The exciting area of immunotherapeutics continues to advance clinical outcomes for cancer patients
Dr Derek Power, Consultant in Medical Oncology, Cork University Hospital, Cork, Dr Lynda McSorley, SpR in Medical Oncology, Galway University Hospital, Galway and Dr Deirdre Kelly, Specialist Registrar in Medical Oncology, Department of Medical Oncology, Cork University Hospital, Cork
Huge optimism has been stirred in the medical oncology community in recent years with breakthroughs in immunotherapy leading to durable disease response across certain cancer types. Continuing to refine treatment combinations and identify effective biomarkers to enhance clinical efficacy in this area remain a priority.
An effective cytotoxic immune response against a cancer cell requires a complex interaction between the adaptive and innate immune system. The human immune system is an intricate and sophisticated system that is not completely understood. CD8+ and CD4+ lymphocytes initiate the distinction between self and non-self antigens. Tumours evade immune surveillance through multiple mechanisms including:
Loss or alteration of antigenic machinery1,2
Promotion of an immune-tolerant micro-environment by manipulation of cytokines
Up-regulation of immune checkpoint molecules such as PD-1 and PD ligand 1 (PD-L1) that promote peripheral T-cell exhaustion.3
Ongoing study is directed at using the immune system as a therapeutic modality to control and treat malignancies. Research approaches include investigation of cytokines, T-cells, antigen-presenting cells, oncolytic viruses and vaccines.
For the purpose of this article we concentrate on clinical advances in checkpoint inhibition, primarily cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitors and programmed cell death 1 (PD-1) inhibitors. We explore toxicities of treatment and present some of the recent clinical trial data pertaining to these agents.
Immune checkpoint inhibitors
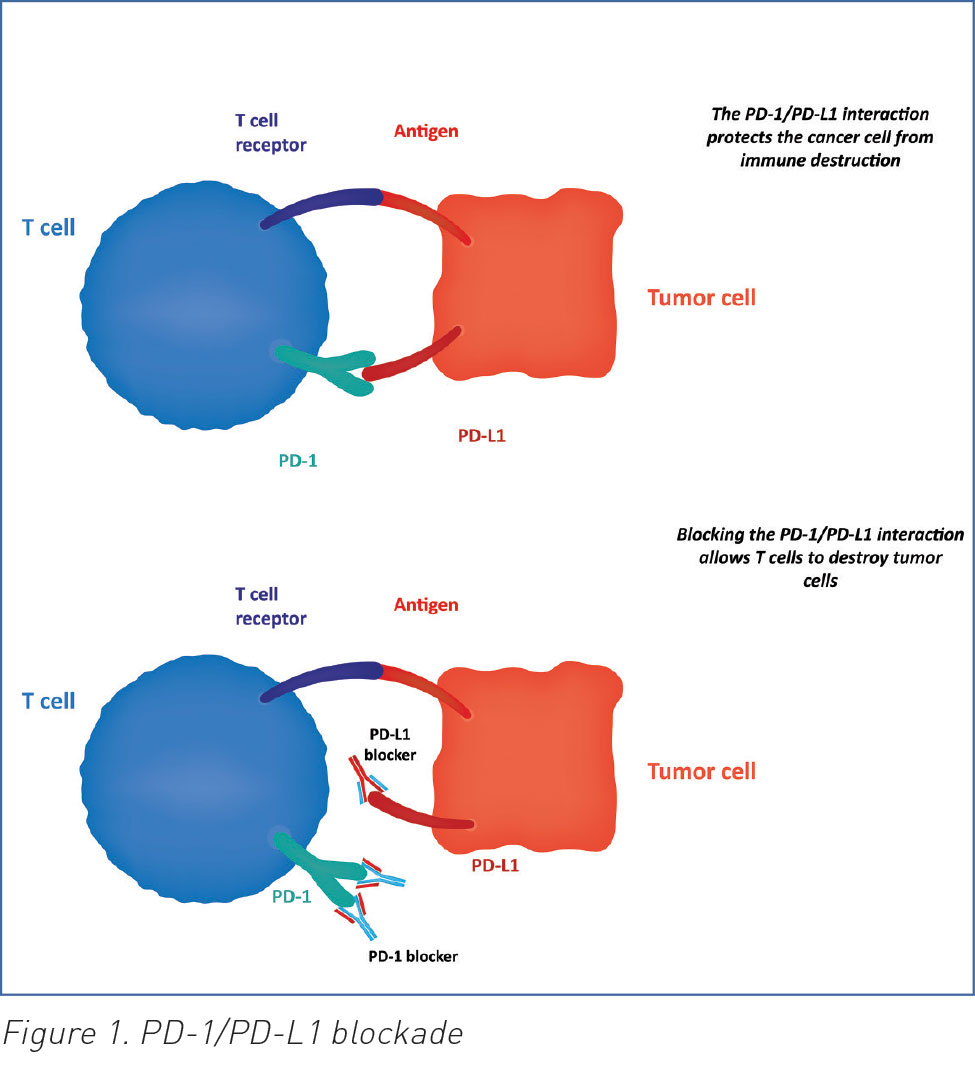
CTLA-4 was discovered in 1987. It is stimulated by antigen presenting cells (APCs) and acts to prevent CD4+ and CD8+ T-cell activation.4 Ipilimumab was the first anti-CTLA-4 antibody immune checkpoint inhibitor to be approved based on its ability to prolong survival in patients with metastatic melanoma.5 PD-1 is a transmembrane protein expressed on T-cells, B-cells and natural killer (NK) cells. Binding of PD-1 to its ligand PDL-1 inhibits apoptosis of the tumour cell and promotes peripheral T-effector cell exhaustion (seeFigure 1).6,7 Nivolumab and pembrolizumab are PD-1 antibodies that inhibit tumour cell evasion of the immune system. They are approved for use in patients with advanced melanoma and non-small cell lung cancer as they have demonstrated an overall survival benefit.
