Primary cutaneous squamous cell carcinoma - an update
A team from Beaumont Hospital outline the current recommendations for investigation and treatment of CSCC's and highlights high-risk tumours with the potential to metastasise
With primary cutaneous squamous cell carcinomas (CSCC) on the rise and the widely varying malignant behaviour of these tumours, a timely diagnosis and referral of patients with CSCC is imperative. This update aims to outline the current recommendations with regards to diagnosis, investigation, referral and treatment.
Definition and epidemiology
Primary CSCC is a malignant tumour that arises from the keratinising cells of the epidermis or its appendages. It is locally invasive and has the potential to metastasise.1 The age standardised incidence rate of CSCC in Ireland is 156 cases per 100,000 per year.2 Current projection models for non melanoma skin cancers projects that female case numbers will increase by 162-235% between 2010 and 2040 and male cases by 157-356%, with proportionate increases in treatment rates.2 There is a rising incidence with age. Men are more commonly affected, probably because of greater head and neck exposure to ultraviolet radiation (UVR).3
Risk factors
Chronic UVR exposure is the most important risk factor. It may also develop de novo in those exposed to chemical carcinogens or in areas of chronic inflammation, such as chronic wounds, scars, burns or ulcers. Individuals with an impaired immune function are at higher risk of developing CSCC, with up to 30% of renal transplant recipients (RTRs) developing CSCC within 10 years of transplantation.2
The risk of CSCC in a transplant recipient is 40-250 times greater than that in the general population, and CSCC in these patients is a very significant cause of morbidity and mortality (see Figure 1).
Pre-malignant conditions include Bowen’s disease and indeed multiple actinic keratosis (AK) are associated with an estimated 10% lifetime risk (see Figure 2).
Figure 1. Rapidly growing scalp SCC in a RTR one year post-transplant, the patient had a small area of keratosis prior to his transplant that had rapidly developed on immunosuppression. He required a skin graft at excision(click to enlarge)
Figure 2. Bowen's (SCC in situ) on the lower limb, required excision and skin grafting(click to enlarge)
Presentation
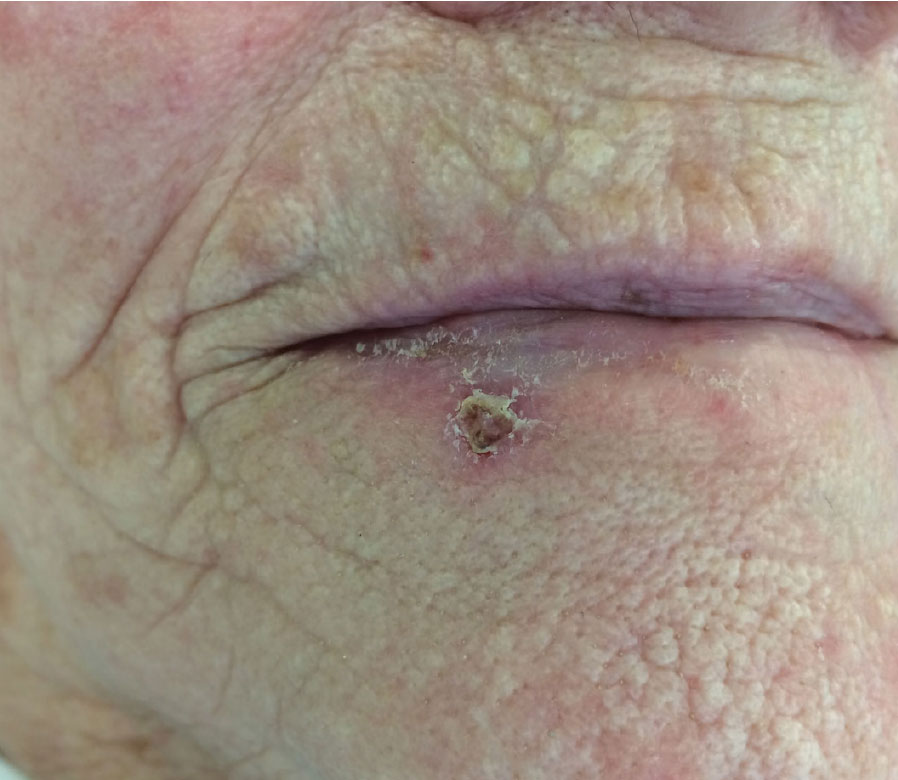
CSCC presents in a variety of ways but usually as an indurated nodular keratinising or crusted tumour that may ulcerate, or it may present as an ulcer without evidence of keratinisation (see Figure 3). In some instances patients may present with a hyperkeratotic papule which can be tender, a sign of transformation to CSCC.
