Childhood cancers and the importance of early detection
While early detection is paramount, newer innovative treatments such as proton beam therapy (PBT) and CAR T-cell therapy are improving outcomes for children and adolescents with cancer
Ms Amy Nolan, Head of Children Adolescents & Young Adults, Irish Cancer Society, Dublin, Ms Rebecca Gorman, Advocacy Officer, Children Adolescents & Young Adults, Irish Cancer Society, Dublin and Ms Elaine Smyth, Children’s Cancer Coordinator Nurse, Irish Cancer Society, Dublin
A cancer diagnosis within a family is always a traumatic event, with the impact amplified when it concerns a child being diagnosed. There are approximately 200 cases of cancer diagnosed in the children under the age of 16 years in Ireland annually and it remains the primary disease-related cause of death in children.1
The average number of children, adolescent and young adult (CAYA) cancers diagnosed in Ireland per year by age at diagnosis is:1
200 (0-15 years + 364 days)
70 (15-19 years + 364 days)
110 (20-24 years + 364 days) annually.
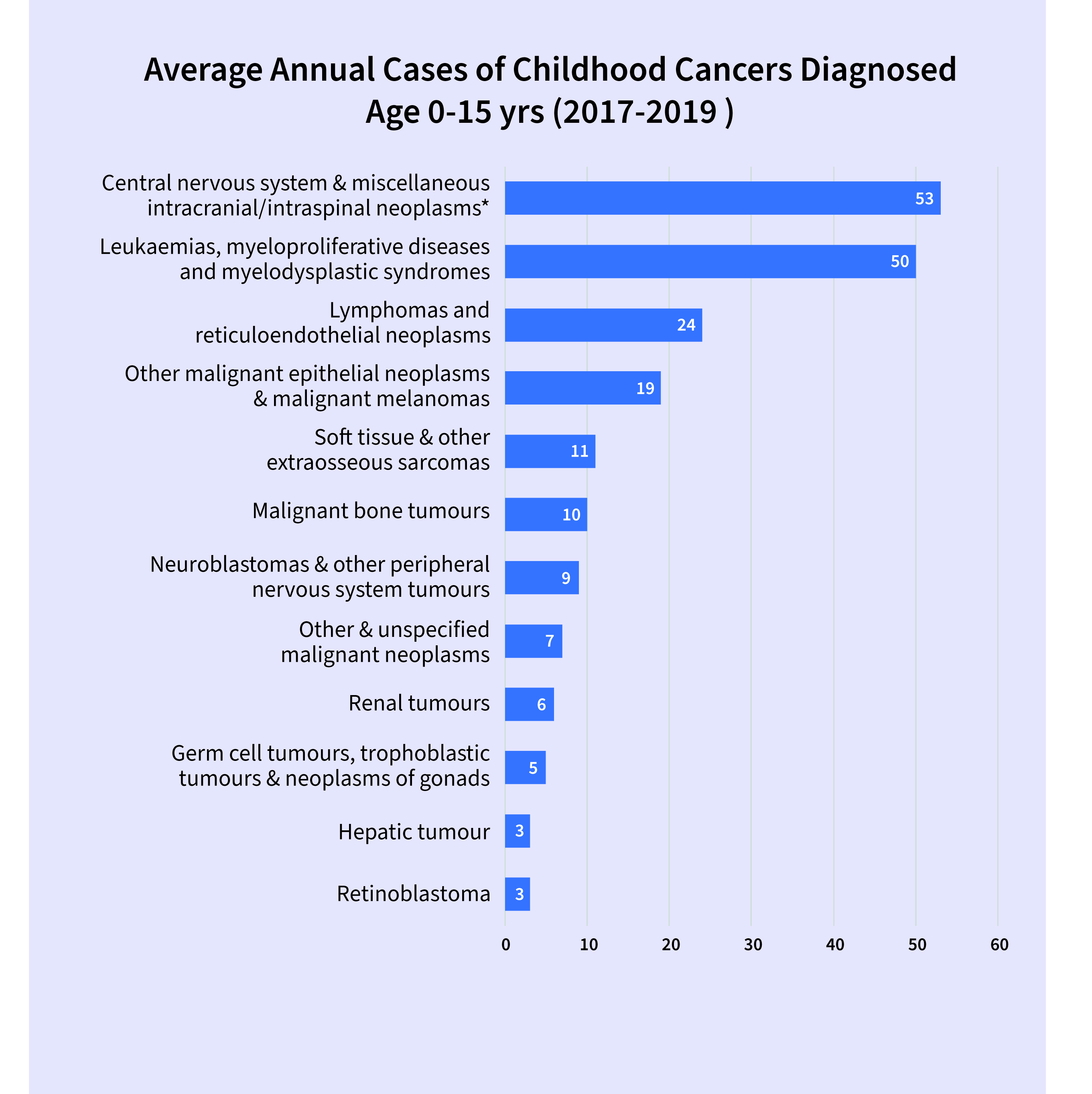
Cancer can present in many forms, with the most common cancers in children being leukaemia, cancer of the brain and central nervous system, and lymphoma (see Figure 1).
