Pharmacological treatments for people with acute stroke
Focusing on therapies useful in ischaemic events, this article outlines the best treatments available
Dr Paul McElwaine, Specialist Registrar in Geriatric Medicine, Centre for Gerontology and Rehabilitation, School of Medicine, UCC, Cork and Dr Suzanne Timmons, Consultant Geriatrician and Senior Lecturer, Centre for Gerontology and Rehabilitation, School of Medicine, UCC, Cork
Stroke is a common, debilitating disease process which requires an organised, multifaceted approach to ensure good outcomes. In this review article the primary focus is on acute pharmacological treatments of ischaemic stroke.
There is significant overlap in general principles of stroke management, whether it is ischaemic or haemorrhagic in aetiology, however, this review will refer predominately to therapies useful in ischaemic events. The principles of pharmacological management of stroke include prevention of propagation of the stroke and regulation of physiological parameters.
Antiplatelet therapy
Already well-established agents in long-term secondary prevention of stroke, the benefits of antiplatelet therapy in acute stroke is tempered by the risk of haemorrhagic transformation of the infarct.
Aspirin
The role of aspirin in improving acute stroke outcome was established in two randomised control trials: the International Stroke Trial (IST) and the Chinese Aspirin Stroke Trial (CAST).1,2
Combining these two studies, in 40,000 patients a small but significant benefit was seen in patients who received aspirin within 48 hours of onset of symptoms with one better outcome per 100 people treated. On exclusion of haemorrhage on cerebral imaging, a loading dose of 300mg of aspirin should be given. If concern exists for safety of the patient’s swallow, this can be given via nasogastric tube or via suppository.
The National Clinical Stroke Guidelines recommend continuing 300mg once daily for two weeks followed by definitive antithrombotic therapy for long-term prevention thereafter.3 If a history of aspirin-related dyspepsia exists, the addition of a proton pump inhibitor is appropriate.
Other agents
The role of clopidogrel is less well defined in acute stroke with fewer data available to support its use. However, in the setting of hypersensitivity to aspirin-containing products or severe dyspepsia secondary to aspirin then clopidogrel may be used. Similar to aspirin, a loading dose of 300mg should be given. There are almost no data on the effects of dipyridamole in acute stroke and therefore it is not recommended.
Anticoagulation
Systemic full-dose anticoagulation is equally as effective as aspirin in reducing mortality and functional dependence, however, it carries a significant intracranial and extracranial haemorrhage risk and therefore is not routinely used.
This haemorrhage risk also has implications in the management of cardioembolic stroke in patients with atrial fibrillation. Given the potential for haemorrhagic transformation of the infarct, a common approach is to wait up to two weeks before starting the definitive antithrombotic therapy, particularly with large infarcts. In less severe strokes and those that show early recovery, treatment is often initiated sooner, however, there is no clear evidence to guide practice in this regard. Immobilised patients such as those with stroke are at a high risk of DVT and pulmonary embolism. Low molecular weight heparin (LMWH) given as prophylaxis is known to reduce the incidence of DVT but also increase risk of cerebral haemorrhage.
The recent recommendations of the American College of Physicians4 advise:
Assessment of the risk for thromboembolism and bleeding in medical (including stroke) patients prior to initiation of prophylaxis of venous thromboembolism
Pharmacological prophylaxis with heparin or a related drug for venous thromboembolism in medical (including stroke) patients unless the assessed risk for bleeding outweighs the likely benefits
Against the use of mechanical prophylaxis with graduated compression stockings for prevention of venous thromboembolism
No support for the application of performance measures in medical (including stroke) patients that promote universal venous thromboembolism prophylaxis regardless of risk
If a patient with an ischaemic stroke develops a DVT then it is appropriate to treat with LMWH. In the setting of intracranial haemorrhage a Greenfield vena cava filter could be placed.
