Familial hypercholesterolaemia (FH) is an inherited condition thought to affect up to one in 250 people, and is associated with markedly raised serum LDL-cholesterol (LDL-C) levels.1 This high LDL-C level is present from birth and can lead to early development of atherosclerotic cardiovascular disease. However, as early atherosclerosis doesn’t result in symptoms, familial hypercholesterolaemia is often clinically silent until an individual with FH has an acute myocardial infarction or a sudden death. FH patients often present with a myocardial infarction, stroke or sudden death in their 20s, 30s or 40s. At least 50% of men with familial hypercholesterolaemia will present with heart disease by the age of 50 and as many as 30% of women will present with heart disease by the age of 60.2
Familial hypercholesterolaemia is not caused by an unhealthy lifestyle, but is passed from generation to generation through pathogenic variants in the gene sequence of the low-density lipoprotein receptor gene (or less commonly in the sequence of two other genes). As a monogenic disorder, brothers and sisters or children of someone with familial hypercholesterolaemia have a 50% chance of having the condition.
While FH patients generally choose healthy life choices, this is insufficient to minimise their risk of cardiovascular disease. As with the population in general, the risk of cardiovascular disease in FH patients is increased significantly by other factors such as high blood pressure, smoking and other unhealthy lifestyle choices.
Globally, the condition is both underdiagnosed and undertreated, with estimates as low as 5% of those affected being identified.3 Evidence suggests that familial hypercholesterolaemia is also significantly underdiagnosed and undertreated in Ireland with little or no data available on its prevalence, diagnosis or management. Some countries, such as the Netherlands, the UK and Northern Ireland have high rates of diagnosis and treatment, principally because they have national programmes of cascade screening supported by the necessary biochemical and genetic testing and developed pathways for clinical management. A strategy that has been effective in a number of jurisdictions is the screening of young children by measuring their cholesterol levels at the time of their vaccination. In Ireland however, there are no formal screening programmes for familial hypercholesterolaemia.
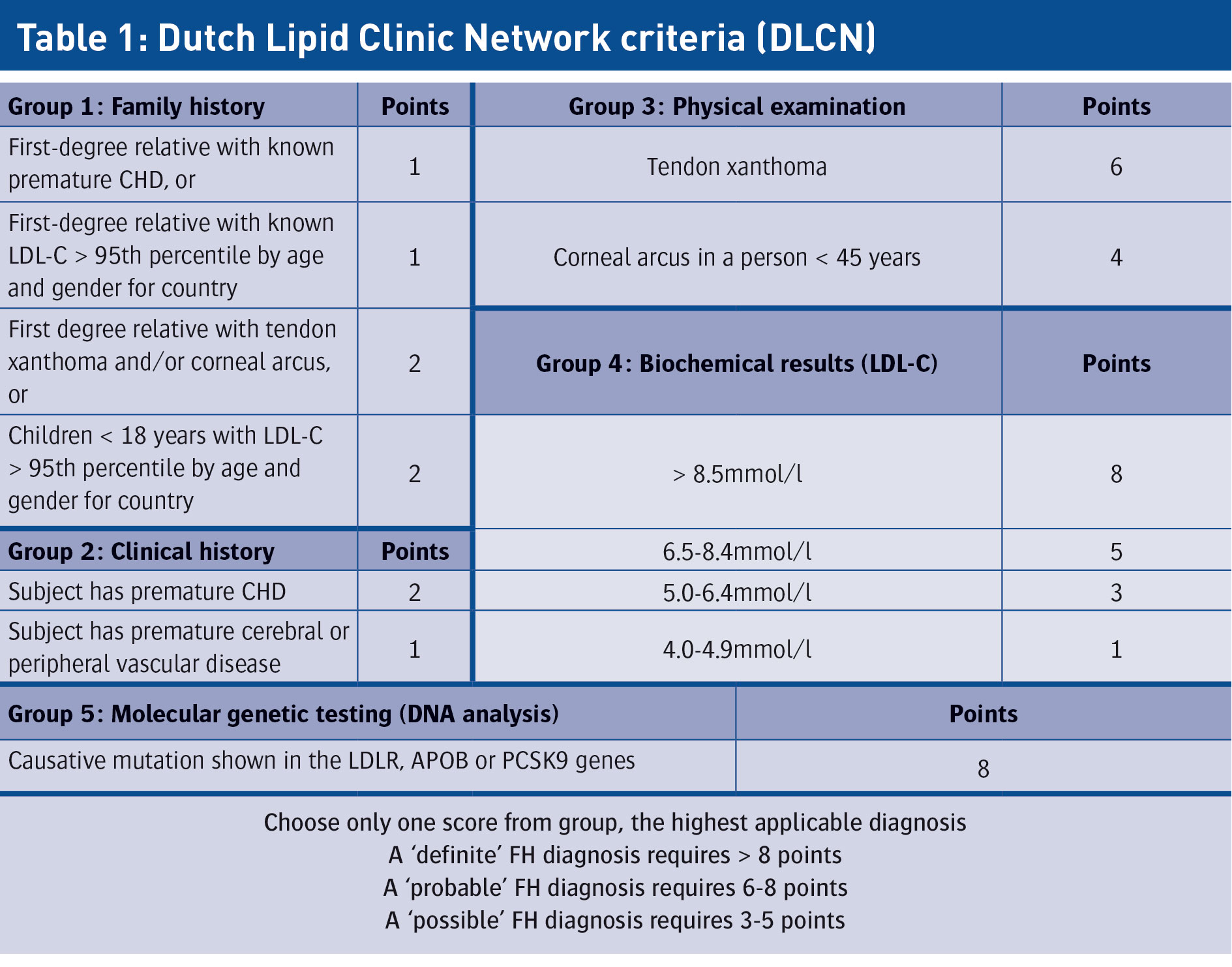
In many individuals, the diagnosis of FH is obvious from the personal or family history of CVD, the markedly elevated LDL-C levels and the presence of xanthomata or corneal arcus on examination. However, in many cases the diagnosis of FH is more challenging and relies on a mix of five criteria:
Family history of premature CVD
Personal history of premature CVD
Physical examination for xanthomas and corneal arcus
Very high LDL-C on repeated measurements
Causative mutation detected by molecular genetics.