(click to enlarge)
Treatment pathway
Upon diagnosis, children under 16 years are typically referred to the National Children’s Cancer Service (NCCS) at Children’s Health Ireland at Crumlin, to confirm their diagnosis and extent of disease, and to outline the treatment plan and extended care plan. As 60% of patients live outside of the Dublin catchment area, the NCCS programme is supported by 16 shared care paediatric units across Ireland. Shared care hospitals provide essential supportive care and components of treatment locally, including the management of side effects related to cancer treatment and disease, under the guidance of the NCCS (in accordance with the NCCS programme Supportive Care Guidelines).2 Depending on the diagnosis, treatment can last from a few months up to three years, and the patient may potentially remain under clinical surveillance into adulthood.
Treatment developments
Treatment modalities mainly consist of surgery, chemotherapy and radiotherapy and in the past 20 years treatment for childhood cancers have significantly advanced with cancer clinical trials accessible to the majority of patients under 15 years of age.
Excitingly, newer innovative treatments including immunotherapies, targeting specific cancer cells are used concomitantly with chemotherapy and as singular agents to enhance survivorship.
Proton beam therapy (PBT) is administered to children with some solid tumours. Using protons rather than high energy x-rays to cause apoptosis of cancer cells. PBT reduces the risk of long-term side effects from the treatment by sparing the normal tissue surrounding the tumour. Children and young adults particularly benefit from this type of radiotherapy as their tissue and organs are still developing. The therapy is not currently available in Ireland and many Irish children travel to Essen in Germany or The Christie Hospital in Manchester for PBT, which is funded under the HSE Treatment Abroad Scheme.
Some children with leukaemia, refractive lymphoma, solid tumour, central nervous system (CNS) tumour, and non-malignant diseases such as metabolic, autoimmune or haematopoietic disorders, may require bone marrow transplant. This requires high-dose chemotherapy and, where indicated, total body irradiation, followed by a haematopoietic stem cell transplant (HSCT) which may be autologous (from the child themselves) or allogeneic (matched donor). Stem cells can be collected from the bone marrow, peripheral blood or the umbilical cord at birth. The stem cell transplant replaces diseased or damaged blood cells with cancer-free stem cells.
The diseased or damaged cells may be the result of cancer or cancer treatments where the body is unable to produce healthy blood cells.
One of the most innovative developments in recent years in treating children with acute lymphocytic leukaemia (ALL) is the innovation of CAR T-cell treatment. The first CAR T-cell therapy was delivered in Ireland in CHI Crumlin in April 2022. This is a revolutionary new cellular therapy. CAR T-cell therapy is a type of immunotherapy which works by using the patient’s immune system to fight the cancer. CAR T-cell therapy involves taking the patient’s own T cells, then reprogramming them in a laboratory so that they are better equipped to seek out and target cancer cells. This is different to a bone marrow transplant, where donor cells provide the immune function. Research is ongoing to extend this treatment to other cancers.
Improvements in transplant and cellular therapy technique and supportive care has led to an increase in survivors. However, there is associated high morbidity and patients remain at high risk of early and long-term complications impacting on quality of life and requiring lifelong surveillance.3
As a result of such developments the overall survival rate for children with cancer is high at over 80%.4 However, ‘survivorship’ no longer means just surviving cancer, it incorporates quality of life into adulthood for childhood cancer survivors. Often survivors must address their lifelong side effects of treatment, known as ‘late effects’. As they move into adulthood, they have an increased risk of developing comorbidities such as cardiac issues, mental health issues, cancer recurrence, hearing loss and developmental issues.4
Detection
Childhood cancer is not preventable through life-style interventions, as is the case in many adult cancers, therefore the early detection of childhood cancer in the community is essential. As infants and children grow, emergence of bone, germ cell and neural tumours can occur as a result of inherited or de novo genetic mutations. These cancers generally have an acute presentation.5
However, childhood cancer can be challenging to diagnose, as symptoms are often vague and can appear to ‘mirror’ more-common childhood ailments.6,7
Coupled with an assumption that childhood cancer is ‘rare’, these combined challenges mean that efforts to improve cancer symptom awareness in young people, families and healthcare practitioners is required.
The earlier that cancer is diagnosed, the chances that more intensive combinations of treatments will be required is less, and the burden of late-effects in survivors will be reduced. Early diagnoses improves health-related quality of life in adolescents and young adults, with increased mental health difficulties also experienced in this vulnerable group.8
The chances of an individual healthcare professional seeing childhood cancer in their career is rare, how-ever, the individual risk of developing childhood cancer remains as high as cases of illnesses such as diabetes, epilepsy or bacterial meningitis.9 It is important therefore to support healthcare professionals in the community to detect this life-threatening disease as soon as possible, in order to ensure diagnostic intervals are minimised for this group to get access to treatment when they need it.
