Intra-articular lidocaine injection for shoulder dislocation
A case of ultrasound-guided intra-articular lidocaine (IAL) injection which proved to be an effective technique in ED management of a shoulder dislocation in a 98‑year‑old woman
Dr Muhammad Zeeshan Azhar, Senior Registrar in Emergency Medicine, Portiuncula University Hospital, Galway, Dr Kiren Govender, Consultant in Emergency Medicine, Portiuncula University Hospital, Galway, Dr Laura Bandut, Consultant in Emergency Medicine, Portiuncula University Hospital, Galway, Dr Waqas Mahmood, Senior Registrar in Emergency Medicine, Portiuncula University Hospital, Ballinasloe, Dr Faisal Dablouk, Registrar in Emergency Medicine, Portiuncula University Hospital, Ballinasloe and Dr Ijaz Ahmad, Registrar in Emergency Medicine, Portiuncula University Hospital, Ballinasloe
We present a case of a 98-year-old female nursing home patient who presented to the emergency department with acute right shoulder pain. The patient was transferred to the emergency department from the nursing home after she had complained of acute shoulder pain while being lifted from the toilet seat. Later in the ED the same patient was not able to lift her arm and reported moderate to severe pain while attempting to move her arm.
She has a background history of dementia, Alzheimer’s disease, ischaemic heart disease, supraventricular tachycardia, hypertension, old cerebrovascular atrial fibrillation (not on anticoagulant), hypercholesterolaemia and is fully dependent on a puréed diet.
On examination she was lying in bed, moaning in severe pain in her right arm while having her shoulder examined. Loss of right shoulder contour was noted and neurological examination was normal. No other abnormality was noted and the rest of the symptoms were unremarkable. The patient did not have denatures, her vitals were within normal limits and her ASA was about four.
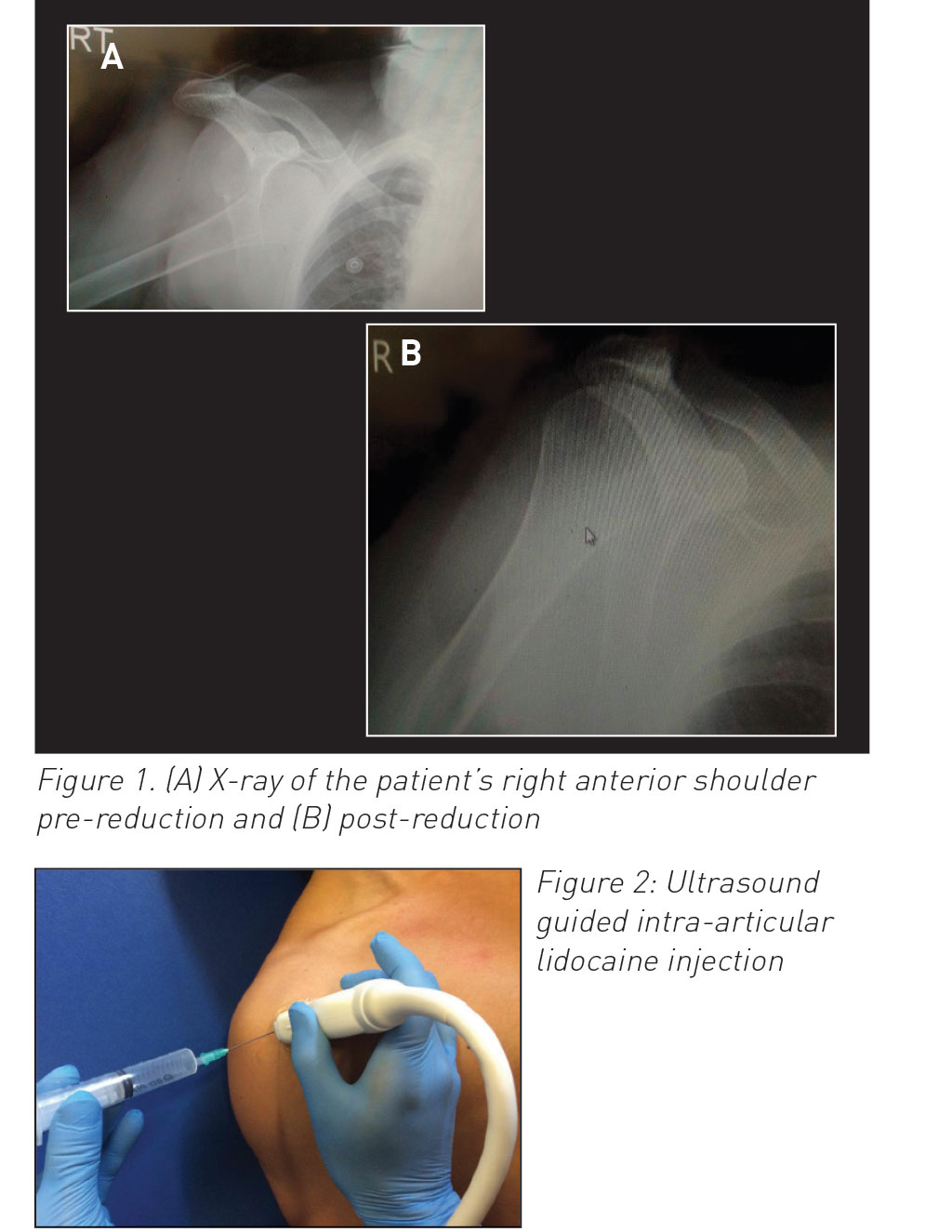
A provisional clinical diagnosis of right anterior shoulder dislocation was made. Ultrasound confirmed the diagnosis and an x-ray of the right shoulder was arranged to confirm the right anterior shoulder dislocation with no evident fracture (see Figure 1a).
