Bleeding duodenal varices: ‘a clip in time saves nine’
A case of duodenal variceal bleeding secondary to liver cirrhosis which was managed using haemoclips and TIPS
Mr Syed Sohail Ahmad, Surgical Registrar, Letterkenny University Hospital, Donegal, Mr Kaleem Khalilullah, Senior Surgical Registrar, Letterkenny University Hospital, Dublin, Dr Chris Steele, Consultant Gastroenterologist, Letterkenny University Hospital, Donegal and Dr Elzamzami Obai, Department of Surgery and Gastroenterology, Letterkenny University Hospital, Donegal
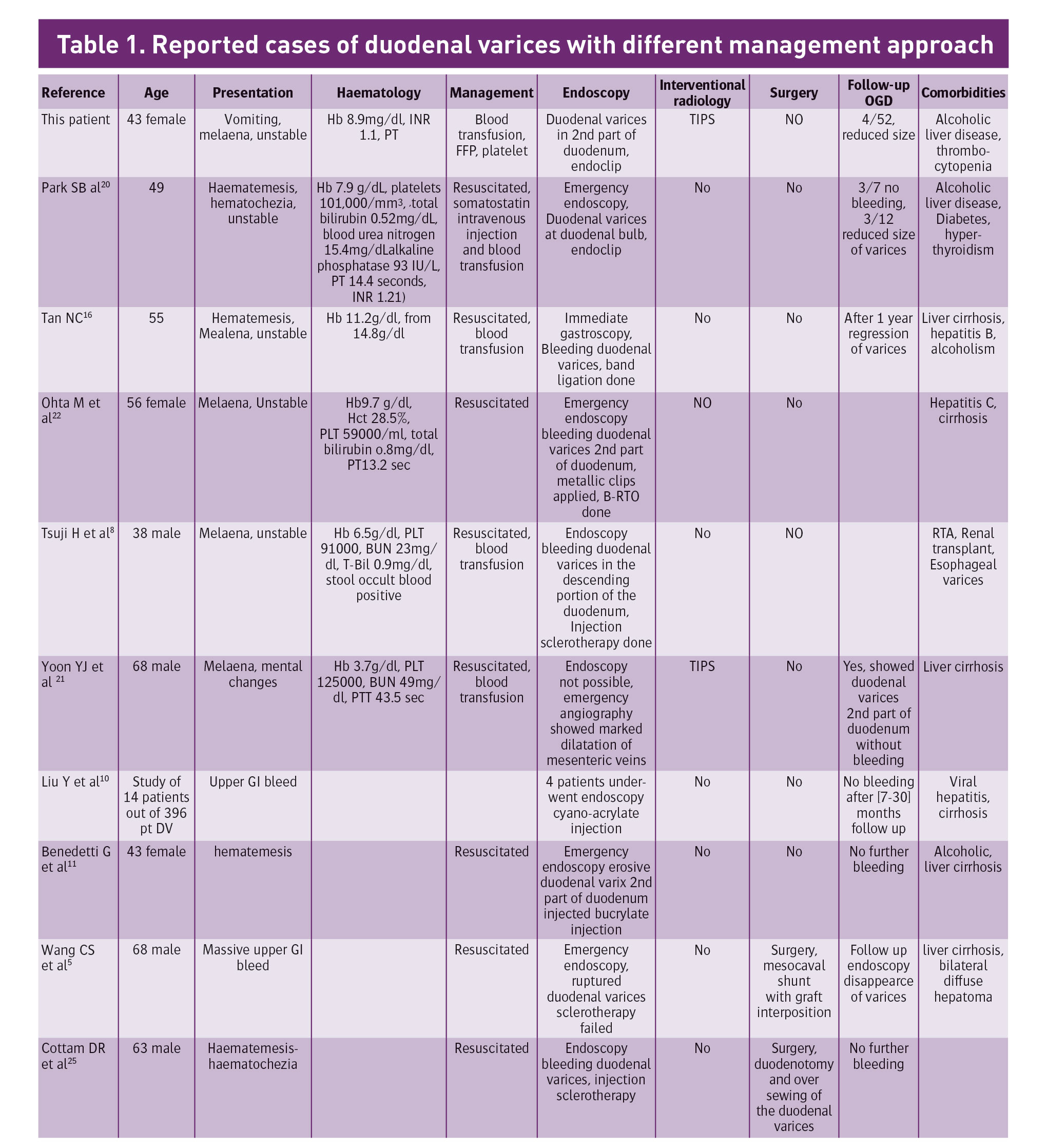
Haemorrhage associated with duodenal varices is an uncommon but often fatal manifestation of portal hypertension with a mortality of nearly 40% and a poor prognosis. We report a case of a 43-year-old female who presented to the emergency department with unstable upper gastrointestinal bleed and had an urgent oesophago-gastro-duodendoscopy (OGD), which showed bleeding duodenal varices in the second part of duodenum which was clipped. She was referred to the tertiary care centre where she had TIPS (transjugular intrahepatic portosystemic shunt). Post TIPS she did well and had follow up OGD done after four weeks, which showed collapsed varices and clips in-situ. We reported the case to suggest that duodenal variceal bleeding secondary to liver cirrhosis can be managed using haemoclips and TIPS.
