Medication prescribing in an inpatient psychiatric hospital
Dr Aoife Curley, Dr Guy Molyneux, Anne Brennan and Prof Brendan Kelly completed three cycles of audit of the improvement of medication prescribing practices in an acute inpatient psychiatric hospital
Dr Aoife Curley, Registrar in Psychiatry, University College Dublin and Mater Misericordiae University Hospital, Dublin, Prof Brendan Kelly, Associate Clinical Professor of Psychiatry and Consultant Psychiatrist, University College Dublin and Mater Misericordiae University Hospital, Dublin, Dr Guy Molyneux, Consultant Psychiatrist and Clinical Director, Department of Adult Psychiatry, UCD School of Medicine and Medical Science, Mater Misericordiae University Hospital and St Vincent's Hospital, Dublin and Ms Anne Brennan, Nurse Practice Development Co-Ordinator, St Vincent's Hospital, Fairview
Medication errors are common, complex and costly.1 A medication error is any error in the medication use process, from prescription to consumption.2 Medication error can be related to several factors, including:
• Patient factors (eg. poor physical or mental health).
Preventable adverse drug events, including medication errors, occur in a significant proportion of all hospital admissions, even in teaching hospitals.1 A study from a tertiary care hospital identified medication errors in 11.5% of all cases and reported that medication administration errors were the most common, followed by prescribing errors.3
In 1999, the US Institute of Medicine estimated that medication errors accounted for 98,000 inpatient deaths annually, which exceeded the annual deaths from breast cancer, vehicle accidents or acquired immune deficiency syndrome.1
Clinical audit is an important and effective way of remedying medication error4 and improving prescribing practices, even if certain deficiencies may remain following completion of a rigorous audit cycle.5 This article describes three cycles of an audit process based in one acute psychiatric hospital, aimed at identifying and reducing certain medication errors among adolescent, adult and old-age psychiatry inpatients. More specifically, we aimed to audit the safe and correct use of a recently introduced medication prescribing record (Kardex) at the hospital to see if a specially-designed educational intervention improved safe and correct use of the new medication record.
