Chronic mid-portion Achilles tendinopathy can affect both recreational and elite athletes
Dr Claire Kennedy, Specialist Registrar, Cork University Hospital, Cork, Dr Sinead Harney, Consultant Rheumatologist, Cork University Hospital, Cork and Dr Owen Cronin, Medical SHO, Cork University Hospital, Cork
Chronic mid-portion Achilles tendinopathy is a degenerative condition affecting both recreational and elite athletes. However, sedentary individuals who commence regular, unaccustomed activity can also be affected.
Figure 1. Longitudinal colour Doppler ultrasound of the Achilles tendon showing both hypoechoic regions and areas of neovascularisation(click to enlarge)
Clinical features
Presenting features include a ‘burning’ pain or stiffness localised 2-6cm above the insertion of the Achilles tendon to the calcaneus. This sensation is invariably exertional in nature. A detailed history may include a sudden increase in levels of physical activity or an increase in training intensity that precedes the onset of symptoms. Often, the intensity of training performed is excessive compared to baseline levels of fitness.
In the case of the elite athlete, there may be a history of over-training without allowance for recovery of the tendon from recurrent micro-trauma. Use of poorly fitted or worn footwear and hill training are additional risk factors. Poor biomechanical function can put individuals at risk, particularly tight gastrocnemius and soleus muscles and the resultant excessive pronation.
Chronic Achilles tendinopathy, as distinct from acute tendonitis, is defined when pain persists greater than three months. Lifetime incidence in competitive athletes is estimated to be 24%.1 Clinical examination may reveal an enlarged and painful tendon. Peri-tendinous pain might indicate an alternative pathology, eg. ankle pathology.
Complete rupture of the Achilles tendon should always be excluded using the Thompson-Simmonds’ calf-squeeze test.2 Dorsiflexion and plantar flexion may elicit crepitus over the tendon. Pain can be reproduced by applying a loading force across the tendon, eg. single-leg heel raise.
Diagnosis and imaging
Achilles tendinopathy is a clinical diagnosis re-enforced by radiological imaging. Imaging should not be relied upon in isolation as neither T2-weighted MRI nor high quality ultrasound are highly specific.3
Although clinical features (ie. pain, tenderness, swelling, impaired function) may imply inflammation as an underlying process, histology does not demonstrate inflammatory cells but rather microfibre collagen disarray, increased ground substance, partial macroscopic tears and surrounding oedema.
During surgical exploration, hyper-vascularity is present without evidence of effective healing. In fact, abnormal neovascularisation can be observed on ultrasound. Hypoechoic areas of the tendon signify regions of fibre disarray. Treatment options can be classified into conservative, injectable therapies and surgical interventions.
Conservative management
Eccentric exercise
Eccentric exercise involves focusing on the elongation phase of muscle action. Alfredson’s heel drop programme was first described in 1998.4 It consists of a 12-week programme incorporating two types of heel drops (the gastrocnemius and soleus drops). Although time-consuming and lengthy, successful completion of Alfredson’s protocol improves symptom scores at one year and is sustained at five years post-diagnosis.5,6 Radiological findings also improve although the correlation between radiological improvement and clinical improvement remains questionable.7
The benefit of adding a night-time splint is controversial and studies have produced conflicting evidence.8,9 Disadvantages of eccentric exercise as a mainstay of treatment include the difficulty in ensuring patient compliance with the regularity of the exercise programme. This is particularly true as exercises are likely to be painful during the initial phases of the programme. Also, the duration of treatment is also problematic, particularly for high-end athletes wishing to return to sport imminently.
Extra-corporeal shockwave therapy
Extra-corporeal shockwave therapy (ESWT) offers a cheap, relatively painless, easily administrable option in the treatment of chronic Achilles tendinopathy. ESWT stimulates soft-tissue healing primarily by inhibiting afferent pain-receptor function and by enhancing angiogenesis.10,11 In practice, it is used more often to reduce pain for short periods allowing the patient to focus on eccentric exercise.12
Topical nitrate therapy
Application of topical glyceryl trinitrate (GTN) patches locally to the affected tendon provides sustained symptom relief during exercise by 12 weeks if used daily.13 A commonly used dose is 1.25mg of GTN per day. In chronic patellar tendinopathy, GTN in conjunction with eccentric exercise programmes shows average results at decreasing pain scores over 24 months.14
However, long-term outcomes for the use of GTN in Achilles tendinopathy are unclear. Dizziness and headaches are theoretical, but rare side-effects.