FH likelihood scoring systems
FH likelihood scoring systems have been developed around these criteria – the Simon Broome criteria and the NICE guidelines for diagnostic criteria, for example. Internationally, the most accepted system appears to be the Dutch Lipid Clinic Network Criteria (DLCN),4 which classifies patients into ‘possible’, ‘probable’ or ‘definite’ FH (see Table 1). It’s now possible to offer genetic testing to patients to formalise the diagnosis. Such a service has been introduced in the chemical pathology laboratory at St James’s Hospital, Dublin by Dr Vivion Crowley.
(click to enlarge)
Early detection and management of familial hypercholesterolaemia and early initiation of lifestyle and pharmacological treatment are imperative to reduce the lifelong burden of CVD. Familial hypercholesterolaemia is often undertreated, even among those with an established diagnosis. Smoking cessation, diet and other lifestyle interventions are also essential to reducing the risk of CVD in FH patients. However, without the initiation of lipid-lowering therapy from an early age, FH patients will almost certainly be at high risk of CVD throughout their life.
In Ireland, based on the findings of international prevalence studies, it is likely that there are 10,000-20,000 individuals with familial hypercholesterolaemia. A small fraction of these are being actively managed by specialist lipid clinics where they are given a formal diagnosis, genetic counselling and a lifestyle and pharmacological management plan. Many FH patients are being managed in primary care and by other hospital-based outpatient services (eg. endocrinology, cardiology), but in these settings detection and management strategies may not always be optimised.
The use of statins is central to the pharmacological management of familial hypercholesterolaemia. However, the addition of other lipid-lowering medications (eg. ezetimibe and PCSK9 inhibitors) is appropriate in more challenging cases. While PCSK9 inhibitors have proven powerful and effective in managing difficult cases worldwide, they have not yet been approved for use in Ireland.
The not-for-profit sector has played an important role in raising awareness of familial hypercholesterolaemia. Heart UK – the cholesterol charity provides support, information and education on familial hypercholesterolaemia for healthcare professionals (HCPs), patients and families. The charity also works on raising awareness of familial hypercholesterolaemia among HCPs and policymakers with the aim of improving services for those impacted by the condition. In recent years, Heart UK has been instrumental in creating the European FH Patient Network (FH Europe).
In Ireland, Croí, the West of Ireland Cardiac and Stroke Foundation, is the only organisation with membership of FH Europe. Croí and its affiliate, the National Institute for Prevention and Cardiovascular Health (NIPC) have begun to engage on some of the FH challenges facing Ireland.
