CANCER
CHILD HEALTH
Dual diagnosis of paraganglioma with acute liver abscess
An interesting case of dual diagnosis of an abdominal paraganglioma coincidental to an acute liver abscess in a 15-year-old boy
October 8, 2019
-
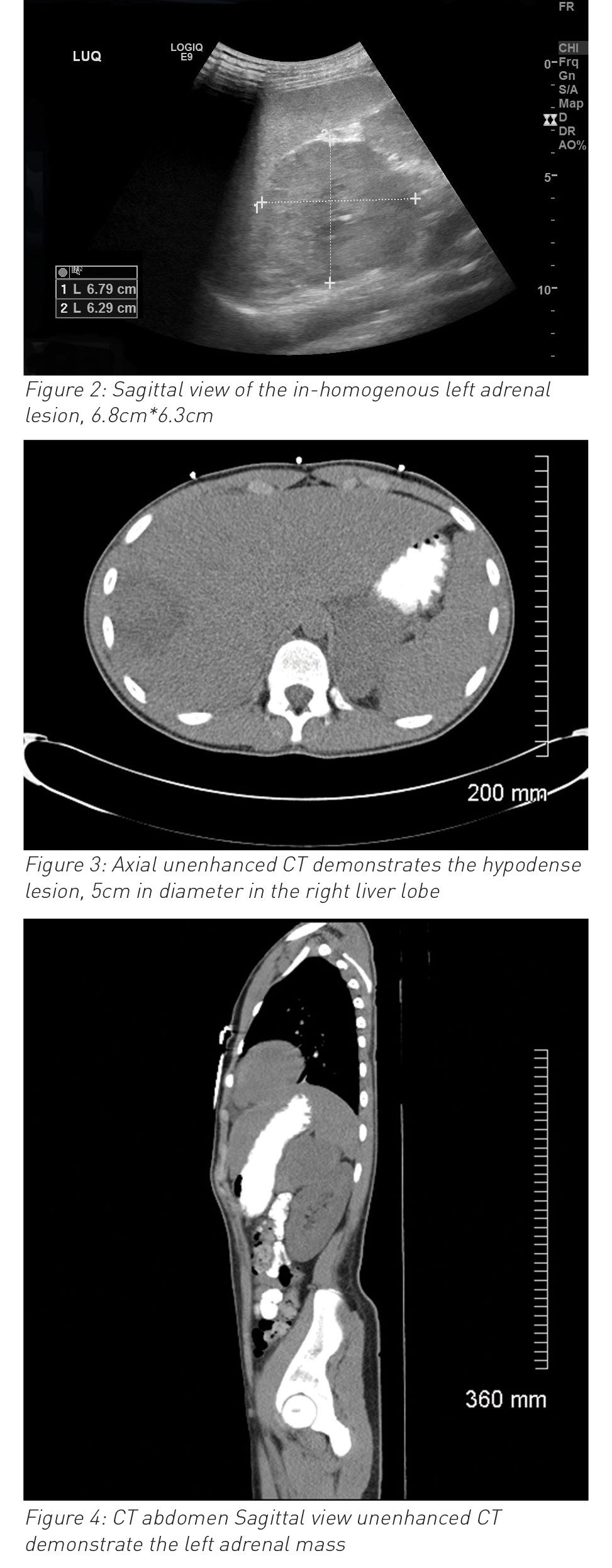
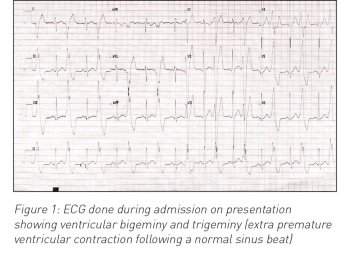
A 15-year-old boy presented with a short history of right upper quadrant abdominal pain, fever and right shoulder tip pain with high inflammatory markers. Within 24 hours he developed ventricular bigeminy and trigeminy. An abdominal ultrasound showed a liver abscess and unexpected findings of left side suprarenal mass. Subsequent MRI abdomen, MIBG scan and histopathology confirmed the diagnosis of an abdominal paraganglioma coincidental to the acute presentation of a liver abscess, likely from preceding trauma.
