GERIATRIC MEDICINE
An unusual case of high anion gap metabolic acidosis
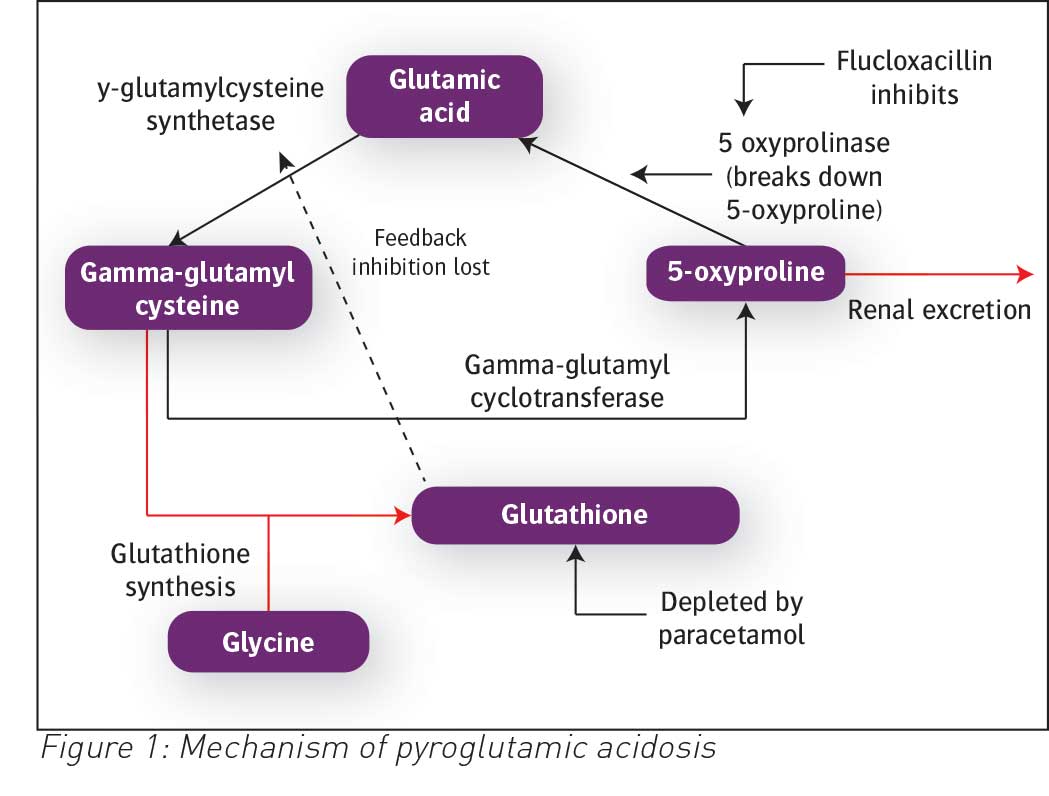
A patient with high anion gap metabolic acidosis secondary to pyroglutamic acid
October 31, 2019
-
An 80-year-old man was admitted under the orthopaedic team with a five-week history of progressive right hip pain. He had a background of a total hip replacement (THR) following a road traffic collision. His past medical history was significant for hypertension and type 2 diabetes with peripheral neuropathy. He had an excellent and independent functional baseline.
X-ray showed a loosening of the acetabular component of the previous THR and he was brought to theatre for a revision of THR. Intraoperatively, pus was noted on entering the joint capsule, and it was determined the loosening of THR was caused by a prosthetic joint infection. The intraoperative samples grew methicillin sensitive Staph aureus and he was commenced on a six week course of flucloxacillin after the joint was washed out during surgery.
On day 24 post op, he had a sudden deterioration. He become drowsy, hypotensive and tachypnoeic. Blood work revealed a metabolic acidosis with a pH of 7.203, unrecordable low pCO2, Po2 of 15 kPa, bicarbonate was 3.6. Anion gap was calculated at 35.2. He had an acute kidney injury with a creatinine of 151 (previous 108). The more common causes of metabolic acidosis were ruled out with a normal lactate, ketones, salicylate and ethanol levels.
He was treated with IV bicarbonate and N-acetyl cysteine which failed to correct the acidosis and subsequently the patient was brought to the intensive care unit for continuous venovenous haemodialysis (CVVHD). Due to the prolonged course of flucloxacillin and paracetamol, pyroglutamic acid toxicity was suspected. The patient improved quickly on haemodialysis; antibiotics were changed from flucloxacillin to ceftriaxone; and paracetamol was stopped. A week later the result of serum sample for pyroglutamic acid returned as markedly elevated.
 (click to enlarge)
(click to enlarge)