The woman presented to the emergency department with the complaint of coffee ground vomiting and melaena. She was haemodynamically unstable with a pulse of 110/min, BP 85/50mm/hg. Her baseline haemoglobin which was 13.5mg/dl dropped to 8.9mg/dl. She had a history of alcoholic liver disease, thrombocytopenia, and a Caesarean-section. She was drinking heavily prior to presentation to ED. Blood investigations showed bilirubin of 31umol/L, AST 84 U/L, ALT 49 U/L, GGT 181 U/L, ALP 89 U/L, PT 12.2 sec, INR 1.1, APTT 28.8sec, urea 2.5, Cr 51, albumin 26g/L, PLT101 [140-450] 10 9/L, hepatitis screen was negative. On examination, there was fullness and tenderness in the epigastrium. Per-rectal examination showed melaena. She was resuscitated and had urgent gastroscopy done which showed early oesophageal varices and bleeding duodenal varices 3cm in size in the second part of the duodenum, which was clipped. She was kept in the high dependency unit and put on terlipressen, antibiotics and had two units of blood transfusion, pool of platelet, and FFP. During her stay in the HDU she had a further two episodes of melaena, and one episode of bleeding per rectum. She was planned for TIPS. Her triphasic CT liver showed patent portal vein.
She did well after the procedure with no further episode of melaena and her haemoglobin was stable at 11gm/dl. She was discharged. Follow-up gastroscopy after four weeks showed collapsed duodenal varices with clip in-situ. She will be followed up as an outpatient.
(click to enlarge)
(click to enlarge)
Discussion
Duodenal varices are rare, occurring in 0.4% of patients with portal hypertension. The aetiology of duodenal varices can be classified into hepatic (eg. cirrhosis) or extra hepatic (eg. portal, splenic or superior mesenteric vein thrombosis). Variceal bleeding mainly occurs in the oesophagus or the stomach, but can also rarely occur in the duodenum, jejunum, ileum, appendix, colon, rectum and the biliary tract. Of these, duodenal variceal bleeding has a mortality of 40% and a poor prognosis.1 The most common cause of duodenal varices is portal hypertension due to liver cirrhosis (30%). Other causes include occlusion of the splenic vein due to pancreatitis, tumours or thrombosis (25%), and occlusion of the portal vein due to thrombosis, infection and tumours (25%).2
Duodenal varices were first recognised radiologically by Alberti in 1931,3 while Kunisaki et al4 reported the first case of duodenal varices visualised by endoscopic examination in 1973. The most common site is the duodenal bulb, followed by the second part of the duodenum.5
The pathogenesis is due to the increasing portal venous pressure which causes portosystemic communication. Duodenal varices are one of the ectopic varices caused by retroperitoneal portosystemic shunts. This is due to the increase in hepatofugal blood flow through the cystic branches of the pyloric veins, gastroduodenal veins, and the superior and inferior pancreatic duodenal veins.6
Endoscopy is the mainstay in the diagnosis of bleeding duodenal varices, however it can be difficult due to heavy bleeding or if the varices are located in the lower portion of the second part of the duodenum. If the site of bleeding cannot be identified, options include mesenteric angiogram, multihelical CT and exploratory laparotomy.
Management of bleeding duodenal varices is still debatable due to limited experience. Currently, there is no data available for primary prophylaxis of duodenal varices, but beta-blockers have been used to prevent rebleeding, despite the lack of supporting evidence. Due to the infrequency of duodenal variceal bleeding, there are no randomised studies on its management, and medical literature on treatment options is limited to case reports or small series.7 It can be treated endoscopically, radiologically or surgically, each having its pros and cons and depending on the expertise of the centre.
