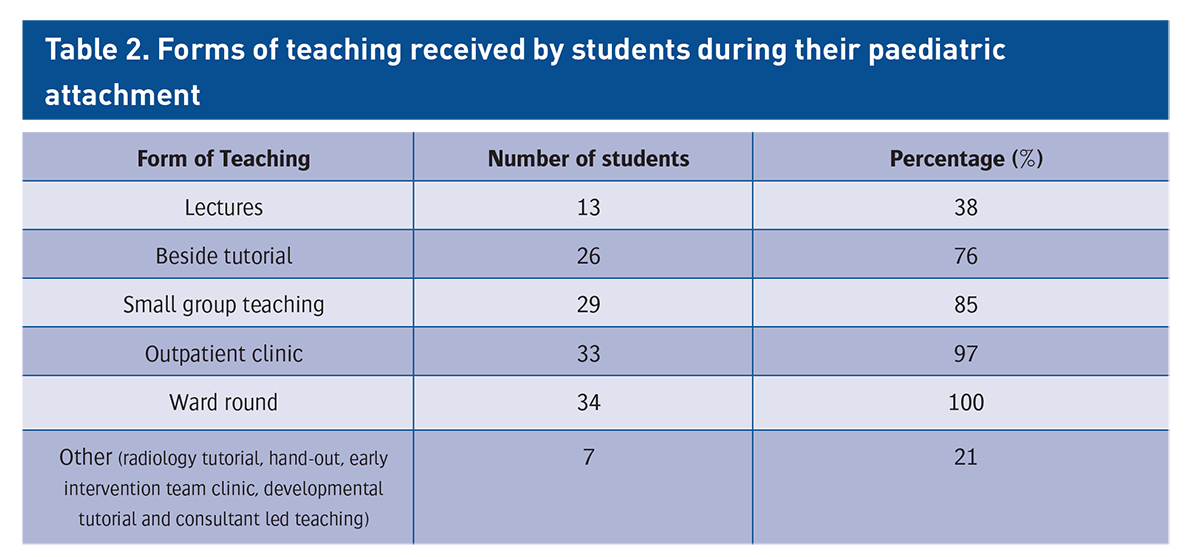
Table 2. Forms of teaching received by students during their paediatric attachment(click to enlarge)
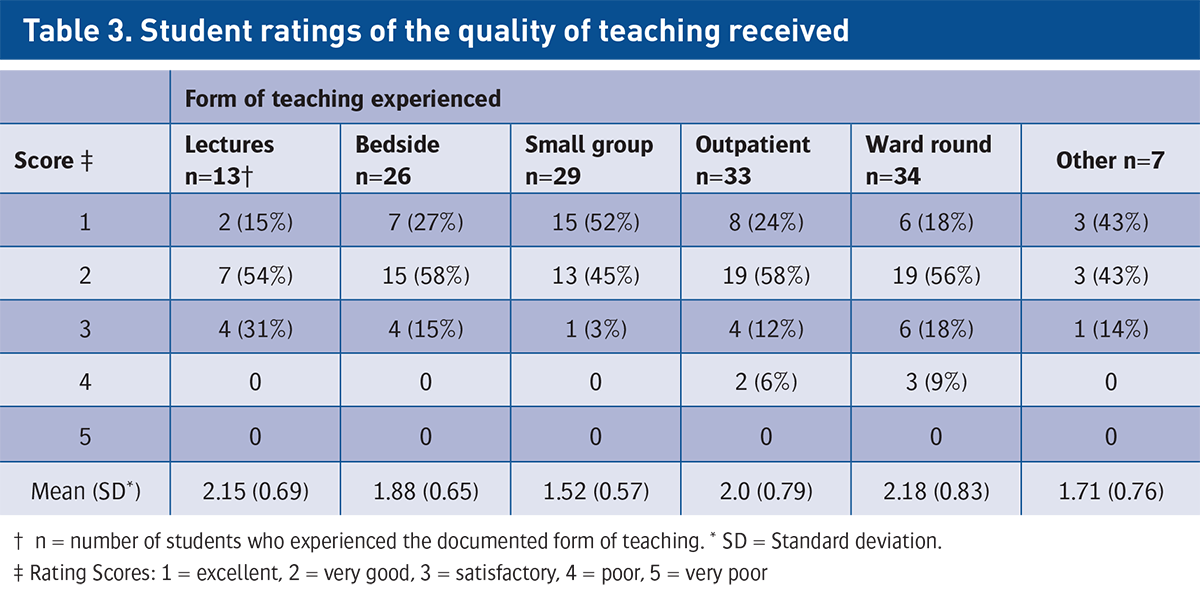
Table 3. Student ratings of the quality of teaching received(click to enlarge)
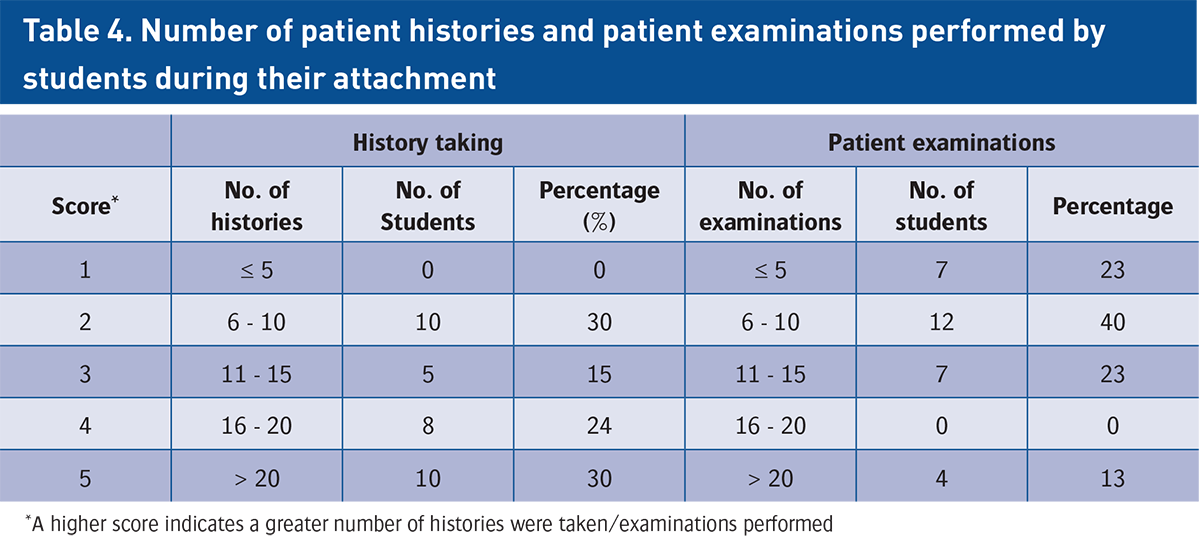
Table 4. Number of patient histories and patient examinations performed by students during their attachment(click to enlarge)
Methods
The study was a prospective questionnaire-based study, conducted at the Regional Hospital Mullingar. All fourth year medical students from the Royal College of Surgeons in Ireland (RCSI) who attended for their two-week paediatric attachment during November 2010 to March 2011 were eligible to take part. There were no exclusion criteria, however students had no obligation to participate.
On average six to seven medical students are present per attachment. These are divided into groups of two or three and each group is then assigned to a consultant. All students receive a log book by the medical school to document clinical activities.
A developmental module for the students was introduced in November 2010 using a variety of styles and methods of teaching. These occurred in addition to regular teaching sessions.
The questionnaire collected both quantitative and qualitative data. Personal details were excluded to ensure anonymity. The questionnaire and an explanatory letter were hand-delivered to each student at the end of their two week attachment by the lead investigator or academic supervisor for immediate completion. The questionnaire was initially piloted by study supervisors and minor adjustments were made prior to distribution. Quantitative data was scored using a four/five point Likert scale and inserted onto an Excel spreadsheet. The qualitative (free text) data was analysed by identifying common themes.
