Macroprolactinoma with chronic headache and lost libido
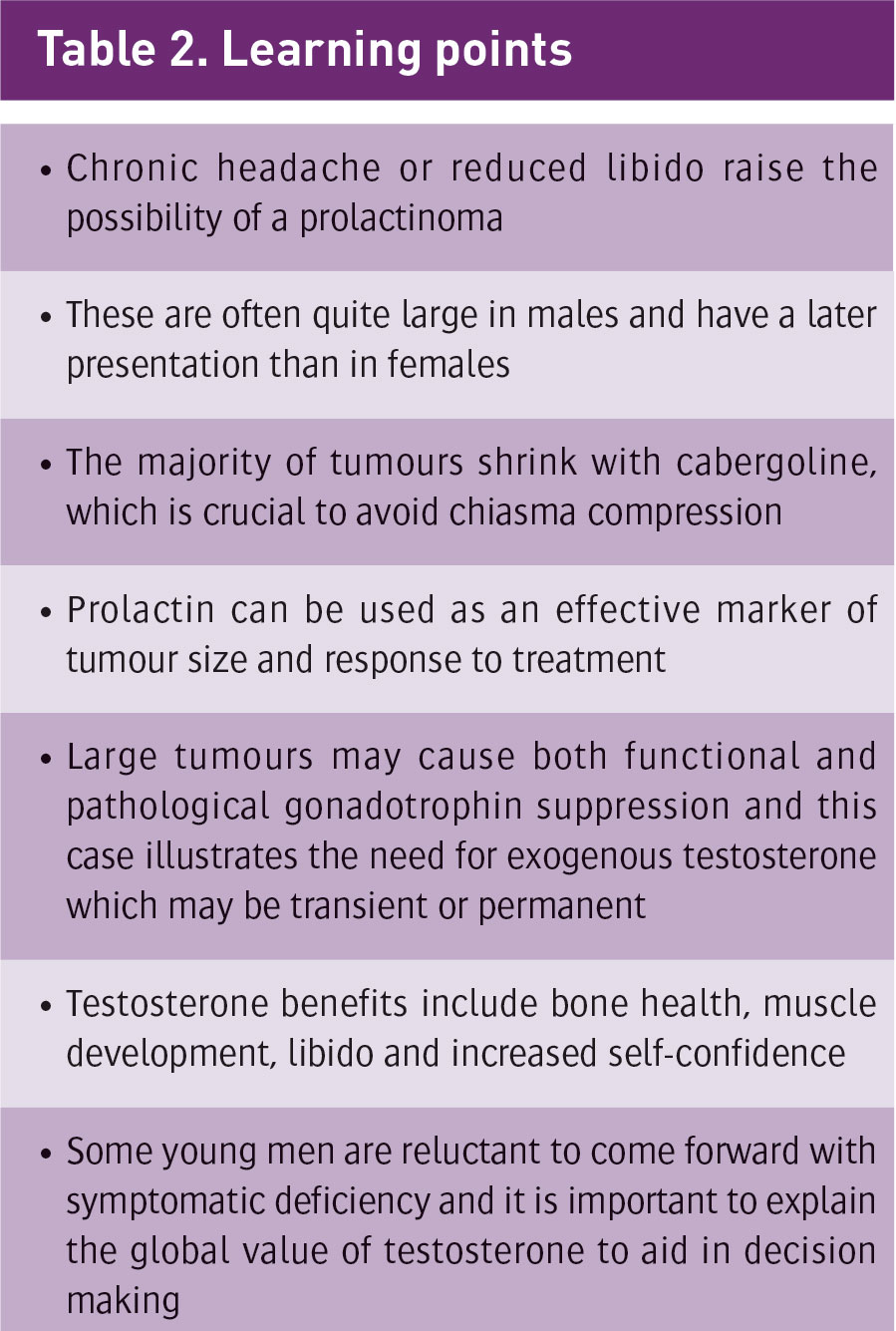
A case of macroprolactinoma presenting with chronic headache and reduced libido
Dr Bart Daly, Senior House Officer, Department of Endocrinology, University Hospital Limerick, Limerick and Dr James O'Hare, Consultant Endocrinologist, Department of Endocrinology, University Hospital Limerick, Limerick
A patient with a macroprolactinoma had good tumour shrinkage with high-dose cabergoline. However, testosterone levels and libido did not improve until intramuscular Sustanon rather than transdermal testosterone was employed.