Methods
This audit was based in a Dublin psychiatric hospital catering for adolescent, adult and old-age psychiatry inpatients. Each patient has an individual medication prescribing record on paper, on which doctors write prescriptions and nursing staff record administration of medication. In May 2011, a new medication prescribing record was introduced at the hospital aimed at increasing the safety and accuracy of prescription and administration of medication based on examples of best practice from other hospitals.
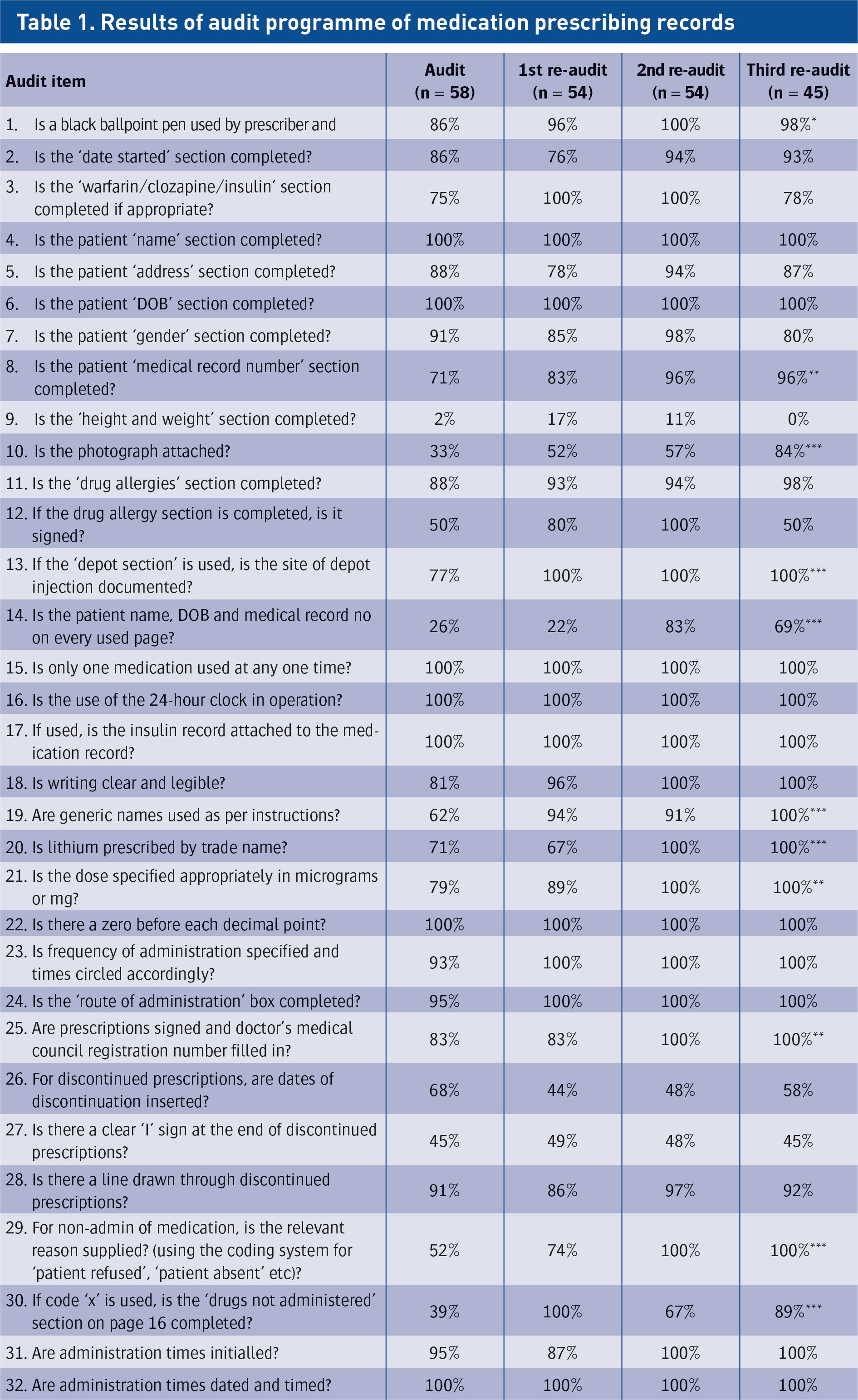
In order to audit the extent to which the new medication record was being used correctly, an audit of the medication records of all adolescent, adult and old-age psychiatry inpatients on a single day (58) was carried out in February 2012. The 32-item audit tool was devised by the multidisciplinary drugs and therapeutic committee to examine key features of the new medication record (see Table 1).
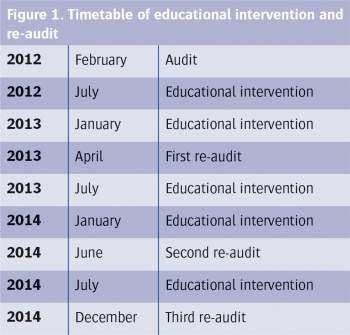
To improve the practice and use of medication records, a presentation was made to relevant hospital staff. Targeted education for staff was provided by the hospital pharmacist in July 2012 and January 2013. Copies of the medication record instructions were also given to each doctor. The medication records of all inpatients were re-audited on a single day in April 2013 to see if these interventions had improved prescribing and recording practices.
The educational intervention was repeated in July 2013 and January 2014; a second re-audit was performed in June 2014; the educational intervention was repeated in July 2014 and a third re-audit was performed in December 2014. Overall, the timetable was as in Figure 1.
This study was performed in accordance with the Declaration of Helsinki (World Medical Association, 2008)6 and data protection guidelines on research in the health sector.7 Data were stored on a password-protected research computer in a locked research office. Data were anonymised and encrypted. Appropriate data protection legislation was adhered to and patient confidentiality was protected at all times.