Control of physiological parameters
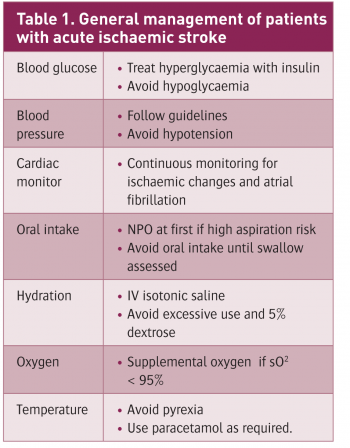
Any patient who has suffered a stroke should be managed and monitored in an appropriate setting, ie. a dedicated stroke unit or high-dependency bed. This facilitates more vigorous observation of their physiological parameters (see Table 1). The extent and intensity to which these parameters should be controlled is still somewhat contentious.
(click to enlarge)
Blood pressure
Hypertension is a major risk factor in development of an acute stroke. A majority of patients who present with stroke will be hypertensive on admission due to either pre-existing disease or as a stress response. This elevation in blood pressure has led to infarction and puts the patient at risk of haemorrhagic transformation and further strokes, but it is also maintaining cerebral perfusion for the area of ischaemia and the rest of the brain. Significant drops in blood pressure may aggravate cerebral ischaemia, particularly in the vulnerable ischaemic penumbra, and promote neuronal death.
The current guidelines do not recommend blood pressure-lowering in patients with acute stroke unless levels are extremely high or thrombolysis is being considered (see Table 2). If rapid reduction is required then IV labetalol is an appropriate choice, with alternatives including IV isosorbide dinitrate or nicardipine. The recent SCAST trial which looked at the role of candesartan versus placebo in acute stroke concluded that clinicians should not prescribe blood pressure lowering agents in the first week of acute stroke.5 In patients already on antihypertensive medication, it is reasonable to continue them with close blood pressure observation.
(click to enlarge)
Blood glucose
Hyperglycaemia is often present in the setting of acute stroke. This can be seen in patients with diabetes or as a stress response in a non-diabetic patient. Animal models have shown that hyperglycaemia causes an increase in infarct size and worse outcome and also that insulin therapy improves brain ischaemia, however, this has not been borne out in human trials.6 Current recommendations are to maintain a blood glucose of 4-11mmol/L while avoiding the neurologically detrimental effects of hypoglycaemia using an insulin sliding scale. There is no proven role for any oral hypoglycaemic agents in acute stroke.
Oral intake and hydration
Dysphagia occurs in almost 50% of stroke patients initially and approximately one-third aspirate to a clinically significant extent, especially in the first week. Patients should be prohibited from eating or drinking (NPO) until their ‘swallowing’ is assessed by a trained professional. Passing a nasogastric tube in clinically appropriate patients will provide means to delivering medication and managing nutritional requirements as a short-term measure. Hydration can be supplemented by intravenous fluid, usually isotonic saline, but avoid excessive use of fluids. Dextrose based fluids may aggravate cerebral oedema and are best avoided.
Temperature
Fever in the setting of stroke is more often than not related to an infective source. The regular use of high-dose paracetamol showed no significant benefit above placebo, but should be used on an as-required basis.7 Controlled hypothermia reduces cerebral metabolism and so may reduce the neurological deficit in acute stroke. However, it causes many complications itself and there may be a rebound worsening of status after re-warming, so it is not standard treatment.8 Further studies are exploring the duration and degree of hypothermia required for optimal results.
Oxygenation
Patients should receive supplemental oxygen therapy only if their oxygen saturation level falls below 95%. There is no evidence to support the routine use of oxygen in the absence of hypoxaemia.
Neuroprotection
In the setting of an acute stroke, cerebral ischaemia gives rise to a cascade of events, including free radical accumulation, acidosis and accumulation of intracellular calcium, which ultimately leads to neuronal death. In the area of brain that is under-perfused, some neurons will be irreversibly damaged, while some are just ‘stunned’ and capable of recovery with time, the so-called ischaemic penumbra.
Many neuroprotective therapies have been developed to try to protect these potentially salvageable neurons, and to extend the time-window for giving thrombolysis without reperfusion-associated neuronal damage. Numerous agents which showed promising results in animal models have yet to demonstrate similar benefits in human trials.
