CARDIOLOGY AND VASCULAR
Who will benefit from CVD prevention?
The new European CVD prevention guidelines place a greater emphasis than before on specific clinical conditions with a higher risk
September 26, 2016
-
The latest European guidelines on cardiovascular disease (CVD) prevention in clinical practice were recently launched at the EuroPrevent conference in June 2016.1 These guidelines represent an evidence-based consensus of the Sixth European Joint Task Force, involving 10 professional societies.
As guidelines with a solid evidence base are more likely to be implemented in practice, the Task Force continues to use the ESC grading system based on classes of recommendations and levels of evidence. The guidelines continue to promote a lifetime approach to CV risk, recognising that risk is continuous as the person ages and/or develops comorbidities.
While the new guidelines clearly identify the individuals who fall into the various risk categories, they also place a greater emphasis on specific clinical conditions that may be associated with a higher than calculated risk, such as autoimmune disease, female specific conditions, erectile dysfunction, etc.
Patients treated for cancer
The new 2016 guidelines place a much stronger emphasis on CV risk in patients surviving cancer in comparison to previous guidelines.
While the risk factors for both cancer and CVD are similar and strongly relate to poor diet, smoking, alcohol misuse and physical inactivity, there is also significant evidence to suggest that treated cancer survivors have an increased CVD risk.
The scientific evidence suggests that the increased incidence of CVD is correlated with the treatments (chemotherapy and/or radiotherapy) given and their administered dose.
Cardiotoxicity due to chemotherapy is related to a direct effect on the cell through the generation of reactive oxygen species. Some chemotherapy agents can have a direct ischaemic effect and can increase risk factors such as hypertension and accelerate atherosclerosis, especially in older patients.2
Cardiotoxicity due to chest radiotherapy can also accelerate atherosclerosis; however this may occur many years after treatment exposure. Moreover, the presence of traditional risk factors in cancer patients further increases their risk.1
Recommendations for practice
The new ESC guidelines recommend:
• Conducting a careful baseline assessment of CV risk factors to identify those at higher risk for cardiotoxicity
• Greater attention should be given to lifestyle factors in cancer survivors including healthy diet, smoking cessation and weight management
• In line with a recent Cochrane systematic review, aerobic exercise should be strongly advised as it has been shown to be effective for the prevention and/or treatment of chemotherapy-induced cardiac damage3
• Signs and symptoms of cardiac dysfunction should be monitored before and periodically during treatment, thus pre-treatment evaluation of left ventricular function is required
• The need for ongoing collaboration between primary care, oncology and cardiology to deliver optimal survivorship care.
With cancer being the second major cause of death in Ireland following cardiovascular disease and with the number of newly diagnosed cancers growing by 6-7% annually,4 it would appear that there is an urgent need to define what is the most appropriate strategy to improve risk stratification and prevent CVD in patients treated for cancer.1
Autoimmune disease
There is established evidence which demonstrates high-grade inflammations as a pathway for accelerated vascular disease. The guidelines highlight that rheumatoid arthritis (RA) enhances CV risk independent of traditional risk factors and recommend that the use of a 1.5-factor risk multiplier should be considered in assessing CV risk.
While there is increasing evidence that other immune diseases such as ankylosing spondylitis or early severe psoriasis increase CV risk, this evidence is not as strong as that for RA and therefore clinical judgement should be applied when assessing CV risk.
The guidelines also highlight that there is a lack of evidence around drug interactions between anti-inflammatory and immunosuppressive drugs with statins, antihypertensive agents and antiplatelet agents.1
Obstructive sleep apnoea
There has not been much change between the 2012 and 2016 guidelines regarding sleep apnoea.5,1 There is evidence of a positive relationship between obstructive sleep apnoea (OSA) and hypertension, coronary artery disease, atrial fibrillation, stroke and heart failure.
OSA affects an estimated 9% of adult women and 24% of adult men and has been associated with a relative risk of 1.7 for morbidity and mortality. While there are mechanisms for screening through the Berlin Questionnaire and Epworth Sleepiness Scale, more studies are needed to determine whether routine screening reduces (non) fatal CVD.
However it is evident that for those diagnosed with OSA, continuous positive airway pressure is the gold-standard therapy and reduces CV mortality and events.
Influenza
Influenza epidemics are associated with an increased risk of cardiovascular events. The recent guidelines recommend that the ‘influenza vaccine may be considered for patients with established CVD’.
However, this is in contrast to previous 2012 guidelines where it was ‘recommended for all patients with established CVD’.
This downgrade of the recommendations is based on the outcomes of a recent meta-analysis which suggests that while preventing influenza by vaccination can prevent influenza-triggered AMI, there is a concern that some studies may be biased, thus more research is warranted.6
Periodontitis
There are studies which show the link between periodontal disease and atherosclerosis.7,8 However the guidelines continue to highlight the lack of clear evidence regarding the impact of active treatment or prevention of periodontitis in terms of reduced CV risk and clinical prognosis.1
Erectile dysfunction
The risk factors for both erectile dysfunction (ED) and CVD are similar and include age, hypertension, high cholesterol, insulin resistance and diabetes mellitus, smoking, physical inactivity, obesity and depression. Erectile dysfunction and CVD also share a common pathophysiological basis of aetiology and progression.9
There are numerous studies that show that ED is associated with future CV events in men with and without established CVD. According to the guidelines, ED precedes coronary artery disease, stroke and periphereal arterial disease by a period that ranges from two to five years of age.