Injectable therapies
Injection of sclerosing agents
Polidocanol is a sclerosing agent, with additional anaesthetic properties, used in the treatment of chronic tendinopathies (Achilles and patellar) as well as varicose veins.15,16,17 Polidocanol is thought to work selectively in the vascular intima causing thrombosis of small vessels. This is particularly pertinent to chronic tendinopathies, where neovascularisation is thought to be part of the underlying pathophysiology. It can be administered under colour Doppler ultrasound guidance with the patient lying prone. The substance is injected into the tendon at regions where neovascularisation exists until vascular flow disappears. Small quantities (0.1-1ml) of the substance are required and concentration (5mg/ml versus 10mg/ml) does not appear to affect results.18
Following therapy, rehabilitation consists of one to three days of rest followed by a gradual increase in tendon-loading activity culminating in maximal loading after two weeks.
Miscellaneous injectable therapies
High-volume image-guided injection and aprotinin
In more recent years alternative injectable therapies have been studied. Aprotinin is a basic pancreatic trypsin inhibitor derived from bovine lung. Previous uses of aprotinin include cessation of bleeding post-operatively.19 Allergic reaction is, unfortunately, a relatively common side-effect. High-volume, image-guided intra-tendinous injections have been studied with various combinations of substances.
A case series of 94 athletes injected with a combination of 10ml of 0.5% bupivacaine, 25mg of aprotinin and 40ml of 0.9% normal saline showed promising results for the treatment of Achilles tendinopathy.20 Another combination of 10mls of 0.5% bupivacaine, 25mg of hydrocortisone and 40ml of 0.9% saline also showed improvements in both symptomatic and radiological scores.21
Platelet-rich plasma
Injection of autologous, centrifuged platelet-rich plasma (PRP) is a novel therapy being studied and used in the treatment of various musculoskeletal disorders.
It has been shown to be of benefit compared to other therapies in the treatment of tennis elbow (lateral epicondylitis).22,23
In the treatment of chronic Achilles tendinopathy, several small, randomised, controlled trials have not demonstrated superiority of PRP over control (small volume saline injection), in both clinical and radiological outcomes.24,25,26 Currently, PRP injections are not recommended in the treatment of chronic mid-portion Achilles tendinopathy.
Corticosteroid injection
Peri-tendinous injection of corticosteroid in Achilles tendinopathy is generally thought to have short-term analgesic effects. Intra-tendinous corticosteroid injection is contra-indicated due to its catabolic effects and inhibition of collagen synthesis.27 Some reports of Achilles tendon rupture following intra-tendinous corticosteroid injection are also described.28,29
Surgical intervention
Surgical intervention for mid-portion Achilles tendinopathy includes open removal of diseased tendon tissue and percutaneous tenotomy. Open surgery produces its most successful results in cases where diffuse tendon disease exists.30 Percutaneous tenotomy offers good or excellent results in 75% of patients.31
Both open and percutaneous surgical methods require extensive and reliable rehabilitation in order to achieve successful outcomes.
References
Kujala UM, Sarna S, Kaprio J. Cumulative incidence of achilles tendon rupture and tendinopathy in male former elite athletes. Clin J Sport Med 2005; 15: 133
Thompson T. A test for rupture of the tendo achillis. Acta Orthop Scand 1962 32;1-4): 461-465
Khan KM, Forster BB, Robinson J et al. Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two-year prospective study. Br J Sports Med 2003; 37: 149
Alfredson H, Pietila T, Jonsson P et al. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998; 26: 360-366
De Jong S, De Vos DJ et al. One-year follow-up of a randomised controlled trial on added splinting to eccentric exercises in chronic midportion Achilles tendinopathy. Br J Sports Med 2010; 44: 673-677
Van der Plas A, De Jong S et al. A 5-year follow-up study of Alfredson’s heel-drop exercise programme in chronic midportion Achilles tendinopathy. Br J Sports Med 2012:46: 214–218
Khan KM, Forster BB, Robinson J et al. Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two-year prospective study. Br J Sports Med 2003; 37: 149-154
Roos E, Engstrom M, Lagerquist A et al. Clinical improvement after 6 weeks of eccentric exercise in patients with mid-portion Achilles tendinopathy: a randomized trial with 1-year follow-up. Scand J Med Sci Sports 2004; 14: 286-295