Examples trialled include calcium channel antagonists (which showed benefit in subarachnoid haemorrhage only), glutamate, NMDA receptor antagonists and recently free radical scavengers such as NXY-059, which after initial promising results failed to replicate its promise in a follow-up study (SAINT studies).9
Malignant cerebral infarction
Cerebral oedema post-stroke occurs due to the breakdown of neuronal cell membranes, cytotoxic oedema, and by disruption of the blood-brain barrier, vasogenic oedema. It may be seen in large middle cerebral artery infarcts, the so-called malignant cerebral infarction, or in haemorrhagic strokes (see Figure 1). Cerebral oedema may result in temporal lobe herniation, brainstem compression, hydrocephalus, and reduced cerebral blood flow. Glycerol,10 mannitol,11 and steroids12 have not been found to improve prognosis in stroke-related cerebral oedema.
Figure 1: Left MCA infarction with cerebral oedema and midline shift(click to enlarge)
Two open, non-randomised prospective studies showed a benefit in terms of survival and function for hemicraniectomy (but the operated patients were younger and fitter and all patients were managed in a neuro ITU).13,14 This involves removing part of the skull vault to allow the cerebral hemispheres to expand without compression of other parts.
Discussion
Of the 10,000 people who suffer a stroke each year in Ireland, their outcome is dependent on many facets. From a pharmacological point of view the increased facility to deliver thrombolysis is welcomed, however, a large proportion of patients still rely on the principal treatments outlined above. Although the work so far on neuroprotection has been disheartening, a number of trials are still ongoing. In the meantime, as the stroke service continues to expand and improve in this country, we should aim to provide care which meets the standards of best international practice.
References
The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. International Stroke Trial Collaborative Group. Lancet 1997; 349(9065): 1569-1581
CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet 1997; 349(9066): 1641-1649
Irish Heart Foundation: Council for Stroke. National Clinical Guidelines and Recommendations for the Care of People with Stroke and Transient Ischaemic Attack October 2009. (www.irishheart.ie/iopen24/pub/strokereports/strokeguidelines.pdf)
Qaseem A, Chou R, Humphrey LL et al. Venous thromboembolism prophylaxis in hospitalized patients: a clinical practice guideline from the American College of Physicians. Ann Internl Med 2011; 155(9) 625-632
Fischer U, Rothwell PM. blood pressure management in acute stroke: does the Scandinavian candesartan acute stroke trial (SCAST) resolve all of the unanswered questions? Stroke 2011; 42(10): 2995-2998
Gray CS, Hildreth AJ, Sandercock PA et al. Glucose-potassium-insulin infusions in management of post-stroke hyperglycaemia: the UK Glucose Insulin in Stroke Trial (GIST-UK). Lancet Neurol 2007; 6(5): 397- 406
den Hertog HM, van der Worp HB, van Gemert HMA et al. The Paracetamol (Acetaminophen) In Stroke (PAIS) trial: a multicentre, randomised, placebo-controlled, phase III trial. Lancet Neurol 2009; 8(5): 434-440
Groysman LI, Emanuel BA, Kim-Tenser MA et al. Therapeutic hypothermia in acute stroke. Journal of Neurosurgery, Neurosurgical Focus 2011; 30(6): 7
Shuaib A, Lees LK, Grotta J et al. SAINT II: results of the second randomized, multicenter, placebo-controlled, double-blind study of NXY-059 treatment in patients with acute ischemic stroke. Stroke 2007; 38: 471
Righetti E, Celani MG, Cantisani T et al. Glycerol for acute stroke. Cochrane Database Syst Rev 2000; (4) CD000096
Hofmeijer J. Treatment of space-occupying cerebral infarction. Crit Care Med 2003; 31(2): 617-25
Qizilbash N, Lewington SL, Lopez-Arrieta JM et al. Corticosteroids for acute ischemic stroke (Cochrane Review) The Cochrane Library 2003; 1
Rieke K, Schwab S, Krieger D et al. Decompressive surgery in space-occupying hemispheric infarction: Results of an open, prospective trial. Crit Care Med 1995; 23: 1576-1587
Schwab S, Steiner T, Aschoff A et al. Early hemicraniectomy in patients with complete middle cerebral artery infarction. Stroke 1998; 29: 1888-1893
 (click to enlarge)
(click to enlarge)