A recent meta analysis showed that patients with ED have a 44% higher risk for total CV events, 62% for MI, 39% for stroke and 25% for all-cause mortality.10 However, despite this the benefits of routine screening for ED and the most effective tool to assess it are still unclear. The guidelines recommend that assessment of CV risk factors and CVD signs or symptoms in men with ED should be considered.1
Female-specific conditions
While the guidelines refer to women being at lower CV risk than men, they continue to emphasise that their risk is deferred by 10 years rather than avoided.
Women also continue to be underrepresented in clinical trials, a gap which requires urgent review considering that more women in Ireland and worldwide die from disease of the circulatory system that any other cause.1,11
However, of significance, the guidelines for the first time focus on female-specific conditions that increase CVD risk, dividing them into obstetric and non-obstetric conditions.
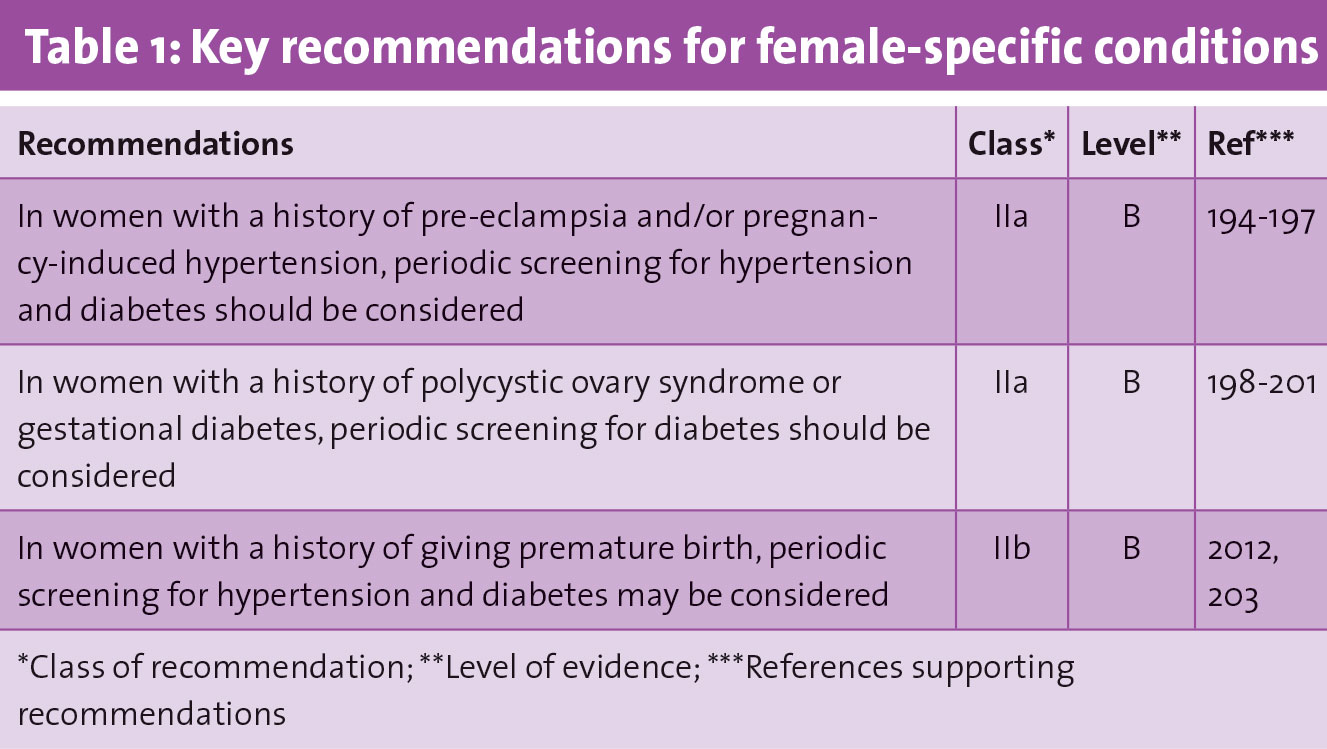
Obstetric complication such as pre-eclampsia and pregnancy-related hypertension are associated with a higher risk of CVD later in life.12, 13,14 What is not clear from the research is whether the increased CV risk after pre-eclampsia and pregnancy-related hypertension occurs independent of CV risk factors, as most of the studies did not adjust for the development of conventional risk factors.
However, despite this, the rationale for screening these women for hypertension and diabetes mellitus remains strong.
It is well established that gestational diabetes significantly increases the future risk of diabetes mellitus, with up to 50% developing it within a five-year period following pregnancy.15 Therefore, periodic screening should be considered for these women.
What is not evident from the new guidelines are recommendations regarding optimal prevention approaches, beyond screening to reduce future CV risk in this population.
In relation to non-obstetric conditions, polycystic ovary syndrome has been associated with an increased risk of CVD, hypertension and diabetes mellitus; however, the data regarding the CVD and hypertension risk is conflicting and more research is warranted.
Premature menopause has been associated with an increased risk of CVD; however there is insufficient evidence on a possible increased risk of hypertension or diabetes mellitus.1 Table 1 provides an overview of key recommendations for practice as outlined in the guidelines.
 (click to enlarge)
(click to enlarge)