On presentation to the emergency department, this previously healthy adolescent had a one-week history of being unwell, vomiting, arthralgia, myalgia and poor appetite which was preceded by coryzal illness for few days. The following day he started complaining of abdominal pain and right-sided shoulder tip pain and low-grade pyrexia. He had a history of a significant fall from a petrol go-kart while racing two weeks earlier with bruising to his back and abdomen.
On clinical examination, he was unwell, pale, tachycardia (H.R: 130/min), pain score: 8/10, positive Murphy sign. Blood investigation showed high inflammatory markers with white blood cells of 36.4 x 109/L and C-reactive protein of 252mg/L) normal liver functions test and serum amylase. The working diagnosis of acute cholecystitis established and was commenced in intravenous antibiotics (initially on co-amoxiclav and then switched to cefotaxime) and further radiological investigations were requested.
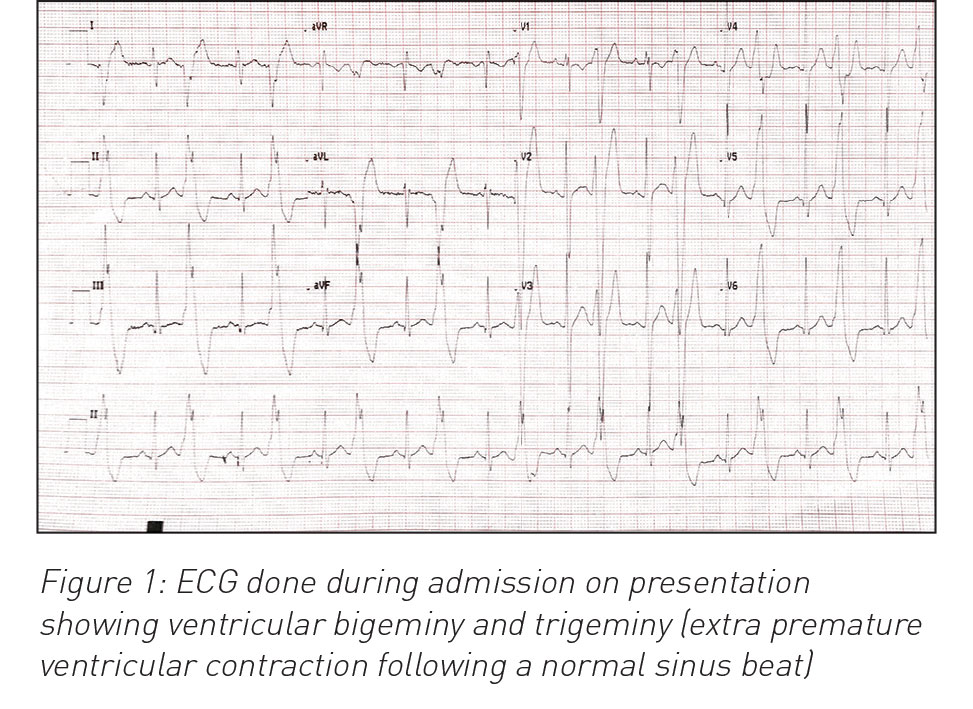
During his hospital stay it was noted that he had an episode of high blood pressure (140/90mmHg) and developed ventricular bigeminy and trigeminy (see ECG in Figure 1). Chest x-ray and echocardiography were normal. Ultrasound and MRI abdomen reported left side suprarenal mass (8cm) and associated liver abscess (7cm x 7cm x 7cm). Urine catecholamines were normal. Liver abscess (abscess grew Streptococcus intermedia) was treated with drainage and with six weeks antibiotics. Paraganglioma was surgically resected successfully three months after initial diagnosis and full evaluation (genetic testing and exclusion of MEN syndrome and von-Hipple-Lindau syndrome). Ventricular bigeminy resolved completely and final diagnosis of non-secreting pheochromocytoma and coincidental liver abscess (likely due to trauma in the past). He was discharged home after full recovery. He is being followed up with regular abdominal imaging; to date, no concerns have been reported.
 (click to enlarge)
(click to enlarge)