Typically patients complain of a non-healing ulcer or growth in one of the higher-risk sun-exposed areas. Most CSCCs appear on the skin of the head and neck but may also appear on the extremities, most commonly the arms in men and the legs in women. Bleeding may occur. The lesion may be both spontaneously painful and/or tender. CSCC may give rise to local metastases or spread to local lymph nodes. The overall rate of CSCC metastasis is low (<5%)9(see Figures 3 and 4).
Of note, CSCC may be present in the base of a cutaneous horn in up to 20% of cases and for this reason these should be excised.9
The differential diagnosis includes keratoacanthoma, actinic keratosis (AK), basal cell carcinoma (BCC), malignant melanoma, seborrhoeic keratosis, cutaneous horn, pyogenic granuloma and plantar wart.
Figure 3. Lower lip SCC. The patient had a previous wedge excision of an SCC of the lower left lip(click to enlarge)
Figure 4. Large SCC on the lower limb, required excision and skin grafting. The patient was placed on post-operative antibiotics as it was ulcerating. The patient had no inguinal lymphadenopathy on examination(click to enlarge)
Diagnosis
The diagnosis is established histologically, ideally by excisional biopsy. Incisional/punch biopsy under local anaesthesia can be employed if the lesion is large, in a cosmetically sensitive area or is near to vital structures, under local anaesthesia.1,5,6 Shave biopsies should not be performed. The full thickness of skin should be taken to determine the depth of the lesion and should be wide of the margins to achieve clearance. The histolopathological report should include the following details according to AJCC guidelines:1,5,9
• Macroscopic details: specimen and lesion size
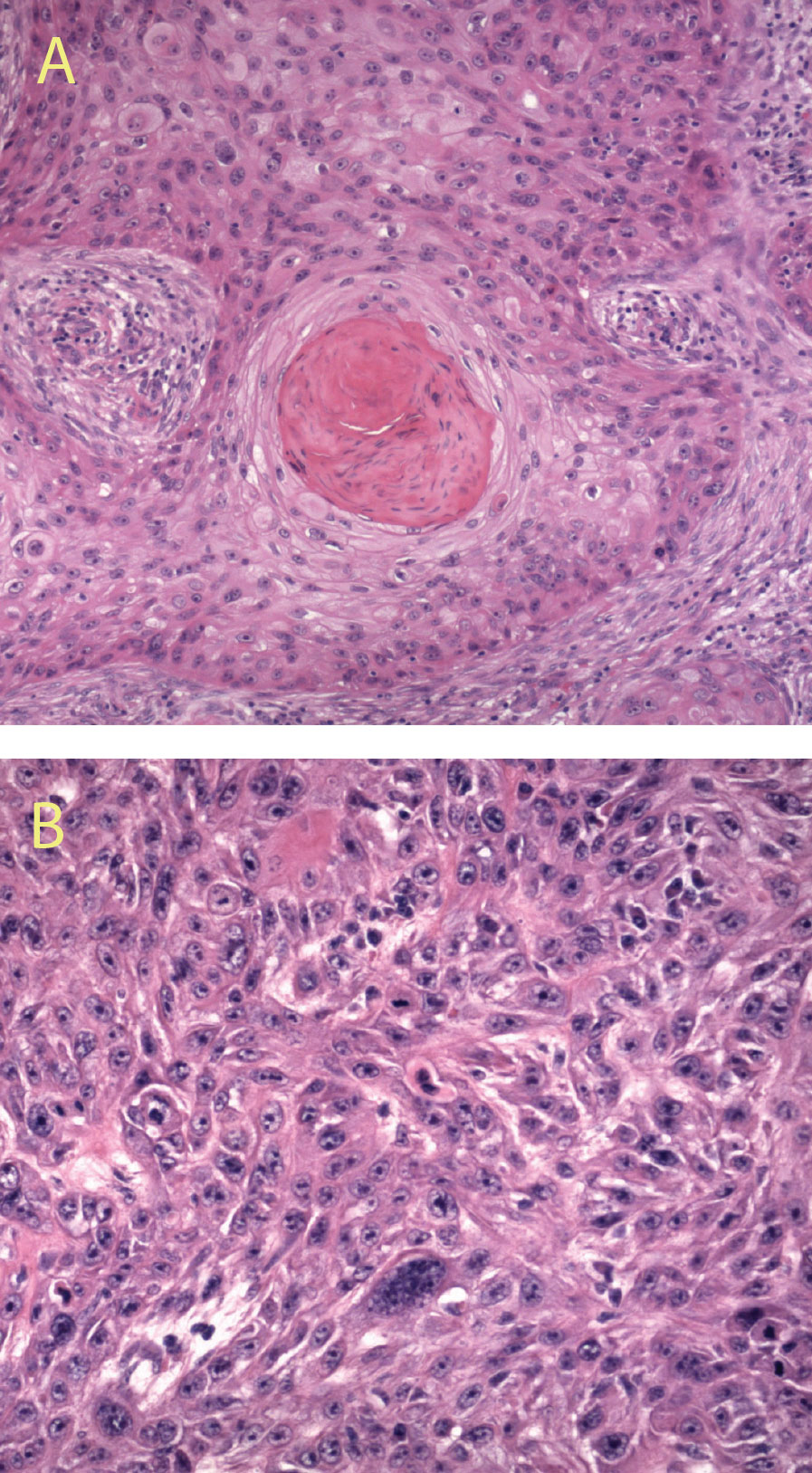
• Microscopic details (see Figure 5a and 5b):
– Histopathological subtype
– Grade/tumour differentiation
– Tumour depth/level of invasion
– Maximum diameter
– Lymphovascular invasion
– Perineural invasion
– Margins.
