CARDIOLOGY AND VASCULAR
GENERAL MEDICINE
RESPIRATORY
A case of rare pulmonary vascular anomaly
A rare case of pulmonary arteriovenous malformation (PAVM) in an otherwise fit and healthy 35-year-old male
December 18, 2015
-
Pulmonary arteriovenous malformations (PAVM) are rare pulmonary vascular anomalies. Although most patients are asymptomatic, PAVM can cause dyspnoea from right to left shunt, as well as embolic events, due to paradoxical emboli, resulting in stroke or brain abscess. In our case, a PAVM was incidentally observed in a 35-year-old male who presented with cough and temperature.
Introduction
PAVMs are caused by direct communication between the branches of pulmonary arteries and pulmonary veins without an intervening pulmonary bed.1 They have been variously called a pulmonary arteriovenous fistula, pulmonary arteriovenous malformation, pulmonary arteriovenous aneurysm, pulmonary angioma, cavernous haemangioma and pulmonary hamartomas.1 PAVM is the preferred term, since it represents a developmental defect (ie. congenital) in about 80% of cases.1
Most commonly they are associated with hereditary haemorrhagic telangiectasia (Osler-Weber-Rendu syndrome). Other conditions associated with PAVMs include:
- Idiopathic
- Infectious – actinomycosis, schistosomiasis
- Cardiac – mitral stenosis, certain corrective surgeries for congenital heart disease
- Hepatic – hepatopulmonary syndrome in cirrhosis
- Renal – Fanconi’s syndrome
- Malignancy – metastatic thyroid carcinoma
- Trauma – penetrating chest trauma.
Case report
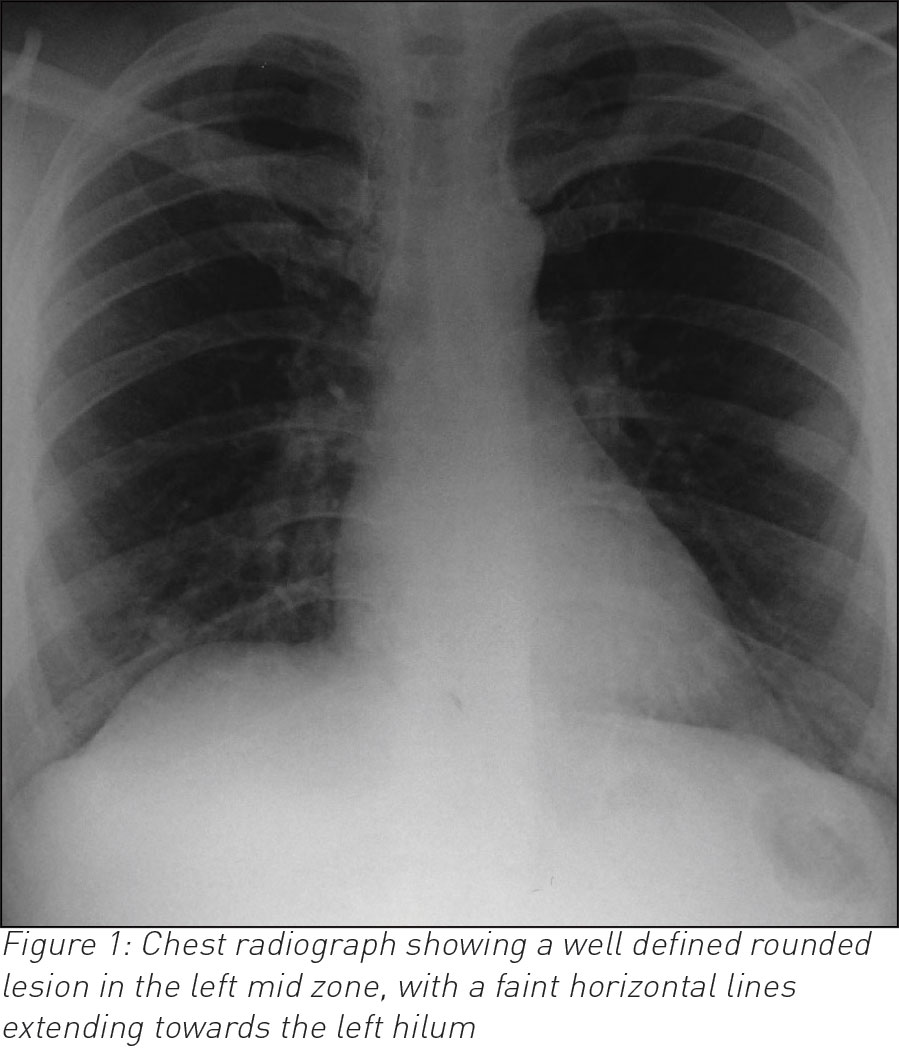
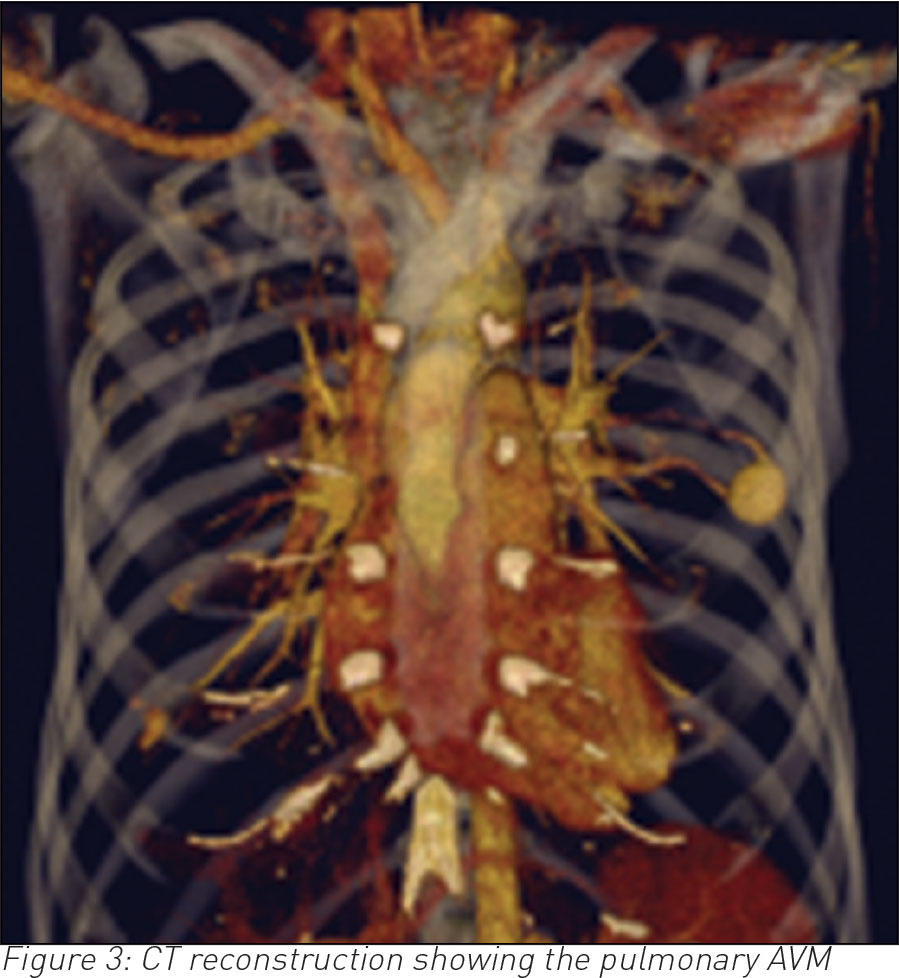
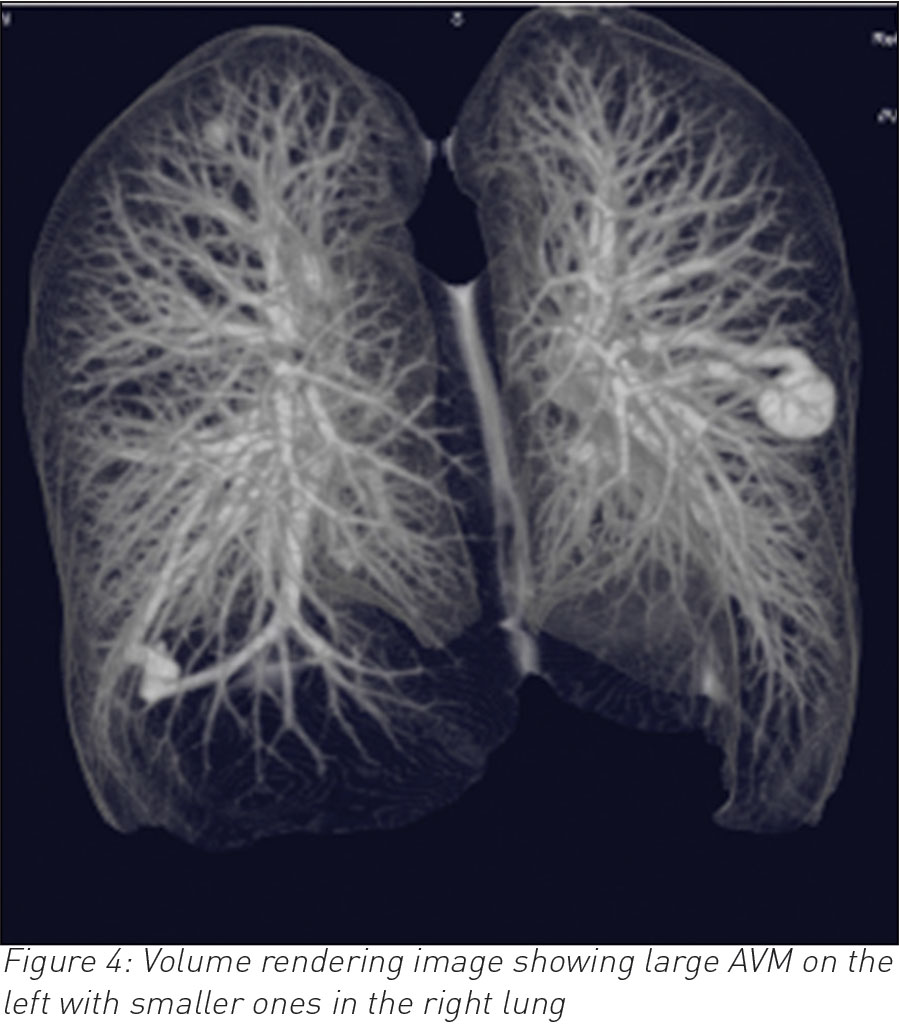