Currently several clinical trials are investigating immunotherapy combinations. Concurrent CTLA-4 and PD-1 blockade with ipilimumab plus nivolumab has demonstrated increased overall response rates but this has been associated with increased toxicity; 55% of patients on a pivotal phase III trial in melanoma experienced grade 3-4 adverse events such as diarrhoea, deranged liver function tests and colitis.8
(click to enlarge)
Toxicities
Immune-related adverse events (irAEs) occur due to generalised stimulation and enhancement of the immune system.9,10 The most frequently seen irAEs involve skin (rash), GI tract (diarrhoea/colitis), liver (elevations of AST and ALT) and endocrine (hypophysitis, hypothyroidism, hyperthyroidism, thyroiditis or adrenal insufficiency).9 Pneumonitis can also occur. The incidence of pneumonitis appears to be less than 10% in patients receiving anti-PD-1/PD-L1 therapy and is more common in patients with lung cancer.11,12,13,14
Rapid identification and early intervention is critical to the successful management of toxicities. Combination immunotherapy is associated with a significantly increased risk of irAEs. For patients experiencing moderate (grade 2) irAEs, management requires withholding the offending immunotherapy agent. Systemic corticosteroids should be commenced if symptoms do not resolve within a week (prednisone 0.5mg/kg/day).15
For life-threatening irAEs (≥ grade 3), management involves permanent discontinuation of the immunotherapy agent and early addition of high doses of corticosteroids (prednisone 1-2mg/kg/day or equivalent), followed by a slow steroid taper over at least one month.
Mortality in immune-related colitis had been associated with delayed reporting, non-compliance with an antidiarrhoeal regimen, and lack of drug withholding.15 Infectious causes must first be ruled out in someone presenting with severe diarrhoea. Once ruled out, corticosteroids should be commenced early, and if not controlling the colitis, consideration should be given to infliximab (5mg/kg) treatment to suppress the unregulated immune system.17,18,19
Immunotherapeutic advances: ASCO 2016
“Every year, thousands of oncologists and millions of patients all over the world await the news coming from this meeting – new breakthroughs, new therapies, new promises of cure, hope. ASCO is harnessing the collective wisdom of oncologists around the world to put patients at the centre of research and care,” stated then US vice president Joe Biden, at ASCO 2016.
The annual ASCO meeting, with over 5,000 research submissions and more than 36,000 attendees, concentrates the most recent advances in global cancer research. Immunotherapy continues to be investigated and developed across many cancer subtypes. In fact, ASCO identified immunotherapy as the advancement of the year in its Clinical Cancer Advances 2016 report.
Colorectal cancer
At the annual meeting in Chicago this year, a phase II study looking at PD-1 blockade in mismatch repair (MMR)-deficient cancers reported on 55 patients with metastatic or locally-advanced MMR-deficient colorectal cancer.20 They had received at least two prior lines of systemic therapy prior to proceeding to pembrolizumab 10mg/kg given two weekly. The overall response rate (ORR) in MMR-deficient colorectal cancer was 57% versus 0% in MMR-proficient colorectal cancer. The investigators also found that mutational load was a good predictor of response to PD-1 blockade.20 This study is potentially practice-changing as it shows that MMR-deficient colorectal cancers have high and durable responses to anti PD-1 therapy.