Most forms of endoscopic treatments reported have employed injection sclerotherapy to achieve haemostasis for bleeding duodenal varices.1 However, there has not been consistent successful results with injection sclerotherapy. Several types of sclerosing agents have been used, including ethanolamine, polidocanol, dextrose 50% solution with 3% sodium tetradecylsulfate and polidocanol/thrombin.8,9 Sclerosing agents have a damaging effect on the surrounding tissue, with complications such as perforation, embolism and tissue injury possible.10 In recent years, the tissue adhesive n-butyl-2-cyanoacrylate (Histoacryl) has been successfully used for endoscopic homeostasis of oesophageal and fundal varices. Endoscopic embolisation by Histoacryl has also been tried successfully in securing haemostasis for bleeding duodenal varices,11,12 the rate of re-bleeding with Histoacryl sclerotherapy is also high.13
There has been limited experience with endoscopic banding for bleeding duodenal varices. Tazawa et al reported a case of duodenal variceal bleeding successfully controlled with endoscopic ligation, but the patient died of liver failure two days later.14 In another case, temporary haemostasis was achieved with endoscopic ligation, and this was followed by balloon-occluded retrograde transvenous obliteration a month later.15 Tan et al also reported successful management of bleeding duodenal varices with band ligation but the size was small (1.5cm).16 The size of a duodenal varix may determine if it is possible to do band ligation endoscopically. If a varix is large, it is difficult to band the whole varix and large defects can occur when the band is removed.1
Haemoclips are designed as an alternative treatment to control bleeding by direct mechanical pressure. Haemoclips generally fall off after 10-14 days of clipping, after the lesion has partly healed and is not expected to rebleed.17 The effectiveness of endoscopic clipping in the haemostasis of bleeding oesophageal varices could be compared with that of band ligation Yolk et al.18 Considering the advantage of high initial haemostasis rate and decreased risk of bleeding, they suggested that endoscopic clipping is more effective than band ligation. Morimoto et al19 have reported a case where active gastric variceal bleeding was treated using metallic clips. Park SB et al20 reported a case of bleeding duodenal varices managed by putting haemoclips on both the afferent and efferent part of the varix together. In our case we used haemoclips to control the bleeding duodenal varices, which resulted in the arrest of bleeding with immediate effect. This patient had TIPS later and repeat OGD after four weeks, which showed collapsed varices with the clips in-situ and stable haemoglobin.
TIPS is a relatively safer treatment method and is used in patients with poor liver function or if the endoscopic accessibility is limited due to severe bleeding. Thus, TIPS can be used in patients with Child-Pugh class B or C, who are candidates for liver transplantation, if endoscopic or radiological embolisation therapy fails. There have been cases where TIPS was used alone, or as a second-line therapy when endoscopic treatment methods failed.21 TIPS is of limited use in patients with severe liver atrophy and can increase the risk of developing complications such as hepatic encephalopathy or cerebral embolisation.22,23 In our case the patient initially had clipping done which arrested the bleeding but later had episodes of melaena and had TIPS done. Her repeat OGD showed collapsed varices.
Surgical operations used in the management of bleeding duodenal varices include procedures such as varices suture ligation, varices resection with or without duodenal resection, Porto-systemic shunts, and spleno-renal anastomosis but the rate of postsurgical mortality is as high as 30% and such methods are not commonly used in recent years.24 Cottam DR reported managing a case of failed injection sclerotherapy by simple over sewing of the duodenal varices through a duodenotomy.25 Surgery is preferred in patients with Child-Pugh class A and in patients with extra-hepatic portal vein thrombosis. In the review of Khouqeer on the surgical treatment of duodenal varices, the portocaval shunt was the most effective method of preventing recurrent haemorrhage.24
(click to enlarge)
Conclusion
In bleeding, duodenal varices endo-clipping can be used as a first line of therapy along with TIPS if the patients are still symptomatic and bleeding to achieve haemostasis. We recommend that in patients with life-threatening haemorrhage from duodenal varices caused by cirrhosis of the liver, transjugular intrahepatic portosystemic shunt be considered in the management.