Case report
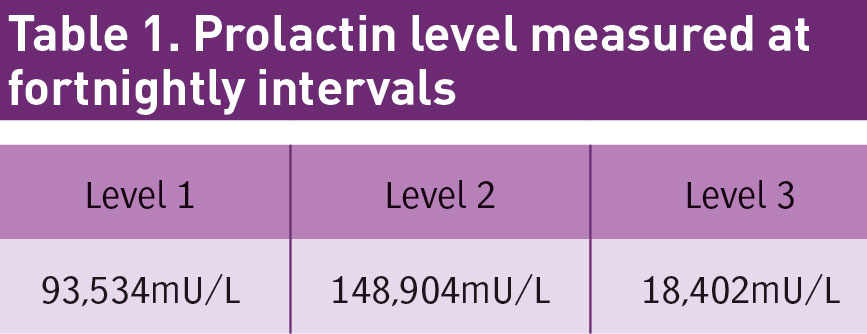
A 32-year-old male presented with a six-month duration of chronic headache and low libido. CT showed a pituitary lesion, MRI confirmed a 2.6 x 2.8cm macro-adenoma with possible impingement on the optic chiasm. Prolactin levels were grossly elevated at 93,000mU/L (53-360mU/L). Testosterone was low at 0.9mmol/L (9-34.7mmol/L) and normal levels of FSH and LH.
Background medical history was significant for cryptorchidism as a child with failure of one testicle to develop and also included sarcoidosis and sub-clinical hypothyroidism. He reported chronically low libido and infrequent shaving, less than once weekly, but no history of galactorrhoea or erectile dysfunction.
Physical examination showed scanty facial hair, mild gynaecomastia, moderate obesity, reduced pubic hair, one underdeveloped testicle and one normal testicle. Visual Fields were intact on formal field testing.
He was commenced on cabergoline, which was built up to 1mg twice weekly. Testosterone replacement was delayed pending control of the prolactin.
(click to enlarge)
On review, headache had improved and prolactin had fallen to 8,671mU/L. Cabergoline was increased to 2mg twice weekly. The patient was clinically well, tolerating treatment well with no fatigue and normal activity levels. Formal visual field testing again showed no deficit.
Repeat MRI brain had shown a 17 x 23mm adenoma much reduced in overall size in the three months since treatment commencement and prolactin fell to 3,721mU/L.
Testosterone level remained low at 2.3mmol/L and the patient noted no improvement in libido, muscle development or energy levels, despite reported compliance with Tostran transdermal gel. He was switched to Sustanon 250mg intramuscular injection every three weeks initially, with maintenance dosing every 12 weeks if a response was shown. This is a blend of four different testosterone compounds with different half lives with the intention of providing a steady state of plasma testosterone.1
At three months, libido improved and the patient had no visual field symptoms. Prolactin was now 2,777mU/L and testosterone level was now 20.4mmol/L, which is within normal range. The patient reported positive feeling towards treatment effect, and eventually started having normal sexual function.
(click to enlarge)
Discussion
There are many causes of transient and long-term elevations of prolactin. Tumours of the pituitary are the rarest but most important.
Transient prolactin elevation can occur with acute stress, seizure, recent sexual activity and breast massage. An important and overlooked cause of elevated prolactin is due to the inert macromolecular form of prolactin called macroprolactin or ‘big’ prolactin.
The endocrine lab should screen for this and alert practitioners if present. A definitive separation of true from big prolactin is possible at specialised laboratories. Once the true prolactin level is normal, no action is required in ‘big’ prolactin measurement.2
Common medications causing increased prolactin levels include dopamine D2 receptor antagonists, including antipsychotic drugs such as risperidone, phenothiazines and haloperidol, as well as the gastric motility drugs metoclopramide and domperidone. Serum prolactin concentrations increase within hours after acute administration of these drugs and return to normal within two to four days after cessation of chronic therapy.3
Renal or hepatic function should be assessed as prolactin clearance can be reduced in failure. Primary hypothyroidism can cause hyperprolactinaemia and amenorrhoea through TRH stimulation and reverses with thyroxine replacement.
If these tests return without diagnosis brain imaging should be considered with MRI, with contrast being the modality of choice.
Dopamine agonists are the cornerstone of treatment for patients diagnosed with prolactinoma.4 Although all dopamine agonists lower prolactin levels, in a double-blind, randomised trial involving 459 women, cabergoline had fewer side effects and prolactin levels normalised in 83% of the patients treated with cabergoline versus 59% of those treated with bromocryptine.5,6
A patient with minimal residual tumour volume and normalised prolactin levels for at least two years may be observed off medication. However, given the high rate of recurrence, ongoing monitoring on a six monthly to yearly basis is advisable.6
References
British National Formulary (BNF) edition 69. Joint formulary committee, March 2015
Yoshida Y et al. A kinetic study on serum prolactin concentration in the thyrotropin-releasing hormone test. Kaku Igaku 1991; 28(6): 585-90 (Article in Japanese)
Snyder P. Causes of hyperprolactinaemia. www.UpToDate.com
The pituitary society. www.pituitary.org.uk; prolactinomas
Webster J et al. A comparison of cabergoline and bromocriptine in the treatment of hyperprolactinemic amenorrhea. N Engl J Med 1994; 331: 904-909
Klibanski A. Prolactinomas. N Engl J Med 2010; 362:1219-1226
 (click to enlarge)
(click to enlarge)