Strategic policy framework
In 2017, Croí and the NIPC contributed to an FH strategic policy framework report, commissioned by Amgen, to understand the barriers to establishing and implementing a standardised best practice approach to diagnosis and treatment of familial hypercholesterolaemia in Ireland.5 This report put a spotlight on many issues and challenges that need to be addressed to ensure that people living with familial hypercholesterolaemia in Ireland are identified and optimally treated. Included in these issues and challenges are:
Low awareness of the condition among the general public and relevant stakeholders: This lack of awareness extends from patients themselves, through primary and secondary clinical care settings, to politicians and policymakers
Low prioritisation of preventive screening in both primary and secondary care: It appears that identification of familial hypercholesterolaemia in Ireland is largely opportunistic, often only identified after surviving an acute presentation. UK research suggests that about a third of people with familial hypercholesterolaemia don’t survive their first heart attack. Preventive screening therefore would not only potentially prevent a cardiovascular event but prevent unnecessary damage to the heart and cardiovascular system
Low and disparate access and availability of patient services: In the UK, everyone between the ages of 40 and 75 can avail of free lipid-testing every five years. In Ireland, by contrast, the majority of residents must pay for GP visits and specialist care appointments. Furthermore, there is only a limited number of dedicated lipid clinics in secondary care capable of diagnosing and treating familial hypercholesterolaemia. In fact, there is low awareness among GPs of both the referral pathway and of where to refer the patient for further testing and treatment. Another barrier exists with regard to genetic testing, which is currently only available in one Dublin hospital with limited capacity. Other hospitals are sending samples to the UK, which is not always possible due to budgetary constraints
No national screening programme or database for the purpose of cascade screening of family members when someone is diagnosed with familial hypercholesterolaemia: Ireland joins Romania and Bulgaria at the bottom of the EU table for the lack of an aligned national strategy for FH screening, with the resulting absence of cascade screening, and the absence of national registers for either children or adults. International evidence confirms that cascade screening is the most cost-effective means of identifying previously undiagnosed FH patients.
Last year, Croí and the NIPC collaborated with Dr Damian Griffin, consultant chemical pathologist, who runs a lipid clinic in Galway University Hospital and four primary care practices in Galway, to conduct a therapeutic review of hypercholesterolaemia. The aims were to ascertain the prevalence of marked hypercholesterolaemia in the Galway area and to gain insights into how these patients are investigated. Based on the information available it was possible to draw conclusions as to the likelihood that these patients had familial hypercholesterolaemia. The management of these patients was also reviewed.
Lipid profiles on patients attending the four practices over a 15-year period were reviewed. Patients with marked hypercholesterolaemia, defined as having a total cholesterol ≥ 8mmol/L (in line with ECS guidelines), were selected. Medical records of the highlighted patients were then interrogated to ascertain whether these patients were likely to have familial hypercholesterolaemia based on the DLCNC scoring system.
While 137 patients were found with markedly elevated cholesterol levels, it was only possible to conclude that seven patients had definite familial hypercholesterolaemia. It was felt that in many other cases, there was a strong probability that the patients could have familial hypercholesterolaemia, but variances across practices in documenting criteria associated with FH meant it was not possible to reach firm conclusions in most cases. The GPs who participated in this study were provided with a more extensive list of patients who possibly had familial hypercholesterolaemia, but where further investigation was required before this could be confirmed.
This project highlighted some of the difficulties that need to be addressed in estimating the prevalence of familial hypercholesterolaemia in Ireland but also provided a good insight that will inform future research endeavours. An integrated approach at every level of the healthcare system is required.
Research, awareness and education
There are plenty of international best practice guidelines that could be adopted to vastly improve the cardiovascular health of those living with familial hypercholesterolaemia in Ireland. The NIPC is committed to supporting the research agenda in this arena and Croí is committed to mobilising the patient voice for awareness, education and advocacy.
As part of this commitment, the NIPC recently appointed Prof Bill McEvoy as its medical and research director. He has taken up a post as professor of preventive cardiology at NUI Galway and consultant cardiologist at Galway University Hospital, having returned from working in the US. Prior to this, Prof McEvoy was a faculty member in the Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease and was active in the advanced lipid clinic at the hospital. He has a track record of successful research in hyperlipidaemia and is widely published in this area, including a review on the treatment of hyperlipidaemia, due to be published this year in the New England Journal of Medicine. He plans on using his expertise to advance our understanding of familial hypercholesterolaemia in Ireland and to improve the treatment of Irish patients.
References
Akioyamen LE et al. Estimating the prevalence of heterozygous familial hypercholesterolaemia: a systematic review and meta-analysis. BMJ Open Sept 2, 2017
Simon Broome Register Group, Scientific Steering Committee. Risk of fatal coronary heart disease in familial hypercholesterolaemia. BMJ 1991 Oct 12 893–896
Nodestgaard et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease. Consensus statement of the European Atherosclerosis Society. Eur Heart J 2013, 34(45) 3478-3490
Ajufo E, Cuchel M. Improving the yield of genetic testing in familial hypercholesterolaemia. Eur Heart J 2017, 38, 574–576)
Familial Hypercholesterolaemia (FH) Strategic Policy Framework Report: A healthcare professional led consensus for the identification and management of FH in Ireland. September 2017
 (click to enlarge)
(click to enlarge)