Ethical approval was obtained from both the RCSI Ethics Committee and RCSI Students’ Union prior to carrying out the study.
Results
Thirty-eight students were included. Completed questionnaires were received from 34 student (three absent, one questionnaire not returned) giving a response rate of 89%. Fifteen (44%) of the respondents were male and 19 (56%) were female.
Teaching type and quality
Students were asked on a scale of 1 to 5 (1 being excellent and 5 very poor) to rate the overall teaching experienced during their attachment. All 34 students responded (see Table 1). The mean score was 1.94. No score >3 was given and 26/34 (76%) gave a rating of excellent or very good. The forms of teaching received are shown in Table 2.
Student ratings of the quality of teaching received during the attachment were positive (see Table 3). Small group and bedside teaching were perceived to be the best quality. Teaching on ward rounds and in the outpatient setting were the only forms considered by some to be poor quality. Students also rated the child development teaching on a score of 1 to 5. Thirty-three students responded. The mean score was 2.03. More students felt confident or very confident in taking a developmental history following the developmental teaching than performing a developmental examination – 73% versus 58% respectively.
History and examination skills
The number of histories and examinations taken are shown in Table 4. Thirty-three students (97%) felt they had gained adequate practice of patient history taking and 26/32 respondents (81%) felt they had gained adequate clinical examination skills.