Non-small cell lung cancer
Unprecedented response rates were seen in first-line advanced non-small cell lung cancer (NSCLC) with the combination nivolumab (3mg/kg given two weekly) and low-dose ipilimumab (1mg/kg given six-12 weekly) achieving an ORR of 39-47%.21
Head and neck cancer
Particularly exciting work has revealed new standards for recurrent and metastatic head and neck cancer. The Checkmate 141 phase III clinical trial enrolled more than 300 patients with recurrent refractory metastatic head and neck squamous cell carcinoma (HNSCC) who had received previous platinum therapy. They were randomised 2:1 to nivolumab versus investigator’s choice of second-line chemotherapy. The one year OS in the nivolumab arm was 36% versus 16% in the chemotherapy arm (p = 0.01).22 This represents a new treatment paradigm for this patient cohort.
The Keynote 055 Study was a single-arm phase 2 trial of recurrent HNSCC refractory to platinum and cetuximab. Patients received pembrolizumab 200mg three weekly. The ORR was 18%.23 This represents a new standard of care in platinum refractory patients and approval by the FDA and EMA is pending.
Bladder cancer
Advanced urothelial cancer has been challenging to treat, however two studies of atezolizumab (an anti-PDL-1 monoclonal antibody) have provided long-awaited positive data. In patients who were unsuitable for first-line cisplatin, atezolizumab first-line treatment produced a 12-month OS of 57%.24 A separate phase II single arm trial evaluated atezolizumab in patients who had received previous platinum therapy. In this setting, atezolizumab elicited a 12-month OS of 35%. It was well tolerated and compared favourably to alternative therapies in this space. This has led to the FDA accelerating approval of atezolizumab in post-platinum bladder cancer patients.25
Metastatic melanoma
Updated results from Checkmate 067 data were also presented at ASCO 2016. This was a double-blind phase III trial of more than 900 patients with unresectable metastatic melanoma randomised to nivolumab and ipilimumab combination versus nivolumab or ipilimumab alone. Objective response rates (ORR) were 57.6% for the combination, 43.7% for nivolumab monotherapy and 19% for ipilimumab monotherapy. PFS at 12 and 18 months is similar between combination treatment and nivolumab monotherapy. It appears there may not be a substantial advantage in adding ipilimumab to nivolumab in terms of improving the rates of complete responses.
Of note, the combination therapy is associated with increased incidence (55%) of grade 3-4 adverse events, which appear to also have increased likelihood of involving multiple organs.8 Managing immune-related toxicity can be challenging and requires knowledge of the effects of immune stimulation across many organ systems, eg. gastrointestinal, endocrine, hepatic, renal and dermatologic. In addition, there is a significant cost implication for the combination treatment and society as a whole is struggling with this.
A phase II survival analysis in patients with advanced melanoma who discontinued treatment with nivolumab plus ipilimumab due to toxicity showed similar one year OS rates between patients who discontinued versus those who continued therapy.26 Patients who experience immune-related adverse events may not need to continue treatment as, if they are going to benefit, they will get the clinical response whether the drug is restarted or not and there is little value in re-exposing patients to potential further toxicity.
At this time, the 12-month OS for patients with advanced melanoma who receive combination immunotherapy is identical to that of nivolumab monotherapy.27 However, as follow-up continues, this may change. The standard of care now remains both anti PD-1 monotherapy or combination immunotherapy. The sequencing with targeted BRAF MEK inhibition is as yet unclear in those patients with somatic BRAF mutations; clinical trials are ongoing.
Conclusion
The exciting area of immunotherapeutics continues to advance clinical outcomes for cancer patients. Clinical trials are ongoing in adoptive therapies – activated T-cells and autologous tumour infiltrating lymphocytes (TILS). Randomised controlled trials are investigating the use of these agents in multiple cancer types and, as these agents become safer to deliver, it looks promising that we will be able to harness the unique power of an individual’s own immune system to continue to improve cancer care for patients.
