Physicians should consider cough-induced rib fractures in patients with prolonged cough and localised area chest pain
Dr Ozair Farooq, Senior House Officer, Portiuncula University Hospital, Galway, Dr Muhammad Zeeshan Azhar, Senior Registrar in Emergency Medicine, Portiuncula University Hospital, Galway, Dr Zaid Rana, Senior House Officer, Portiuncula University Hospital, Galway, Dr Kiren Govender, Consultant in Emergency Medicine, Portiuncula University Hospital, Galway and Dr Laura Bandut, Consultant in Emergency Medicine, Portiuncula University Hospital, Galway
A 61-year-old man presented to the emergency department with a two-week history of non-traumatic lower left localised chest pain, which was initially intermittent but in past few days had become severe in intensity associated with temperature. The patient reported that he had had a dry cough for more than one month duration. He had reported no urinary symptoms, abdominal pain, diarrhoea or vomiting. No history of trauma or an old rib fracture was mentioned.
The patient had a routine medical outpatient appointment a month previously where an increasing dry cough complaint was noticed, but no chest pain was documented at that time.
He has background history of left renal stones, hypertension, gout, C-PAP for obstructive sleep apnoea, asthma, type 2 diabetes and right femoral artery stenosis. He had no drug allergies and no previous pulmonary embolism or deep vein thrombosis (DVT).
On examination he was in pain (7/10) tachycardiac (110), tachypnoeic (32), BP 110/70, saturation 91% on room air, and localised tenderness at left lower rib cage postero-laterally associated with fine left basal creptitations and wheeze. Rest systems were unremarkable.
Provisional diagnosis of a lower respiratory tract infection (LRTI), non-traumatic cough-induced rib fracture, pulmonary embolism and left renal colic was made. His Well’s PE score was 1, PERC PE score was 3, and CURB 65 was zero.
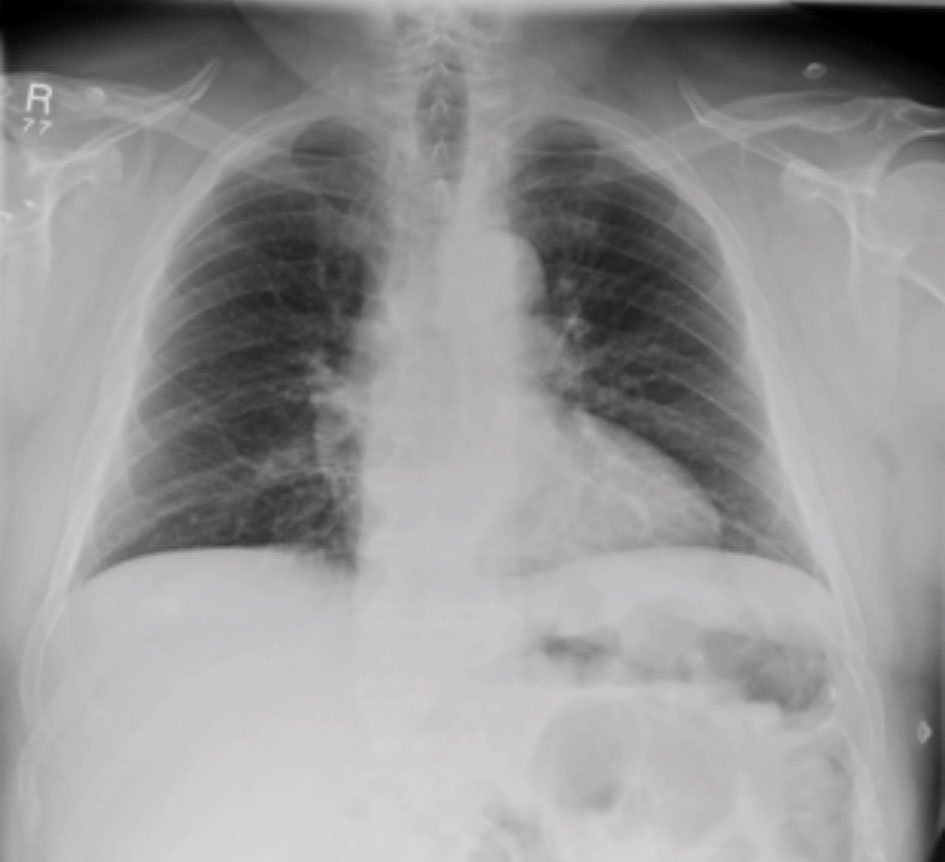
ABG showed type 1 respiratory failure picture with PO2 of 9.40, PCO2 was 4.68 and saturation of 92%, lactate was 2.2. Septic work up including full blood count, liver functions and electrolytes were normal. A postero-anterior chest x-ray (see Figure 1) was performed, reported normal with no rib fracture or pneumothorax. Urine dip analysis showed one plus blood. ECG performed showed sinus tachycardia.