Symptom awareness
Awareness of childhood cancer symptoms among the general public in Ireland is low. An omnibus survey conducted in September 2022 by Core research on behalf of the Irish Cancer Society found some disheartening figures for symptom awareness in CAYA cancers. Of the population surveyed, 84% were not aware of the most common symptoms of childhood cancer, which includes issues with balance, co-ordination or speech problems; loss of appetite or weight loss; and an unexplained lump, swelling or pain.10 The Irish Cancer Society supports the development of a nationwide campaign to improve awareness of childhood cancer symptoms for families and to encourage them to visit their GP when these occur.
Referral guidelines and awareness campaigns in the UK have brought about improved awareness and early detection, particularly of paediatric brain tumours. ‘Childhood Cancer Smart’, a collaboration of cancer charities and research institutions in the UK, is building a framework with research, campaigns and information development all supporting the early detection of childhood cancer.11
Ireland can learn from these projects and ensure our children can access excellent cancer care when they need it via increased public awareness of the common symptoms of childhood cancer, and timely referral to specialists via their GP.
Symptoms of childhood cancers (unusual, unexplained and won’t go away)12
Balance, co-ordination or speech problems
Loss of appetite or weight loss
An unexplained lump, swelling or pain
Fits or seizures
Changes in eyes or vision: a squint, pain or a white glow in photos
Swollen lymph nodes in the neck or groin
Feeling very tired most of the time
Regular night sweats or high temperature
Nausea and vomiting
Blood in urine or faeces
Bruising or bleeding under the skin that looks like a rash
Regular headaches/early morning vomiting
Awareness and early detection
Greater awareness and earlier detection of childhood cancer will increase survival rates and ensure earlier commencement of treatment pathways which may result in less toxic treatments, reducing the likelihood of long-term side effects of treatment.
A priority for the Irish Cancer Society is to collaborate with stakeholders across Ireland to increase awareness of childhood cancer for both healthcare professionals and the general public in order to avoid delayed diagnosis and disease progression for children in Ireland.
Patients and relatives can call Freephone 1800 200 700 or email supportline@irishcancer.ie and speak to a cancer nurse or be referred to the children’s cancer coordinator nurse for confidential advice and information. The support line is open Monday to Friday, 9am-5pm
Childhood cancer facts13
250 children and teenagers up to 19 years are diagnosed with cancer each year in Ireland
Almost 82% of children with cancer in Ireland with survive their cancer for five years or more
On average 50% of all childhood cancers are leukaemia, lymphoma, tumours of the brain and central nervous system
Childhood cancer is not preventable through lifestyle interventions
Childhood cancer can be challenging to diagnose, as symptoms are often vague and can appear to ‘mirror’ more-common childhood ailments
References
National Cancer Control Programme. Framework for the Care and Support of Adolescents and Young Adults (AYA) with Cancer in Ireland (2021-2026). 2021
Department of Health. National Cancer Strategy (2017-2026), 2017 (Jul)
Hierlmeier S, Eyrich M, Wölfl M, Schlegel PG, Wiegering V. Early and late complications following hematopoietic stem cell transplantation in pediatric patients – A retrospective analysis over 11 years. PLOS ONE 2018 ; 13(10): e0204914. https://doi.org/10.1371/journal.pone.0204914
Bhakta N, Liu Q, Ness KK, Baassiri M et al. The cumulative burden of surviving childhood cancer: an initial report from the St Jude Lifetime Cohort Study (SJLIFE). The Lancet 2017 Dec 9; 390(10112):2569-82
Pruteanu DP, Olteanu DE, Cosnarovici R, Mihut E, Nagy V. Genetic predisposition in pediatric oncology. Med Pharm Rep 2020 Oct; 93(4):323-34
Lethaby CD, Picton S, Kinsey SE, Phillips R, van Laar M, Feltbower RG. A systematic review of time to diagnosis in children and young adults with cancer. Arch Dis Child 2013 May; 98(5):349-55
Herbert A, Lyratzopoulos G, Whelan J, Taylor RM, Barber J, Gibson F, et al. Diagnostic timeliness in adolescents and young adults with cancer: a cross-sectional analysis of the BRIGHTLIGHT cohort. Lancet Child Adolesc Health 2018 Mar; 2(3):180-90
Forster AS, Herbert A, Koo MM et al. Associations between diagnostic time intervals and health-related quality of life, clinical anxiety and depression in adolescents and young adults with cancer: cross-sectional analysis of the BRIGHTLIGHT cohort. Br J Cancer 2022 Jun 1; 126(12):1725-34
Walker DA. Helping GPs to diagnose children’s cancer. Br J Gen Pract 2021 Apr 1; 71(705):151-2
Irish Cancer Society. Omnibus Survey. 2022 Sep, www.cancer.ie
Childhood Cancer Smart campaign www.cclg.org.uk/more-about-child-cancer-smart
Better safe than tumour - Signs and Symptoms (headsmart.org.uk)
 (click to enlarge)
(click to enlarge)