The patient was not able to use phenthrox, entonox (due to dementia and lack of facial support) and sedation in the ED was not considered safe due to possible airway issues, as per her ASA score, as well as no facial support and other co-morbid factors.
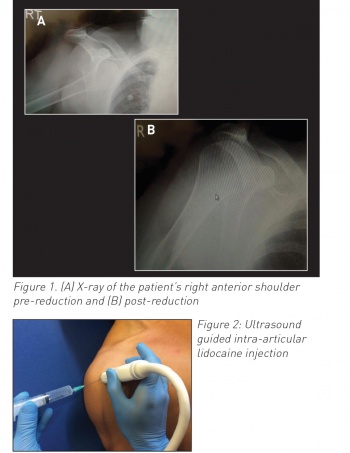
We then decided to carry out an ultrasound guided intra-articular lidocaine (IAL) injection under full aseptic technique to reduce the patient’s dislocated shoulder and safely discharge her back to the nursing home.
Under full aseptic technique, ultrasound guidance and on cardiac monitor, the patient received 10ml of 1% IAL (see Figure 2). Subcutaneous lidocaine was given before this procedure to minimise the pain of the injection. We then waited 15 minutes for the lidocaine for shoulder reduction to take full effect. After 15 minutes her right shoulder was reduced successfully with modified Kocher’s technique on the first attempt. The procedure was pain free and easily performed. Ultrasound was used again to confirm her shoulder reduction. Neurological examination post reduction was normal (different techniques present for ultrasound guided IAL depending on physician experience). A shoulder sling was then applied. The patient had no intra or post-procedure complications.
The patient then underwent x-ray post-reduction, which confirmed that her shoulder was reduced successfully (see Figure 1b).
(click to enlarge)
The patient remained vitally stable and pain free since receiving the intra-articular lidocaine injection. A fracture clinic appointment with orthopaedics was made for her.
The patient was observed for one hour post-IAL injection and no complications were noted. She was then safely discharged back to the nursing home, with advice on analgesia if the patient complains of pain and to follow up in the fracture clinic. The follow up call was made after one week and the patient had no complication noted post the procedure in ED.
Discussion
Joint dislocations commonly present to the ED and shoulder joints alone account for 50% of all major joint dislocations.1 Anterior shoulder dislocations account for 95-97% and posterior dislocations account for 3%. Shoulder dislocations routinely present with decreased range of movement, loss of shoulder contour, and severe pain.
The role of the emergency physician is to diagnose the type of dislocation using x-rays such as AP, axillary or Y views,2,3 manage by reduction with suitable techniques4 and procedures to minimise risk of possible complications. Eliminating pain is one of the goals both pre and post reduction procedures.
An intra-articular lidocaine injection (IAL) is one of the alternatives to conventional sedation/analgesia used in the reduction of shoulder dislocations.5 Many studies advocated the IAL as similar to intravenous sedation (IVS) in providing pain relief during shoulder relocations.6,7
However, few reported in favour of IVS compared to IAL for same.8 IVS is associated with complications such as respiratory and central nervous system depression, whereas few complications are reported regarding the use of IAL in the literature.9,10
Multiple prospective randomised controlled trails mentioned that IAL has more favourable results in terms of cost, safety and effectiveness, low manpower input, time spent in the emergency department and fewest complications as compared to IVS for similar reasons.11,12 Orlinsky et al13 and Kosnik et al6 reported IVS as clinically significant but that IAL can be used as an alternative where it is necessary to avoid complications of sedation. However, Lippitt et al14 and Suder et al showed 100% and 97% respectively for IAL in comparison to IVS where it was 75% and 94% for both studies. Miller et al7 also favours IAL for cost, safety and effectiveness. Cunningham15 suspected IAL as a possible cause of septic arthritis, however it is not supported by other literature and the majority of the studies. The majority of studies, such as Kosnik et al,6 Suder et al,5 Lippit et al15 and Matthews and Roberts16 did not show any complications with IAL, whereas they documented complications with IVS in their studies as 5%, 11%, 12% and 30% respectively.
