CHILD HEALTH
Perforated appendicitis with faecolith in an infant
A case of a seven-month-old infant with perforated appendicitis with faecolith
October 1, 2018
-
A seven-month-old, previously well, Caucasian male infant presented in the emergency department with one-day history of runny nose, vomiting, decrease oral intake and low grade fever. He was discharged after a short stay with suspected gastroenteritis.
He presented again with irritability, decreased urine output, pyrexia, loose stools and bilious vomiting. There was no significant past medical and surgical history of note. On examination, he looked pale, diffusely mottled and had prolonged capillary refill time of three seconds. There was nonspecific blanching, macular rash on his abdomen, he was haemodynamically stable, and his abdomen was mildly distended and tender to touch on the right side with hypoactive bowel sounds. The clinical impression was sepsis or intussusception.
Blood gas was normal. Septic workup, including full blood count, liver functions and electrolytes, was normal.
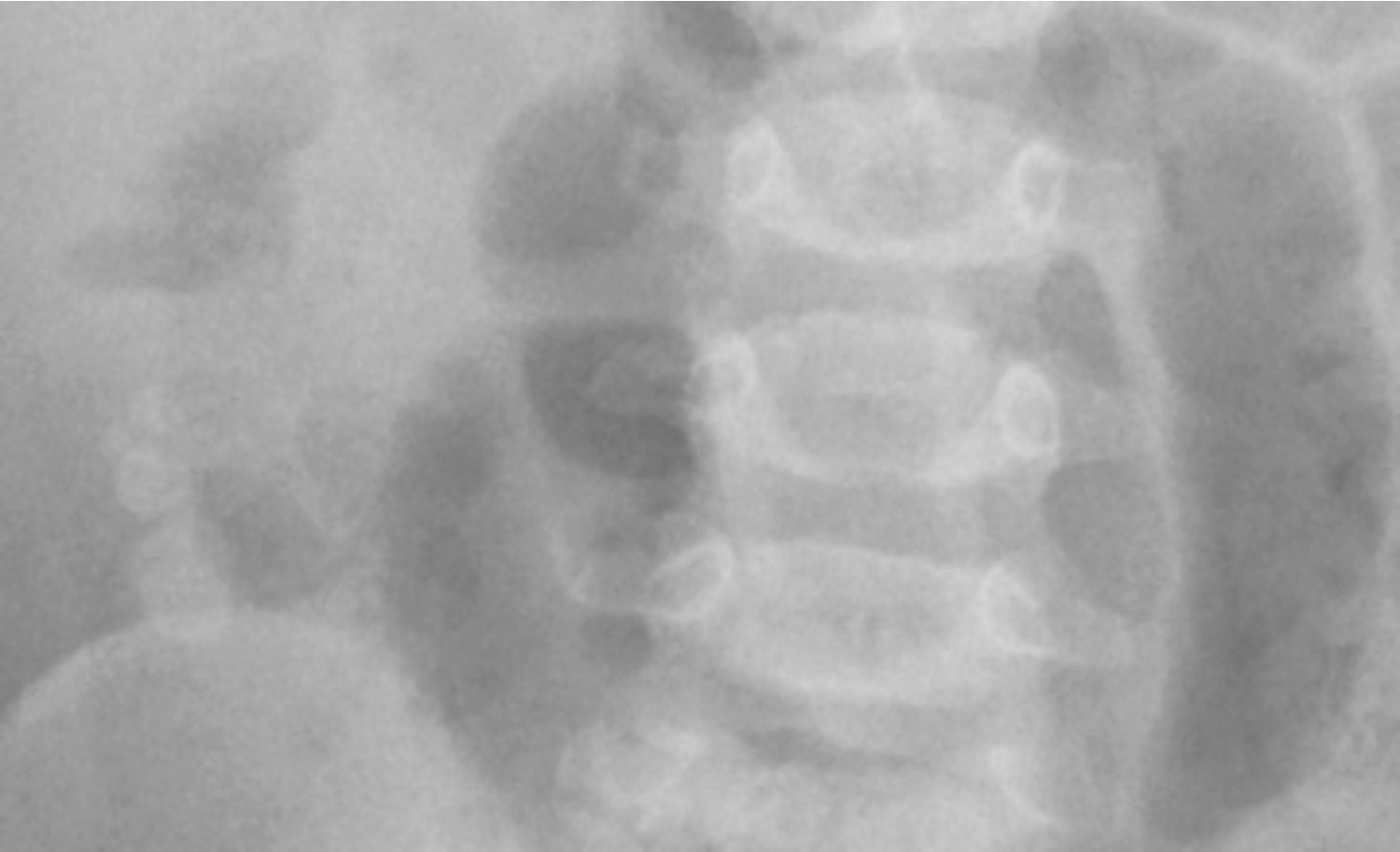
X-ray abdomen showed centrally situated, dilated, air filled small bowel loops. There were visible areas of calcification in RIF on plain film with provisional diagnosis of faecolith, confirmed later by ultrasound and laparoscopy.
US abdomen showed free fluid in the hepatorenal recess. A thick-walled oedematous tubular structure consistent with an inflamed appendix was observed in right flank anterior to the mid pole of the right kidney. This tubular structure appeared to be continuous with a tubular structure immediately inferior to it that contained at least four calcified densities. Therefore, diagnosis of perforated appendicitis with multiple faecolith was made.
The infant was resuscitated with IV fluids and broad spectrum antibiotics, was kept NPO with NG free drainage and was later transferred to the paediatric tertiary level facility for further management. He underwent an emergency laparotomy. The intraoperative finding confirmed perforated appendix with multiple faecoliths. The patient had an uneventful, but slow recovery during convalescence.
 (click to enlarge)
(click to enlarge)