De Jonge S, De Vos RJ et al. One-year follow-up of a randomised controlled trial on added splinting to eccentric exercises in chronic midportion Achilles tendinopathy. Br J Sports Med 2010; 44: 673-677
Wang CJ, Huang HY, Pai CH. Shock wave enhances neovasularization at the tendon-bone junction. J Foot Ankle Surg 2002; 41: 16-22
Takahashi N, Ohtori S, Saisu T et al. Second application of low-energy shock waves has a cumulative effect on free nerve endings. Clin Orthop Relat Res 2006; 443: 315-319
Rompe JD, Furia J, Maffulli N. Eccentric loading versus eccentric loading plus shock-wave treatment for midportion achilles tendinopathy: a randomized controlled trial. Am J Sports Med 2009; 37(3): 463-370
Paoloni J, Appleyard R, Nelson J et al. Topical glyceryl trinitrate treatment of chronic noninsertional Achilles tendinopathy. J Bone Joint Surg 2004; 86-A(5): 916-922
Steunebrink M et al. Topical glyceryl trinitrate treatment of chronic patellar tendinopathy: a randomised, double-blind, placebo-controlled clinical trial. Br J Sports Med 2013; 47: 34-39
Alfredson H, Ohberg L. Sclerosing injections to areas of neovascularisation reduce pain in chronic Achilles tendinopathy: a double-blind randomised controlled trial. Knee Surg Sports Traumatol Arthrosc 2005; 13: 338-344
Hoksrud A, Ohberg L, Alfredson H, Bahr R. Ultrasound-guided sclerosis of neovessels in painful chronic patellar tendinopathy: a randomized controlled trial. Am J Sports Med 2006; 34(11): 1738-1746
Tisi PV, Beverley C, Rees A. Injection sclerotherapy for varicose veins. Cochrane Database Syst Rev 2006; 4: CD001732
Willberg L, Sunding K, Ohberg L et al. Sclerosing injections to treat midportion Achilles tendinosis: a randomised controlled study evaluating two different concentrations of Polidocanol. Knee Surg Sports Traumatol Arthrosc 2008 16: 859–864
Sedrakyan A, Treasure T, Elefteriades JA. Effect of aprotinin on clinical outcomes in coronary artery bypass graft surgery: a systematic review and meta-analysis of randomized clinical trials. J Thorac Cardiovasc Surg 2004; 128(3): 442-448
Maffulli N, Spiezia F, Longo UG et al. High volume image guided injections for the management of chronic tendinopathy of the main body of the Achilles tendon. Phys Ther Sport 2012; doi: 10.1016/j.ptsp.2012.07.002. [Epub ahead of print]
Humphrey J, Chan O, Crisp T et al. The short-term effects of high volume image guided injections in resistant non-insertional Achilles tendinopathy. J Sci Med Sport 2010; 13(3): 295-298
Peerbooms JC, Sluimer J, Bruijn DJ et al. Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial: platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. Am J Sports Med 2010; 38: 25
Gosens T, Peerbooms JC, van Laar W et al. Ongoing positive effect of platelet-rich plasma versus corticosteroid injection in lateral epicondylitis: a double-blind randomized controlled trial with 2-year follow-up. Am J Sports Med 2011; 39: 1200
de Jonge S, de Vos RJ, Weir A et al. One-year follow-up of platelet-rich plasma treatment in chronic Achilles tendinopathy: a double-blind randomized placebo-controlled trial. Am J Sports Med 2011; 39: 1623
de Vos RJ, Weir A, van Schie HT et al. Platelet-rich plasma injection for chronic Achilles tendinopathy: randomized controlled trial. JAMA 2010; 303(2): 144-149
de Vos RJ, Weir A, Tol JL et al. No effects of PRP on ultrasonographic tendon structure and neovascularisation in chronic midportion Achilles tendinopathy. Br J Sports Med 2011; 45: 387-392
Shrier I, Matheson GO, Kohl HW 3rd. Achilles tendonitis: are corticosteroid injections useful or harmful? Clin J Sport Med 1996; 6(4): 245-250
Mahler F, Fritschy D. Partial and complete ruptures of the Achilles tendon and local corticosteroid injections. Br J Sports Med 1992; 26(1): 7-14
Jones JG. Achilles tendon rupture following steroid injection. Jones JG. J Bone Joint Surg Am 1985; 67(1): 170
Paavola M, Kannus P, Orava S et al. Surgical treatment for chronic Achilles tendinopathy: a prospective seven month follow up study. Br J Sports Med 2002; 36: 178-182
Testa V, Capasso G, Benazzo F et al. Management of Achilles tendinopathy by ultrasound-guided percutaneous tenotomy. Med Sci Sports Exerc 2002; 34(4): 573-580
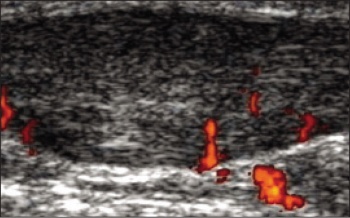 Figure 1. Longitudinal colour Doppler ultrasound of the Achilles tendon showing both hypoechoic regions and areas of neovascularisation(click to enlarge)
Figure 1. Longitudinal colour Doppler ultrasound of the Achilles tendon showing both hypoechoic regions and areas of neovascularisation(click to enlarge)