References
Norton ID, Andrews JC, Kamath PS. Management of ectopic varices. Hepatology 1998;28:1154-1158
Kotfila R, Trudeau W. Extraesophageal varices. Dig Dis 1998; 16:232-241
Alberti W. Über den rontgenologischen nachweise von varizen imbulbus duodeni. Fortschr Geb Rontgenstr 1931; 43:60
Kunisaki T, Someya N, Shimokawa Y et al. Varices in the distal duodenum seen with a fiber duodenoscope. Endoscopy 1973; 5:101-4
Wang CS, Jeng LB, Chen MF. Duodenal variceal bleeding successfully treated by mesocaval shunt after failure of sclerotherapy. Hepatogastroenterology 1995; 42:59-61
Itzchak Y, Glickman MG. Duodenal varices in extra hepatic portal obstruction. Radiology 1977;124:619-624
Attila T, Kolbeck KJ, Zachary M et al. Duodenal variceal bleeding successfully treated with transjugular intrahepatic portosystemic shunt: A case report and review of the literature. Turk J Gastroenterol 2008; 19 (4): 284-290
Tsuji H, Okano H, Fujino H, et al. A case of endoscopic injection sclerotherapy for a bleeding duodenal varix. Gastroenterol Jpn 1989; 24:60-64
Sans M, Leach J, Boards JM et al. Thrombin and ethanolamine injection therapy in arresting uncontrolled bleeding from duodenal varies. Endoscopy 1996; 28:403
Liu Y, Yang J, Wang J et al. Clinical characteristics and endoscopic treatment with cyanoacrylate injection in patients with duodenal varices. Scand J Gastroenterol 2009; 44:1012-1016
Benedetti G, Sablich R, Lacchin T et al. Endoscopic treatment of bleeding duodenal varices by bucrylate injection. Endoscopy 1993; 25:432-3
Yoshida Y, Imai Y, Nishikawa M et al. Successful endoscopic injection sclerotherapy with N-butyl-2-cyanoacrylate following the recurrence of bleeding soon after endoscopic ligation for ruptured duodenal varices. Am J Gastroenterol 1997; 92:1227-9
Akahoshi T, Hashizume M, Shimabukuro R et al. Long-term results of endoscopic Histoacryl injection sclerotherapy for gastric varicealbleeding: a 10-year experience. Surgery 2002; 131 (1 suppl):S176-81
Tazawa J, Sakai Y, Koizumi K et al. Endoscopic ligation for ruptured duodenal varices. Am J Gastroenterol 1995; 90:677-8
Haruta I, Isobe Y, Ueno E et al. Balloon-occluded retrogradetransvenous obliteration (BRTO), a promising nonsurgical therapy for ectopic varices: a case report of successful treatment of duodenalvarices by BRTO. Am J Gastroenterol 1996; 91:2594-7
Tan NC, Ibrahim S, Tay KH. Successful management of a bleeding duodenal varix by endoscopic banding Singapore Med J 2005; 46(12): 723
Shin EJ, Ko CW, Magno P et al. Comparative study of endoscopic clips: duration of attachment at the site of clip application. Gastrointest Endosc 2007; 66:757-761
Yolk S, Belviranli M, Toprak S, Kartal A. Endoscopic clipping versus band ligation in the management of bleeding oesophageal varices. Surge Endosc 2003; 17:38-42
Morimoto T, Fu KI et al. Endoscopic haemostasis with hemoclips for active gastric variceal bleeding. Endoscopy 2010; 42(Suppl 2):E333-E334
Park SB, Lee SH, Kim JH et al. Successful treatment of duodenal variceal bleeding by endoscopic clipping. Clin Endosc 2013 Jul; 46(4):403-406
Yoon YJ, Hahn KH, Lee SY et al. A case of massive bleeding duodenal varices successfully controlled with transjugular intrahepatic portosystemic shunt. Korean J Gastroenterol 2001; 38:292-295
Ohta M, Yasumori K, Saku M et al. Successful treatment of bleeding duodenal varices by balloon-occluded retrograde transvenous obliteration: a transjugular venous approach. Surgery 1999; 126:581-583
Ponec RJ, Kowdley KV. Paradoxical cerebral emboli after transjugular intrahepatic portosystemic shunt and coil embolization for treatment of duodenal varices. Am J Gastroenterol 1997; 92:1372-1373
Khouqeer F, Morrow C, Jordan P. Duodenal varices as a cause of massive upper gastrointestinal bleeding. Surgery 1987;102:548-552
Cottam DR, Clark R, Hayn E, Shaftan G. Duodenal varices: a novel treatment and literature review Am Surg 2002 May;68(5):407-9
 (click to enlarge)
(click to enlarge)