In order to provide an overall assessment of progress over the three-year period of the audit programme, and avoid problems associated with multiple statistical testing, statistical comparison of proportions compared results from the third re-audit with those from the initial audit; statistical significance was set at p < 0.05.
(click to enlarge)
Key *** p<0.05; *** p<0.01; *** p<0.001 (comparing proportions in the third re-audit with the initial audit)(click to enlarge)
Results
Audit (February 2012)
Levels of compliance with each of the 32 required aspects of the medication record audited ranged from 100% to 2% (Table 1). Seven items were completed on all medication records audited (ie. 100%), these were: name, date of birth, use of only one medication record per patient, use of 24-hour clock, use of insulin record where appropriate, use of ‘zero’ before decimal point, and recording medication administration time and date. The lowest scores were for recording height and weight (recorded on 2% of medication records); recording name, date of birth and medical record number on every page of the medication record (26%); attaching patient photograph (33%); specifying the reason for non-administration of medication (39%); and entering a clear ‘I’ sign at the end of discontinued prescriptions (45%).
Intervention (July 2012 and January 2013)
Following the initial audit, the intervention comprised targeted education for staff by the hospital pharmacist, provided in July 2012 and January 2013. Copies of the medication record instructions were also given to each doctor.
First re-audit (April 2013)
At the first re-audit, compliance with required aspects of the medication record had improved for 16 of the 32 items, eight items remained unchanged (seven of which remained at 100% and eight items disimproved (Table 1). The largest improvements were seen with: completion of the ‘drugs not administered’ section (improvement of 61%); use of generic names for medications (32%); and signing the ‘drugs allergies’ section (30%). The lowest scores were, again, for recording height and weight (17%, improved from 2%) and recording the patient’s name, date of birth and medical record number on every page of the medication record (22%, disimproved from 26%); the next lowest score was for recording the date of discontinuation of mediation (44%, disimproved from 68%).
Intervention (July 2013 and January 2014)
Following the first re-audit, the intervention again involved targeted education for staff by the hospital pharmacist in July 2013 and January 2014. Copies of the medication record instructions were also given to each doctor.
Second re-audit (June 2014)
At the second re-audit, compliance with required aspects of the medication record had improved for 17 of the 32 items, compared with the first re-audit; 11 items remained unchanged (all of which remained at 100%); and four items disimproved (Table 1). The largest improvements were seen with recording the patient’s name, date of birth and medical record number on every page (improvement of 61%) and prescribing lithium using trade-name (33%). The lowest score was, again, for recording height and weight (11%).
Intervention (July 2014)
Following the second re-audit, the intervention once again involved targeted education for staff by the hospital pharmacist in July 2014. Copies of the medication record instructions were also given to each doctor.
Third re-audit (December 2014)
At the third re-audit, compliance with required aspects of the medication record had improved for five of the 32 items, compared with the second re-audit; remained unchanged for 17 items (16 of which remained at 100%); and disimproved for 10 items (Table 1). The largest improvements were seen with attaching the patient’s photograph to the medication record (improvement of 27%) and with completion of the ‘drugs not administered’ section (22%). The lowest score was, again, for recording height and weight (0%, compared to 11% in the second re-audit, 17% in the first re-audit and 2% in the initial audit).
Statistical analysis
Compared to the initial audit, the third re-audit showed that, over the entire three-year period, compliance with 12 of the 32 required aspects of the medication record had improved to a statistically significant degree (p < 0.05) (see Table 1). Overall, the largest improvements were seen with attaching the patient’s photograph to the medication record (improvement of 51%; p < 0.001) and with completion of the ‘drugs not administered’ section (50%; p < 0.001).
