Errors in written prescriptions in the drug kardex in Irish ICU
A retrospective audit of 100 prescriptions in an Irish hospital setting was done to find out errors in written prescription in drug kardex in ICU. In this article the hospital team discuss the findings
Dr Anwar Ul Haq, Consultant Anaesthetist, Midland Regional Hospital, Offaly
Medication errors, defined as any error in the prescribing, dispensing or administration of a drug, whether there are adverse consequences or not, are the single most preventable cause of patient injury.1-3 A retrospective audit was done to find out errors in written prescription in the drug kardex in the intensive care unit (ICU). Data on 100 prescriptions of 10 aspects were evaluated percentage-wise. About 43% errors were found overall in all aspects, which is approximately the same in various studies done in ICUs.
Medical Council number and bleep number of the prescriber and the generic name of the drug were the three aspects where the highest percentage of errors were found. This is a significant number in this small audit. Certain protocols should be set first to reduce these errors and a re-audit should be done in the near future.
Introduction
These types of medication errors can occur at any stage in the drug-use process from prescription to administration to the patient. A report by the Institute of Medicine (IOM) estimated that errors in medical management cause between 44,000 and 98,000 deaths each year in US hospitals.4 The rate of serious medication error is approximately 7% in the US.3 Reports from the Medical Defence Union and the Medical Protection Society revealed that 25% and 19%, respectively, of legal claims against general practitioners (GPs) related to medication errors.5,6
In 2004, Ridley SA et al described prescription errors in 24 UK ICUs for a period of four weeks. This study followed four categories:
Not writing in the order according to the BNF recommendations
An ambiguous medication order
Non-standard nomenclature
Writing legibility, which accounted for 47.9% of all errors.7
Although prescription rates (and error rates) in critical care appear higher than elsewhere in this hospital, the number of potentially serious errors is similar to other areas of high-risk practice. This ICU audit is part of the overall audit carried out by different departments of the hospital.
Aims and objectives
Aims of the retrospective audit are to:
Improve quality of written inpatient drug kardex in ICU
Suggest interventions designed to address identified deficiencies
Prevent errors in delivery of medications and adverse drug events.
In light of this audit guidelines will be implemented regarding improving standard of quality of prescriptions.
Methods
It is a retrospective ICU audit carried out in prescribed form and part of the mega-audit carried out by various departments of the hospital, which were permitted by the hospital’s ethical committee. Only 100 prescriptions were evaluated on the following 10 aspects of the drug kardex.
Date of prescription
Allergies
Drug’s generic name
Patient’s ID
Dose
Route of administration
Legible signature
Bleep number of prescriber
Legibility (readable)
Medical Council number and data was analysed on percentage bases.
Results
Data were collected for 100 prescriptions in intensive care patients. One person evaluated these data based on the aforementioned 10 aspects. Their evaluation of numbers and percentages are shown in Table 1.
Figure 1 shows a total of 47% errors in prescription that occurred overall in all aspects of the analysis in the drug kardex.
Table 1: Aspects of prescription written on drug kardex(click to enlarge)
Figure 1: Number of prescriptions: total 100% of all aspects(click to enlarge)
Discussion
The Irish Medication Safety Network (IMSN) mentioned in 2008 that medication errors and adverse drug reactions occur frequently, leading to a high burden of patient harm in the hospital setting.
Many Irish hospitals have established medication safety initiatives, designed to encourage reporting and learning to improve medication use processes and therefore patient safety.
Eight Irish hospitals or hospital networks provided data from voluntary medication safety incidents and ‘near miss’ reporting programmes for pooled analysis of events occurring between January 1, 2006, and June 30, 2007.8
There were 6,179 reports received in total (mean 772 per hospital; range 96-1,855). Ninety-five per cent of reports did not involve patient harm. Forty-seven per cent of reports related to the prescribing stage of the medication-use process, while 40% related to the administration stage and 9% to the pharmacy dispensing stage. These data are published to:
Increase awareness of this key patient safety issue
Share learning from these incidents and near misses
Encourage a more open patient safety culture.8
The IMSN report showed that 47% of errors occurred in prescription stage, which is similar to this audit’s results, however, evaluation was different in different aspects of both studies and settings.
