The clinical, biochemical and histological features of giant-cell arteritis
Dr Claire Kennedy, Specialist Registrar, Cork University Hospital, Cork, Dr Sinead Harney, Consultant Rheumatologist, Cork University Hospital, Cork and Dr Bryan O'Sullivan, Specialist Registrar, Cork University Hospital, Cork
Giant-cell arteritis (GCA) is a medium-to-large vessel vasculitis. It has a predilection for the cranial branches of arteries arising from the aortic arch, but has the potential for systemic involvement. Diagnosis is based on a variety of clinical, biochemical and histological features as outlined by the American College of Rheumatology (ACR) in 1990 (see Table 1).1 The presence of three of the five criteria has a sensitivity of 93.5% and a specificity of 91.2%1 for the diagnosis. The approach to GCA is evolving with the advent of increasingly sophisticated techniques. In line with this, the European League Against Rheumatism (EULAR) published recommendations in 2008 based on all available evidence and expert consensus.2
Table 1: ACR criteria for diagnosis of GCA(click to enlarge)
Non-invasive diagnosis
Since the introduction of multi-modality vascular imaging, there has been an interest in non-invasive diagnostic techniques. There are several characteristic ultrasonographic features including the hypoechoic ‘halo’ sign. Meta-analysis suggests that ultrasonography has high diagnostic yield.3 It is, by definition, user-dependent, and so its strength and reproducibility as a diagnostic tool must be evaluated in multi-centre trials prior to general use.
The role of magnetic resonance angiography (MRA) has not been clarified although it has a potential role in guiding temporal artery biopsies and assessing large vessel involvement.4 Positron emission tomography (PET) is also in its early stages of evaluation as a diagnostic modality.5,6
Invasive diagnosis
Temporal artery biopsy remains the gold standard diagnostic technique. Although recommended in all possible GCA cases,2 it is unlikely to help in cases that do not meet the ACR criteria for diagnosis.7 In most published series, about one-third of temporal artery biopsies yield positive results.7 Therefore, it is recommended that a unilateral sample at least one centimetre in length be taken.2
Treatment
It is vital that the biopsy does not delay treatment.8,9 Due to the possibility of a false negative result, and the risk of irreversible ocular damage, treatment should begin immediately when there is strong clinical suspicion of GCA.11
Glucocorticoid therapy
Early, intensive high-dose steroid therapy is the mainstay of treatment in GCA.12 Intravenous methylprednisolone may benefit patients presenting with visual symptoms, preventing progression to irreversible visual loss.10,13 The optimal dose of glucocorticoids for initial treatment of GCA is uncertain. An initial dose of prednisolone 1mg/kg/day (maximum 60mg/day) is almost always used.13
Once the disease has been controlled adequately, tapering of glucocorticoid should begin. This usually starts two to four weeks after the initiation of prednisolone. A moderate dose of steroid such as 10-15mg/day is favourable at two to three months.15,16 Tapering should not be in the form of alternate day therapy as this is more likely to lead to a vasculitis relapse.14 Treatment length is mainly dictated by response to therapy and disease flare, and can vary. Adverse effects of glucocorticoids should be anticipated and patients told about them. Prophylaxis against steroid-induced osteoporosis is always recommended.17
Immunosuppressive therapy
To minimise the long-term steroid side-effects, steroid-sparing strategies have been evaluated in recent times.13 There have been three small randomised controlled trials (RCTs) evaluating methotrexate as adjunctive therapy to glucocorticoid.15,18,19 A meta-analysis of these three trials demonstrated some benefit for methotrexate (10-15mg/week) in reducing the relapse rate and lowering the cumulative dose of glucocorticoid therapy.20 Although GCA has been characterised by granulomatous inflammation, anti-tumour necrosis factor (TNF) agents such as infliximab have shown no therapeutic benefit to date.21
Antiplatelet therapy
Patients with GCA are at an increased risk of developing cardiovascular and cerebrovascular events.22,23 The addition of low-dose antiplatelet agents such as aspirin (75-150mg/day) protects against such events and, in the absence of contraindications, should be prescribed to all patients.24