Compliance improved, but the improvement was not statistically significant for seven items and compliance remained unchanged for nine items, seven of which remained at 100%. Compliance disimproved for four items and while the largest disimprovements were seen with completing the ‘gender’ section of the medication record (disimprovement of 11%) and inserting dates of discontinuation of medication (10%), none of these disimprovements were statistically significant (p > 0.05). Throughout the entire audit process, the lowest score was for recording height and weight, which was 2% in the initial audit and 0% in the third re-audit.
Discussion
The audit process described in this article demonstrated statistically significant improvement in compliance with 12 of the 32 required aspects of the new medication prescribing record. While there were no statistically significant disimprovements overall, it is notable that certain improvements observed mid-audit were not always sustained until the third re-audit, and compliance with certain items (notably recording height and weight) remained low throughout.
This audit cycle had several strengths. It studied and sought to produce improvements in an aspect of practice common to virtually all psychiatric inpatient settings, maintaining an accurate and complete medication prescribing record. It also presents not only an initial audit and re-audit following an educational intervention, but also results of second and third re-audits following further educational interventions. Finally, results from the third re-audit are compared with the initial audit in order to provide an assessment of overall progress, but avoid the problems of multiple statistical tests.
Limitations include the possibility that the standards for the medication record agreed by the drugs and therapeutic committee at this hospital may not have been identical to the standards devised elsewhere, although it appeared likely that there would be substantial overlap between these standards and those devised elsewhere. It is also noteworthy that different hospital staff (eg. different non-consultant hospital doctors) were working in the hospital for various periods throughout the audit; this, however, is the situation in most, if not all, psychiatric hospitals and in our view increases the applicability of our results to other psychiatric hospitals.
Overall, the improvements seen in 12 of the 32 required aspects of the medication record demonstrate that targeted education and presentations can improve correct use of medication prescription records. It is especially notable that large improvements were seen with attaching the patient’s photograph to the medication record (overall improvement of 51%) and completion of the ‘drugs not administered’ section (50%); both of these are important standards in ensuring patient safety and the accuracy of the medication record.
Notwithstanding these improvements, however, this audit cycle also showed continued room for improvement. Compliance with certain items (notably recording height and weight) remained low throughout, despite the educational interventions provided over the course of the audit cycle. This is similar to the findings of Tully et al5 who also studied medication prescription practices and found that while an audit cycle improved adherence to certain standards, certain deficiencies remained.
Conclusions
Introduction of a new medication prescribing record, coupled with repeated educational interventions, produced significant improvements in some, but not all, aspects of prescribing. Levels of compliance with various standards changed significantly over the audit period, emphasising the importance of continued education and other interventions in sustaining improvements. Further quantitative research could usefully examine the potential cumulative benefits of further audit cycles, while qualitative work could use focus-group methodologies to identify why compliance with certain standards improved and compliance with others did not
References
Kohn KT, Corrigan JM, Donaldson MS (eds) (2000). To Err Is Human: Building a Safer Health System. National Academy Press: Washington DC
Wittich CM, Burkle CM, Lanier WL. Medication errors: an overview for clinicians. Mayo Clin Proc 2014 ; 89:1116-1125
Karthikeyan M, Lalitha D. A prospective observational study of medication errors in general medicine department in a tertiary care hospital. Drug Metabol Drug Interact 2013 ; 28:13-21
Jainer AK, Noushad F, Coupe T et al. Mind the gap – using clinical audit to minimise medication information errors at hospital discharge. Psychiatr Bull 2010; 34:248-250
Tully J, Park E, Dunne A et al. (2010) Analysis of prescribing practices in an acute psychiatric ward. Ir J Psychol Med 27: 82-85
World Medical Association. WMA Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects. World Medical Association: Ferney-Voltaire, 2008
Data Protection Commissioner. Data Protection Guidelines on Research in the Health Sector. Data Protection Commissioner: Dublin.Data Protection Commissioner. Data Protection Guidelines on Research in the Health Sector. Data Protection Commissioner: Dublin, 2007
 (click to enlarge)
(click to enlarge)