A recent study, carried out in Iran by Kashani et al17 in 2016 revealed that the use of IAL is effective, safe and time-saving, with fewer complications. IAL can be used in cases where IVS is not desired. Therefore, nearly all of the studies recommended IAL as a possible alternative to IVS with few observations, with the exception of Hames et al18 who mentioned a long stay in the emergency department as compared to the other RCTs mentioned above.
However, on the other hand some studies revealed that IVS has some favourable results due to patient satisfaction in relation to muscle relaxation, pain reduction and a greater success rate compared to IAL.6,7,8,9,10,11,12,13 In some studies, physicians felt more comfortable with IVS rather than IAL due to these factors.
In normal emergency practice, IVS is one of the most common methods used during acute shoulder dislocation reductions. The ideal shoulder dislocation reduction should be less painful and without complications.
However, it is always challenging to introduce new techniques in ongoing practices.
In conclusion, IAL injection could be more beneficial in terms of early discharge, cost effectiveness, staffing and monitoring. It also has the fewest complications. It could also be an excellent alternative where IVS is contraindicated or carries high risk. The addition of ultrasound-guided IAL shoulder dislocation/relocation will be beneficial in eliminating its limitations and producing better and more accurate results. IAL would benefit the ED where bed availability is always a concern.
Proper patient education and emergency physician training for ultrasound-guided IAL can introduce a possible alternative when conventional intravenous sedation/analgesia carries high risk or other techniques are exhausted.
References
Zacchilli MA, Owens BD. Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Joint Surg Am 2010 Mar; 92(3):542-9 doi: 10.2106/JBJS.I.00450
Khiami F, Gérometta A, Loriaut P. Management of recent first-time anterior shoulder dislocations. Orthop Traumatol Surg Res 2015 Feb; 101(1 Suppl):S51-7
Kane P, Bifano SM, Dodson CC, Freedman KB. Approach to the treatment of primary anterior shoulder dislocation: A review. Phys Sportsmed 2015 Feb; 43 (1):54-64
Riebel GD, McCabe JB. Anterior shoulder dislocations: a review of reduction techniques. Am J Emerg Med 1991; 9:180-8
Suder PA, Mikkelsen JB, Hougaard K et al. Reduction of traumatic, primary anterior shoulder dislocations with local anaesthesia. J Shoulder Elbow Surgery 1994; 3(5):288-94
Kosnik J, Shamsa F, Raphael E et al. Anaesthetic methods for reduction of acute shoulder dislocations: a prospective randomized study comparing intra-articular lidocaine with intravenous analgesia and sedation. Am J Emerg Med 1999; 17(6):556-70
Miller SL et al. Comparison of intra-articular lidocaine and intravenous sedation for reduction of shoulder dislocations, a randomized prospective trial. J Bones Joint Surg Am 2002; 84:2135-9
Glesson AP, Graham CA, Mayer AD. Intra-articular versus Entonox for reduction of acute anterior shoulder dislocation. Injury 1999; 15:804
Greenblant DJ, Koch WJ. Adverse reaction of diazepam. Am J Med Sci 1973; 266: 261-6
Gross JB, Long WB. Nasal oxygen alleviates hypoemia in colonoscopy patients sedated with midazolam and mepridine. Gastrointest, eEndosc 1990; 36:26-9
Rookwood CA, Freen DP, Bucholz RW. Fractures in adults. 3rd Ed Philadelphia JB Lippincott, 1991
Dahl MR, Dasta JF, Zeuler W et al. Lidocaine local anaesthesia for arthroscopic knee surgery. Anaesth Analg 1990; 71:670-4
Orlinsky M, Shon S , Chiang C et al. Comparative study of intra-articular lidocaine and intravenous diazepam for shoulder dislocation. J Emerg Med 2002; 22:241-5
Lippitt SB, Kennedy JP, Thompson TR. Intraarticular lidocaine versus intravenous analgesia in the reduction of dislocated shoulders. Orthop Trans 1991; 15:804
Cunningham NJ. Techniques for reduction of anterioinferior shoulder dislocation. Emerg Med Australasia 2005; 17:463-71
Matthews DE, Roberts T. Intraarticular lidocaine vs IV analgesia for the reduction of acute anterior shoulder dislocation. University of Mississippi. Am J Sports Med 1995; 23(1):5458
Kashani P, Asayesh Zarchi F, Hatamabadi HR et al. Intra-articular lidocaine versus intravenous sedation and analgesia for reduction of anterior shoulder dislocation. Turk J Emerg Med 2016; 16(2):60-4
Hames H, McLeod S, Millard W. Intra-articular lidocaine versus intravenous sedation for the reduction of anterior shoulder dislocation in the emergency department. CJEM 2011 Nov; 13(6):378-83
 (click to enlarge)
(click to enlarge)