The total number of histories taken by individual students ranged from six to >30. The student reporting inadequate practice had taken six histories. The number of clinical examinations performed ranged from two to 30. Eight students documented inadequate practice of clinical examinations. Two students did not state the number performed, the remaining six performed four to 10 examinations.
Only 14 (41%) students were observed taking a patient history by a physician. All students had the opportunity to present at least one history. Eighteen students (53%) stated they were observed performing a patient clinical examination. The number of times observed was variable, ranging from one to 20 for history taking and one to 18 for clinical examination.
Of the 34 students, 30 (88%) made suggestions on how the paediatric attachment could be improved. Four recurring themes were identified; to see patients independently in the outpatient department, increased number of teaching sessions, more time for self directed learning and increased observation/teaching of examination skills. The need for more teaching sessions, especially bedside teaching, was suggested by 67% (20/30) of respondents.
Comments made by students regarding the positive attributes of the attachment were encouraging. At least one comment was made by 33 students (97%). The teaching and friendly/approachable staff were the predominant themes. A third of students reported good patient exposure.
Twenty-six (77%) students recommended a variety of areas that would benefit from additional teaching, in particular neurological, developmental and cardiovascular system examinations. Other suggestions included more examination teaching at the bedside and to be observed taking histories and performing examinations.
Discussion
The response rate was good at 89%. Medical students received clinical teaching in a variety of different forms. As found in the study by Young et al in 2009, most of the different learning opportunities were highly valued by students.11 Small group teaching received the highest rating.
Previous studies reported a decline in bedside teaching.12,13 Ramani 2003 documented that <25% of clinical teaching time is spent at the bedside.14 In our study 76% (26/34) had received bedside teaching. The ratings for the quality of bedside teaching was encouraging, with 76% stating that the teaching was excellent/very good. Students were keen to have more bedside teaching sessions. This complements the findings of Nair et al (1997) and Williams et al (2008), where 48% and 41-65% respectively felt that they had not received sufficient bedside teaching.15,16
Stark found that students had variable experiences of the quality of teaching in the outpatient clinic setting.17 This was reflected in this study with some students rating the teaching as excellent but others (6% of respondents) rating it as poor. Students suggested the need to see patients on their own, however room availability is difficult. Hence, students possibly have an observer role, encouraging passive learning.3
The frequency of ward rounds for academic purposes is said to be decreasing,18 however in this study all students experienced ward rounds teaching. Walton et al described ward rounds as one of the most important clinical training activities and the foundation of clinical education.18 Ward rounds in this study however received the lowest rating with regards to teaching quality. This agreed with Sanson-Fisher et al where students believed ward rounds to have low instructional value and opportunistic teaching.7 The low ratings for ward rounds and clinics could be due to the busy nature of these activities, leaving little time for teaching.
Results from the questionnaire showed that 97% (33/34) had gained adequate practice of patient history taking. The number of histories taken varied (range six to >30). Interestingly, the student who felt they had received inadequate practice took the least amount of histories. Unfortunately, the reason for lack of practice was not included in the questionnaire. Adequate practice of patient examinations was reported by 81% (26/32) respondents.
The observation of students’ history taking and patient examinations was poor. Only 14 (41%) were observed while taking a patient’s history and 53% while performing a clinical examination. A similar percentage was found in a survey by Kumar (2004) where only 57% of paediatric clerkships evaluated students’ physical examination skill and clinical skills by observation.19 These results are disappointing, especially when observation has been shown to be an important way of assessing a students’ clinical development.6 All students in this study had the opportunity to present a patient history. Allowing students to present a case has been reported to be an important characteristic of clinical teachers.20
A child development module was recently introduced and 70% (23/33) of respondents perceived this teaching to be excellent or very good. Almost all, 97% (32/33), respondents felt that they would have some confidence in taking a developmental history. However, students felt less confident with performing a developmental examination (88%). This agrees with findings in an Australian study where only 45% of students felt confident in performing a developmental assessment.9
Many studies have compared teaching and learning in the peripheral/DGH (District General Hospital) setting versus the teaching hospital setting.1,10 Staff in DGHs were friendlier and showed more interest in students.1,10 In our study the most frequent comment in the free text was the friendliness/approachability of the staff. Johnston and Boohan found that teaching in the DGH setting was more educational and enjoyable.1 Some 45% (15/33) of respondents in our study documented the teaching to be a positive attribute. Peripheral hospitals generally have fewer students per consultant team and this is reflected in this study with two to three students per consultant. This study supports previous findings that smaller sites are perceived as favourable with regards to learning, teaching and a positive atmosphere.21
There are limitations. Firstly, the sample size was small however it did represent 89% of students attending during the study period. Four students did not participate and may have biased results as the reason for the these students’ absence is unknown, eg. did the students fail to attend because they felt the teaching was not beneficial. The study was also carried out in a single institution.