A 35-year-old male, who is otherwise fit and healthy, presented with a 10-day history of cough and temperature. Bloods showed raised white cell count otherwise normal. Chest infection was suspected and a chest radiograph was requested. The latter showed a well-rounded soft tissue opacity in the left midzone with possibly a connecting vessel radiating to the hilum. Two smaller opacities were identified in the right lung. A computed tomography (CT) pulmonary angiogram with intravenous contrast followed and that confirmed the diagnosis of a PAVM of 2cm in the left upper lobe and exquisitely demonstrated the feeding artery and vein with further smaller PVMs of 1cm in the right lung. The patient declined any further intervention.
CT renal angiography and MRI of the brain did not reveal any other aneurysms. PAVMs can be simple (single feeding artery) or complex (multiple feeding arteries).
Discussion
PAVMs are rare vascular anomalies that are more frequent in women.2,3 They are mostly congenital and have strong association with hereditary haemorrhagic telangiectasia (HHT). Approximately, 70-80% of cases of PAVM have HHT. Conversely, only 5-35% of the patients with HHT have PAVM.1,2 Most cases of PAVM are simple with one feeding artery but up to 20% can have complex (two or more) feeding vessels.3 They can be multiple in one third of cases,3 as in the present case.
PAVMs can potentially affect any part of the lung, but there is recognised predilection towards the lower lobes;1,3 the left lower lobe being the most common location, followed by the right lower lobe and right upper lobe.1
Although mostly asymptomatic, patients with PAVM may present with the classical triad of cyanosis, polycythaemia and clubbing of the fingers in 20% of cases.2 Other symptoms include dyspnoea, epistaxis, haemoptysis, palpitation and chest pain.1 Clinically a murmur or bruit may be audible over the lesion, especially if peripheral.3 Complications such as stroke, brain abscess or endocarditis may occur.1