Figure 1. X-ray chest – no evident rib fracture(click to enlarge)
The patient was treated with intravenous fluids, analgesia, nebulisers, antibiotics and steroids and then referred to the medical team with above provisional diagnosis. A CT pulmonary angiography (CTPA) was arranged to exclude above. CTPA showed left 10th rib fracture (see Figure 2), mild atelactic band left lung base and no pulmonary embolism was reported. Renal CT did not show any new stone as cause of left lower rib cage tenderness.
Figure 2. CT image showed left 10th rib fracture, (arrow mark)(click to enlarge)
The patient was then discharged in stable condition on regular analgesia (oral and topical), antibiotics (for element of LRTI) with GP and medical outpatients for further follow up with respiratory team. It was proposed that the patient’s chronic lung issue may contribute towards his cough-induced rib fracture.
Discussion
Non-resolving cough is a presentation that forces patients to seek medical attention.1 It resolves without any significant issue but sometimes can result in complex issues such as cough-induced non-traumatic rib fracture, pneumothorax, haemothorax, flail chest, lung contusion2,3 or sometimes more serious issues such as diaphragmatic rupture, possibly followed by serious complications. Non-resolving pain is one the most common symptoms that cause a patient to present.
There are a few theories that propose mechanisms leading to a cough-induced rib fracture. The first of these is the repeated coughing force that can cause a rib to fracture at one point. Secondly, strong opposing muscles such as the serratus anterior and external oblique can exert opposite forces on the ribs that can lead to rib fractures in patients with chronic cough. Acute or chronic lung disease may also be a contributing factor.
Cough-induced rib fracture was first reported by Gooch in 1773 and then by Monteggia in 1802. Castellan in 1861 reported sneezing as a cause of rib fracture. Later, in 1843 Graves and then in 1923 Webb et al4 mention cough as one of the mechanisms to induce rib fractures. Since then different causes of cough-induced rib fractures have been reported in the literature, including a few cases in pregnancy and psychogenic cough-induced rib fractures.
Predicting and diagnosing cough-induced rib fractures can be challenging. Chest radiographs are less sensitive than CT scan in diagnosing rib fractures, ie. 60% and 100% respectively.5,6 More dedicated chest radiographs may be more informative in detecting rib fractures.
Hanak et al2 in 2005 carried out a retrospective study (54 patients), which described six to nine ribs affected with the sixth rib being the most commonly affected in two groups. Half of the cohort (27 patients) had a single rib fracture and the remaining half had multiple rib fractures noted. The majority of patients had a CT scan of chest.
Sano et al7 (14 patients) in 2015 mentioned the 10th rib as the most common rib to be affected as compared to above study. In his study, nine patients had single and five had multiple fractures. Women were most often affected in both studies especially those who had osteopenic bones.2,7
Case reports such as a 22-year-old healthy man,8 72-year-old woman with diabetes and 53-year-old man9 on enalapril, described as cough-induced rib fractures.
It is observed from literature that multidimensional dedicated chest x-rays can decrease the use of CT in diagnosing rib fractures so that CT can be limited to more complex cases. Treatment goals are mainly pain relief as per local guidelines, other supportive measures and regular follow up.7,10,11
In conclusion, physicians should consider cough-induced rib fractures in patients with prolonged cough and localised area chest pain, however, good history and clinical examination is the best tool in predicting above. Chronic lung disease may be a contributing factor. Investigations depend on a patient’s co-morbid factors and initial presentation.
References
Madison JM, Iris RS. Cough a worldwide problem. Otolarygol Clin North Am 2010; 46:1-13
Roberge RJ, Morgenstern MJ, Osborn H. Cough fracture the ribs. Am J Emerg Med; 1984: 2: 513-517
Webb et el. Rib fractured by coughing. JAMA 1923; 81:25-29
Connolly LP, Connolly SA. Rib stress fractures. Clin Nucl Med 2004 29: 614-616
De Maesenerr M, De Mey J, Lenchik L, Everaert H, Osteaux M, Helical CT of rib lesions, a pattern-based approach. Am J Roentgenol 2004: 182: 173-9
Sano A, Tashiro K, Fukuda T. Cough-induced rib fractures. Asian Cardiovasc Thorac Ann 2015: 23: 958-60
Yeh CF, Su SC. Cough-induced rib fracture in a young healthy man. J Formos Med Assoc 2012 Mar;111(3): 179-80
Trovato DA, Sousa JE, Bruetman JE, Finn BC, Young P. Symmetrical rib fractures associated with chronic cough. Report of one case. Rev Med Chil 2018 Mar; 146(3): 391-393.
Achilleos A. Evidence based evaluation and management of chronic cough. Med Clin North Am 2016; 100:1033-45
Kawahar H, Baba H, Wada M, Azuchi M, Ando M, Imura S. Multiple rib fractures associated with severe coughing – a case report. Int Orthop 1997: 21: 279-81
 Figure 1. X-ray chest – no evident rib fracture(click to enlarge)
Figure 1. X-ray chest – no evident rib fracture(click to enlarge)