References
Hunder GG, Bloch DA, Michel BA et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum 1990; 33: 1122-8
EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis 2009; 68: 318–323
Karassa FB, Matsagas MI, Schmidt WA, Ioannidis JP. Meta-analysis: tes performance of ultrasonography for giant-cell arteritis. Ann Intern Med 2005; 142: 359–369
Bley TA, Wieben O, Uhl M et al. High-resolution MRI in giant cell arteritis: imaging of the wall of the superficial temporal artery. AJR Am J Roentgenol 2005; 184(1): 283-287
Hooisma GA, Balink H, Houtman PM et al. Parameters related to a positive test result for FDG PET(/CT) for large vessel vasculitis: a multicenter retrospective study. Clin Rheumatol 2012; 31(5): 861-871
Treglia G, Mattoli MV, Leccisotti L et al. Usefulness of whole-body fluorine-18-fluorodeoxyglucose positron emission tomography in patients with large-vessel vasculitis: a systematic review. Clin Rheumatol 2011; 30(10): 1265-1275
Quinn EM, Kearney DE, Kelly J et al. Temporal artery biopsy is not required in all cases of suspected giant cell arteritis. Ann Vasc Surg 2012; 26(5): 649-654
Younge BR, Cook BE Jr, Bartley GB et al. Initiation of glucocorticoid therapy: before or after temporal artery biopsy? Mayo Clin Proc 2004; 79(4): 483
Bury D, Joseph J, Dawson TP. Does preoperative steroid treatment affect the histology in giant cell (cranial) arteritis? J Clin Pathol 2012
Danesh-Meyer H, Savino PJ, Gamble GG. Poor prognosis of visual outcome after visual loss from giant cell arteritis. Ophthalmology 2005; 112: 1098–1103
Gonzalez-Gay MA, Blanco R, Rodriguez-Valverde V et al. Permanent visual loss and Cerebrovascular accidents in giant cell arteritis: predictors and response to treatment. Arthritis Rheum 1998; 41: 1497–1504
Proven A, Gabriel SE, Orces C et al. Glucocorticoid therapy in giant cell arteritis: duration and adverse outcomes. Arthritis Rheum 2003; 49: 703–708
Hayreh SS, Zimmerman B, Kardon RH. Visual improvement with corticosteroid therapy in giant cell arteritis. Report of a large study and review of literature. Acta Ophthalmol Scand 2002; 80: 355–367
Hunder GG, Sheps SG, Allen GL, Joyce JW. Daily and alternate-day corticosteroid regimens in treatment of giant cell arteritis: comparison in a prospective study. Ann Intern Med 1975; 82:613.
Hoffman GS, Cid MC, Hellmann DB et al. A multicenter, randomized, double-blind, placebo-controlled trial of adjuvant methotrexate treatment for giant cell arteritis. Arthritis Rheum 2002; 46: 1309–1318
Mazlumzadeh M, Hunder GG, Easley KA et al. Treatment of giant cell arteritis using induction therapy with high-dose glucocorticoids: a double-blind, placebo-controlled, randomized prospective clinicaltrial. Arthritis Rheum 2006; 54: 3310–3318
Cortet B, Hachulla E, Barton I et al. Evaluation of the efficacy of etidronate therapy in preventing glucocorticoid-induced bone loss in patients with inflammatory rheumatic diseases. A randomized study. Rev Rhum Engl Ed 1999; 66: 214–219
Jover JA, Hernandez-Garcia C, Morado IC et al. Combined treatment of giant-cell arteritis with methotrexate and prednisone. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 2001; 134: 106–114
Spiera RF, Mitnick HJ, Kupersmith M et al. A prospective, double-blind, randomized, placebo controlled trial of methotrexate in the treatment of giant cell arteritis (GCA). Clin Exp Rheumatol 2001; 19: 495–501
Mahr AD, Jover JA, Spiera RF et al. Adjunctive methotrexate for treatment of giant cell arteritis: an individual patient data meta-analysis. Arthritis Rheum 2007; 56: 2789–2797
Hoffman GS, Cid MC, Rendt-Zwagar KE et al. Infliximab for maintenance of glucocorticosteroid-induced remission of giant cell arteritis: a randomized trial. Ann Intern Med 2007; 146: 621–630
Ray JG, Mamdani MM, Geerts WH. Giant cell arteritis and cardiovascular disease in older adults. Heart 2005; 91: 324–328
Le Page L, Duhaut P, Seydoux D et al. Incidence of cardiovascular events in giant cell arteritis: preliminary results of a prospective double cohort study (GRACG). Rev Med Interne 2006; 27: 98–105
Lee MS, Smith SD, Galor A, Hoffman GS. Antiplatelet and anticoagulant therapy in patients with giant cell arteritis. Arthritis Rheum 2006; 54: 3306–3309
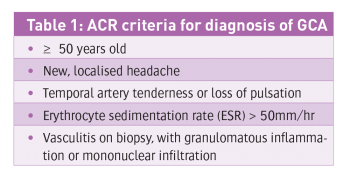 Table 1: ACR criteria for diagnosis of GCA(click to enlarge)
Table 1: ACR criteria for diagnosis of GCA(click to enlarge)