A number of imaging modalities are available for the diagnosis of PAVM, including contrast echocardiography, computed tomography, magnetic resonance imaging (MRI) and the gold standard is pulmonary angiography.2,3 The latter would confirm diagnosis but also further defines the angio-architecture of pulmonary vasculature which is necessary before any therapeutic embolisation or surgical resection.1
CT is often the diagnostic modality of choice.3 It differentiates PAVMs from other causes of pulmonary nodules or masses. On CT, the characteristic presentation of a PAVM is a homogenous non-calcified nodule up to several centimetres in diameter or a serpiginous mass connected with blood vessels. Occasionally associated phleboliths may be seen as calcification. Contrast injection shows enhancement of the feeding artery, aneurysmal part and the draining vein.3
There is evidence that PAVMs progressively enlarge over a period of time and incidence of progression is higher in patients with untreated PAVM.1 Pulmonary AVMs are commonly stable in size, but up to 25% grow slowly. Pregnancy can also exacerbate growth, especially in the third trimester.
It is recommended that all symptomatic PAVMs and those bigger than 2cm in diameter be treated.2 Available options are either surgery or embolisation which is now considered firstline therapy since it is less invasive than surgery and has a lower complication rate.1,2 The risk of serial growth of occult lesions and recanalisation of previously embolised PAVM dictates that patients should have a regular follow up.1
In this case, our patient refused any intervention and has not developed any complications in the past seven years.
 (click to enlarge)
(click to enlarge)