High-risk pathological and clinical features upstage a lesion from pT1 to pT2.
In AJCC7, pT2 is defined as either maximum diameter > 20mm, or pT1 (ie. ≤ 20mm) upstaged two high-risk features:5
– Grade – poorly differentiated or undifferentiated
– Peri-neural invasion
– Thickness > 2mm
– Clark level ≥ 4
– Clinical – ear and lip.
According to SIGN guidelines, where any of the following high-risk features are present, patients with primary SCC should be discussed at a skin cancer multidisciplinary team meeting:9
SCC arising on the ear
Tumour diameter > 20mm
Tumour depth > 4mm
Tumour extending beyond dermis into or through subcutaneous fat
Perineural invasion
Poorly differentiated
Desmoplastic subtype
Immunosuppression.
Figure 5. High power magnification of a well differentiated SCC (A) and a poorly differentiated SCC (B) (click to enlarge)
Investigations1,5,6
In advanced stages of disease, further investigations to assess the extent of disease may be required: CT is ideal to assess for bone or soft tissue spread, and in particular helps to delineate involved cervical lymph nodes. MRI is useful for head and neck spread, and assessing perineural invasion. Radioisotope bone scans can help identify suspected bony metastases
Communication1
Having a diagnosis of cancer can evoke many emotions within a person. Good communication skills are important to the clinician when imparting diagnosis and information. It is essential that each person with CSCC receives very clear and fully informed verbal and written advice. Some people may require additional psychological support and this can often be accessed through the multiprofessional supportive and palliative care team.
Referral
Indications for referral to an appropriately trained specialist, according to several different guidelines (SIGN, BAD, NICE, London Cancer), include:1,4,5,6,9
Biopsy confirmed skin cancer
A non-healing keratinising or crusted tumour > 1cm with significant induration on palpation
Skin lesions suggestive of skin cancer
Persistent or slowly evolving unresponsive undiagnosed skin conditions
A rapidly growing tumour
A lesion with poorly defined clinical margins
Pain/dysaesthesia associated with a lesion
An organ transplant recipient who develops new or growing cutaneous lesions
High levels of cumulative psoralen plus UVA photochemotherapy.
Treatment 10,11
Three main factors influence treatment:1
Complete removal or destruction of the primary tumour, preferably through histological assessment
Removal of local ‘in transit’ metastases
Removal of tumour positive lymph nodes by regional node dissection (beyond the scope of this update).
Surgical excision1,5
For clinically well-defined, low risk tumours less than 2cm in diameter, surgical excision with a minimum 4mm margin around the tumour border is appropriate and would be expected to completely remove the primary tumour mass in 95% of cases. (Strength of Recommendation A, Quality of Evidence IIiii). In order to maintain the same degree of confidence of adequate excision, tumours > 2cm in diameter, tumours classified as moderately, poorly or undifferentiated, tumours extending into the subcutaneous tissue and those on the ear, lip, scalp, eyelids or nose should be removed with a wider margin, of 6mm or more (see Figure 6).
Mohs’ micrographic surgery is advocated where it is critical to obtain a clear margin while preserving the maximum amount of normal surrounding tissue. (Strength of Recommendation B, Quality of Evidence II-iii). Prophylactic lymph node dissection has been proposed for SCC on the lip > 6 mm in depth and cutaneous SCC > 8mm in depth (Strength of Recommendation C, Quality of Evidence II-iii).
Figure 6. Large lip SCC required complex reconstruction with an advancement rotation flap(click to enlarge)
Radiotherapy1,4
Radiotherapy has the following roles:
• Surgery not possible
• Incomplete excision
• Advanced inoperable disease
• Palliative
• Adjuvant in extracapsular nodal disease.