Rediley SA et al (2004)6 evaluated prescription errors in 24 ICUs in the UK over 18 months. In the four categories, written prescriptions evaluation accounted for 47.9% of all errors. As in the aforementioned study, it was quite comprehensive on:
Number of ICUs
Number of patients
Various aspects of analysis.
However, in the Irish hospital audit, the percentage amount of ICU errors were evaluated across the 10 aspects of the drug kardex and still prescription errors were all there.
In addition to the above study,7 over the four-week period of the Rediley study, 21,589 new prescriptions (or 15.3 new prescriptions per patient) were written:
Eighty-five per cent (18,448 prescriptions) were error-free
3,141 (15%) prescriptions had one or more errors (2.2 erroneous prescriptions per patient, or 145.5 erroneous prescriptions per 1,000 new prescriptions).
The five most common incorrect prescriptions in the Rediley study were for:
Potassium chloride (10.2% errors)
Heparin (5.3%)
Magnesium sulphate (5.2%)
Paracetamol (3.2%)
Propofol (3.1%).
Most of the errors were minor or would have had no adverse effects, but 618 (19.6%) errors were considered significant, serious or potentially life-threatening.
Such detailed analysis was not undertaken in the Irish hospital audit, however, in future, more detailed audits should be designed. Certain guidelines or protocols should be developed so as to reduce the percentage of errors found in this audit, in future audits.
Another important aspect to be highlighted from the results of the audit is that none of the prescribers wrote their Medical Council number in the drug kardex. Either that or there was no box available for the Medical Council number, even though section 59.1 of the guidelines of the conduct and the ethics of registered medical practitioners in 20099 clearly mentions that the prescriptions issued must be legible, dated and signed and must state the doctor’s Medical Council registration number. This was significantly lacking in the results.
Recommendations
Even though this was a small audit of a multidisciplinary team who handled the ICU in a county general hospital, the percentage of errors was quite significant.
However, certain recommendations are designed to reduce or eradicate the errors and they involve everyone: consultants, senior and junior doctors, Sister in charge of ICU/CNM/medical students/nursing students etc.
The audit register should be kept for a prospective re-audit or for educational strategies, eg. feedback of audit results, education sessions for doctors and nurses on prescribing and medication errors.
There should be a series of audits to review progressive improvements like a computerised prescription system in the ICU. There should also be system changes such as:
Modifications to medication charts
Development of hospital-wide prescribing standards and an alert notification system
Zero tolerance days
Legibility of prescription assurance
Legible signature assurance
Proper bleep number
Medical Council number
Drugs should be written in capital letters
Dosages should be accurate
Route of administration should ensure that errors are avoided
Incidents
Near misses
Potential danger.
References
Leape LL. Preventing adverse drug events. Am J Health Syst Pharm 1995; 52: 379-382
La Pietra L, Calligaris L, Molendini L. Medical errors and clinical risk management: state of the art. Acta Otorhinolaryngol Ital 2005; 25(6): 339-346
Weingart SN, Wilson R, Gibberd RW, Harrison B. Epidemiology of medical errors. BMJ 2000; 320: 774-777
Becher EC, Chassin MR. Improving quality, minimizing error: making it happen. N Engl J Med 2000; 342: 1123-1125
Silk N. An analysis of 1000 consecutive general practice negligence claims. The MDU Risk Management 1996; 1-8
MPS Casebook 1999; 9-10
Ridley SA, Booth SA, Thompson CA. Prescription errors in UK critical care units. Anaesthesia 2004 ; 59 : 1193–1200
Kirke C, Irish Medical Safety Network. Medical safety in hospitals. Ir Med J 2009; 102 (10): 339-341
Guide to Professional Conduct and Ethics for Registered Medical Practitioners. Medical Council: 2009 (Sec 59.1)
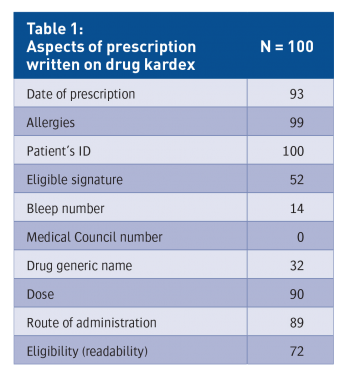 Table 1: Aspects of prescription written on drug kardex(click to enlarge)
Table 1: Aspects of prescription written on drug kardex(click to enlarge)