References
Johnsen AK, Templeton DJ, Sy M, Harding CV. Deficiency of transporter for antigen presentation (TAP) in tumor cells allows evasion of immune surveillance and increases tumorigenesis. J Immunol 1999; 163: 4,224
Donia M, Andersen R, Kjeldsen JW et al. Aberrant Expression of MHC Class II in Melanoma Attracts Inflammatory Tumor-Specific CD4+ T- Cells, Which Dampen CD8+ T-cell Antitumor Reactivity. Cancer Res 2015; 75:3,747
Walker LS, Sansom DM. The emerging role of CTLA4 as a cell-extrinsic regulator of T cell responses. Nat Rev Immunol 2011; 11: 852
Schadendorf D, Hodi FS, Robert C et al. Pooled Analysis of Long-Term Survival Data From Phase II and Phase III Trials of Ipilimumab in Unresectable or Metastatic Melanoma. J Clin Oncol 2015; 33: 1,889
Francisco LM, Salinas VH, Brown KE et al. PD-L1 regulates the development, maintenance, and function of induced regulatory T cells. J Exp Med 2009; 206: 3,015
Amarnath S, Mangus CW, Wang JC et al. The PDL1-PD1 axis converts human TH1 cells into regulatory T cells. Sci Transl Med 2011; 3: 111ra120
Wolchok JD et al. Efficacy and safety results from a phase III trial of nivolumab (NIVO) alone or combined with ipilimumab (IPI) versus IPI alone in treatment-naive patients (pts) with advanced melanoma (MEL) (CheckMate 067). J Clin Oncol 33, 2015 (suppl; abstr LBA1)
Naidoo J, Page DB, Li BT et al. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann Oncol 2015; 26: 2,375
Champiat S, Lambotte O, Barreau E et al. Management of immune checkpoint blockade dysimmune toxicities: a collaborative position paper. Ann Oncol 2016; 27: 559
Brahmer J, Reckamp KL, Baas P et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med 2015; 373: 123-135
Garon EB, Rizvi NA, Hui R et al. Pembrolizumab for the treatment of non-small cell lung cancer. N Engl J Med 2015; 372: 2,018-2,028
Robert C, Thomas L, Bondarenko I et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med 2011; 364:2,517-2,526
Kleiner DE, Berman D. Pathologic changes in ipilimumab-related hepatitis in patients with metastatic melanoma. Dig Dis Sci 2012; 57: 2,233-2,240
Weber JS, Dummer R, de Pril V et al. Patterns of onset and resolution of immune-related adverse events of special interest with ipilimumab: detailed safety analysis from a phase 3 trial in patients with advanced melanoma. Cancer 2013; 119:1,675-1,682
Joseph RW, Cappel M, Goedjen B et al. Lichenoid dermatitis in three patients with metastatic melanoma treated with anti-PD-1 therapy. Cancer Immunol Res 2015; 3: 18-22
Carlos G, Anforth R, Chou S et al. A case of bullous pemphigoid in a patient with metastatic melanoma treated with pembrolizumab. Melanoma Res 2015; 25: 265-268
Krenacs T, Kiszner G, Stelkovics E et al. Collagen XVII is expressed in malignant but not in benign melanocytic tumors and it can mediate antibody induced melanoma apoptosis. Histochem Cell Biol 2012; 138: 653-667
Dung T Le et al. PD-1 blockade in mismatch repair deficient non-colorectal gastrointestinal cancers. J Clin Oncol 34, 2016 (suppl 4S; abstr 195)
Hellman MD et al. CheckMate 012: Safety and efficacy of first-line (1L) nivolumab (nivo; N) and ipilimumab (ipi; I) in advanced (adv) NSCLC. J Clin Oncol 34, 2016 (suppl; abstr 3001)
Ferris R et al. Further evaluations of nivolumab (nivo) versus investigator’s choice (IC) chemotherapy for recurrent or metastatic (R/M) squamous cell carcinoma of the head and neck (SCCHN): CheckMate 141. J Clin Oncol 34, 2016 (suppl; abstr 6009)
Bauml J et al. Preliminary results from KEYNOTE-055: Pembrolizumab after platinum and cetuximab failure in head and neck squamous cell carcinoma (HNSCC). J Clin Oncol 33, 2015 (suppl; abstr 6011)
Balar AJ et al. Atezolizumab (atezo) as first-line (1L) therapy in cisplatin-ineligible locally advanced/metastatic urothelial carcinoma (mUC): Primary analysis of IMvigor210 cohort 1. J Clin Oncol 34, 2016 (suppl; abstr LBA4500
Hoffman-Censits JH et al. IMvigor 210, a phase II trial of atezolizumab (MPDL3280A) in platinum-treated locally advanced or metastatic urothelial carcinoma (mUC). J Clin Oncol 34, 2016 (suppl 2S; abstr 355)
Hodi FS et al. Overall survival in patients with advanced melanoma (MEL) who discontinued treatment with nivolumab (NIVO) plus ipilimumab (IPI) due to toxicity in a phase II trial (CheckMate 069). J Clin Oncol 34, 2016 (suppl; abstr 9518)
Weber JS et al. Survival outcomes of nivolumab (NIVO) given sequentially with ipilimumab (IPI) in patients with advanced melanoma (CheckMate 064). J Clin Oncol 34, 2016 (suppl; abstr 9517)
 (click to enlarge)
(click to enlarge)