The cure rates are over 90% for most skin lesions, but the same area cannot be treated twice. The decision to treat with radiotherapy should be made in a multidisciplinary setting.
Other treatments
Topical treatment,1,7 photodynamic therapy (PDT),13 cryotherapy/cryosurgery,1,12 curettage and cautery6 are only suitable for small in situ SCCs (Bowen’s disease) and pre-cancerous lesions (actinic keratoses), and are not suitable for invasive CSCCs. The significant disadvantage is lack of histological assessment. If in doubt, histological assessment of any lesions suspicious for CSCC should be performed.
Prognosis
The overall rate of cutaneous SCC metastasis is low (< 5%),9 but where distant metastases are present, the five-year survival rate is poor at around 25-40%.9 Up to 95% of metastases and local recurrences are detected within five years of initial treatment, with 70-90% occurring within the first two years.14
Follow-up
Follow-up should be determined by patient factors and whether the lesion is high or low risk. Some 75% of local recurrences and metastases are detected within two years and 95% within five years.1
All current guidelines recommend patient self-examination of the surgical scar site, local skin and lymph nodes. Instructions to this regard should be both verbal and written.
According to the SIGN guideline:9
Low risk lesions where there is a small solitary tumour with clear margins and no high-risk features on the pathology report, follow up may be unnecessary,9 patients should be offered a review appointment to check histopathology (if not previously assessed) and conduct skin surveillance
High-risk lesions should be offered follow-up appointments every three to six months for 24 months following treatment. One further appointment at three years may be appropriate depending on the clinical risk.
Patients who are immunosuppressed and those who are developing multiple SCC should be offered long-term follow up.
Ongoing follow up may be undertaken by an appropriately trained general practitioner with a specialist interest in dermatology or by a clinical nurse specialist.
Current guidelines
The current guidelines used by Plastics Surgery and Dermatology include the British Association of Dermatologists (2009) and the Scottish Intercollegiate Guidelines Network – SIGN (June 2014). Both are available in printed format, online publication and the SIGN guidelines are available as an Apple and an Android App.
Conclusion
With the increasing incidence of primary cutaneous SCC avoiding sun exposure is the key to prevention. Secondary prevention by early detection, referral and effective management is also very important. This update aims to outline the current recommendations with regards to diagnosis, investigation, referral, treatment and prognosis of CSCCs and to highlight high risk tumours with the potential to metastasise.
References
Multi-professional guidelines for the management of the patient with primary cutaneous squamous cell carcinoma; British Association of Dermatologists (2009)
Cancer Projection for Ireland 2014-2015, National Cancer Registry
Marks R. Squamous cell carcinoma. Lancet 1996; 347: 735-38.
Referral for suspected cancer; NICE Clinical Guideline (2005)
Guidelines for the treatment and referral of SCC of the Skin, Version 1.0, London Cancer Guidelines (2013)
Improving Outcomes for People with Skin Tumours including Melanoma (update): The Management of Low-risk Basal Cell Carcinomas in the Community; NICE (2010)
www.medicines.ie
Guidelines for the diagnosis and treatment of cutaneous squamous cell carcinoma and precursor lesions. French Dermatology Association. Published 2011.
Lansbury L, Leonardi-Bee J, Perkins W, et al; Interventions for non- metastatic squamous cell carcinoma of the skin. Cochrane Database Syst Rev. 2010 Apr 14;(4):CD007869.
Lansbury L, Bath-Hextall F, Perkins W, et al; Interventions for non- metastatic squamous cell carcinoma of the skin: systematic review and pooled analysis of observational studies. BMJ. 2013 Nov 4;347:f6153. doi: 10.1136/bmj.f6153.
Kuflik EG. Cryosurgery for skin cancer: 30 year experience and cure rates. Dermatol Surg 2004; 30: 297-300.
Photodynamic therapy for non-melanoma skin tumours (including premalignant and primary non-metastatic skin lesions); NICE Interventional Procedures, February 2006
Firnhaber JM; Diagnosis and treatment of Basal cell and squamous cell carcinoma. Am Fam Physician. 2012 Jul 15;86(2):161-8
 Figure 1. Rapidly growing scalp SCC in a RTR one year post-transplant, the patient had a small area of keratosis prior to his transplant that had rapidly developed on immunosuppression. He required a skin graft at excision(click to enlarge)
Figure 1. Rapidly growing scalp SCC in a RTR one year post-transplant, the patient had a small area of keratosis prior to his transplant that had rapidly developed on immunosuppression. He required a skin graft at excision(click to enlarge)