Conclusion
Despite its limitations, the findings corresponded well with previous studies. Similarities regarding the highly rated clinical teaching sessions, the need for more bedside and developmental assessment teaching, along with more observation of clinical skills were shown. The advantages of learning in a peripheral hospital were also highlighted in this study. Further studies with larger samples are needed to consolidate the positive attributes of peripheral healthcare teaching to medical students as well as to find out the drawbacks as it may lead to further changes in teaching modules and practices for better future prospects. We hope our study will attract researchers’ attention for further studies into this field.
Declaration of interest
The authors declare that they have no competing interests. We did not receive any funding from any agency or person for this study
Acknowledgements
We extend our sincere thanks to the medical students who participated in this study
References
Johnston BT, Boohan M. Basic clinical skills: Don’t leave teaching to the teaching hospitals. Medical Education 2000; 34(9):692-699
Hendry RG, Kawai GK, Moody WE et al. Consultant attitudes to undertaking undergraduate teaching duties: Perspectives from hospitals serving a large medical school. Medical Education 2005; 39(11):1129-39
Spencer J. Learning and teaching in the clinical environment. BMJ (Clinical Research Ed.) 2003; 326(7389):591-594
Marton F, Saljo R. On qualitative differences in learning. I. Outcomes and process. Br J Educational Psychology 1976; 46:4-11
Bannister SL, Raszka WV Jr, Maloney CG. What makes a great clinical teacher in pediatrics? lessons learned from the literature. Pediatrics 2010; 125(5), 863-865
Brownell AK, McDougall GM. The patient as the focus of teaching. Can Med Assoc J 1984; 131(8):855-857
Sanson-Fisher RW, Rolfe IE, Jones P, Ringland C, Agrez M. Trialling a new way to learn clinical skills: Systematic clinical appraisal and learning. Medical Education 2002; 36(11):1028-1034
Crowther RL. A medical student’s view of paediatrics. J Royal Society of Medicine 1990; 83(11):683-685
Nicol P. Using the ages and stages questionnaire to teach medical students developmental assessment: A descriptive analysis. BMC Medical Education 2006; 6:29
Parry J, Mathers J, Al-Fares A et al. Hostile teaching hospitals and friendly district general hospitals: Final year students’ views on clinical attachment locations. Medical Education 2002; 36(12):1131-1141
Young L, Orlandi A, Galichet B, Heussler H. Effective teaching and learning on the wards: Easier said than done? Medical Education 2009; 43(8):808-817
El-Bagir M, Ahmed MK. What is happening to bedside clinical teaching? Medical Education 2002; 36:1185-1188
Anderson RC, Fagan MJ, Sebastian J. Teaching students the art and science of physical diagnosis. Am J Med 2001; 110:419-423
Ramani S. Twelve tips to improve bedside teaching. Medical Teacher 2003; 25(2):112-115
Nair BR, Coughlan JL, Hensley MJ. Student and patient perspectives on bedside teaching. Medical Education 1997; 31(5):341-346
Williams KN, Ramani S, Fraser B, Orlander JD. Improving bedside teaching: Findings from a focus group study of learners. Academic Medicine. J Assoc American Medical Colleges 2008; 83(3):257-264
Stark P. Teaching and learning in the clinical setting: A qualitative study of the perceptions of students and teachers. Medical Education 2003; 37(11): 975-982
Walton JM, Steinert Y. Patterns of interaction during rounds: Implications for work-based learning. Medical Education 2010; 44(6): 550-558
Kumar K, Gera R, Shah G, Godambe S, Kallen DJ. Student evaluation practices in paediatric clerkships: a survey of the medical schools in the United States and Canada. Clinical Paediatrics 2004; 43(8):729-735
Alweshahi Y, Cook D. Domains of effective teaching process students perspectives in two medical schools. Medical Teacher 2009; 31(4): e125-30
Bennett D, Kelly M, O’Flynn S. Are the bigger hospitals better: DREEM on? Ir J Medical Science 2010; 179(4): 515-519
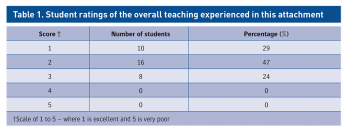 Table 1. Student ratings of the overall teaching experienced in this attachment(click to enlarge)
Table 1. Student ratings of the overall teaching experienced in this attachment(click to enlarge)