Quality of prescribing on an acute psychiatric inpatient unit
Serial audit and feedback aimed to improve the quality of prescribing in an acute psychiatric inpatient setting
Dr Melissa Gill, Senior Registrar in General Adult Psychiatry, Cavan/Monaghan Mental Health Services, Cavan/Monaghan, Dr Hisham Khider, SHO in Psychiatry, St Bridgid's Hospital, Ardee, Co Louth, Dr Yvonne Ryan, GP Registrar, St Bridgid's Hospital, Ardee, Co Louth, Dr MacDara McCauley, Consultant Psychiatrist in General Adult Psychiatry, St Bridgid's Hospital, Ardee, Co Louth and Dr Haider Hussain, SHO in Psychiatry, St Bridgid's Hospital, Ardee, Co Louth
Poor prescribing is recognised as one of the leading causes of medication error and adverse events.1,2,3 Indeed, the US Institute of Medicine report, To Err is Human: Building a Safer Health System,4 noted that medication error-linked deaths ranked above those due to road traffic accidents, breast cancer and AIDS. Misinterpretation of handwritten prescriptions is an important and potentially avoidable cause of errors. Missing information and ambiguous abbreviations may also contribute.5,6 It is recommended that active interventions to reduce prescribing errors should be employed, with education and training of staff at the forefront of these.6
Didactic sessions and passive dissemination of guidelines have been found to be ineffective in improving prescription quality, however.7 While audit itself is unlikely to alter prescriber behaviour, serial audits combined with feedback improve prescription quality in inpatient hospital settings.3,7,8
Aims
This study aimed to improve the quality of prescribing practices on an acute psychiatric inpatient unit by combining serial audit with feedback.
Methods
There exists a lack of national or international gold standards in prescription writing guidelines for inpatients.9 As such, a resource such as the BNF10 can inform local guidelines. A local protocol was drawn up using this resource. An audit template was created with 12 variables attributed to good prescribing practice. The protocol included that :
Prescriptions on inpatient medication sheets should be written legibly in ink, with the patient’s name, date of birth and allergy status clearly recorded
Medication names should be written in generic form and capitalised
Dosage, frequency and times of administration should be documented
If a medication is discontinued, this should be clearly indicated by crossing it off and recording the date of discontinuation
Finally, each medication should be signed by the prescribing doctor and their Medical Council number documented.
Medication prescription sheets for each inpatient on the acute unit were examined at each audit. The first audit was carried out in November 2012, the second in December 2012, the third in December 2013, the fourth in February 2014 and the most recent in June 2014. Feedback was given in a group educational setting after the first, third and fourth audit.
Results
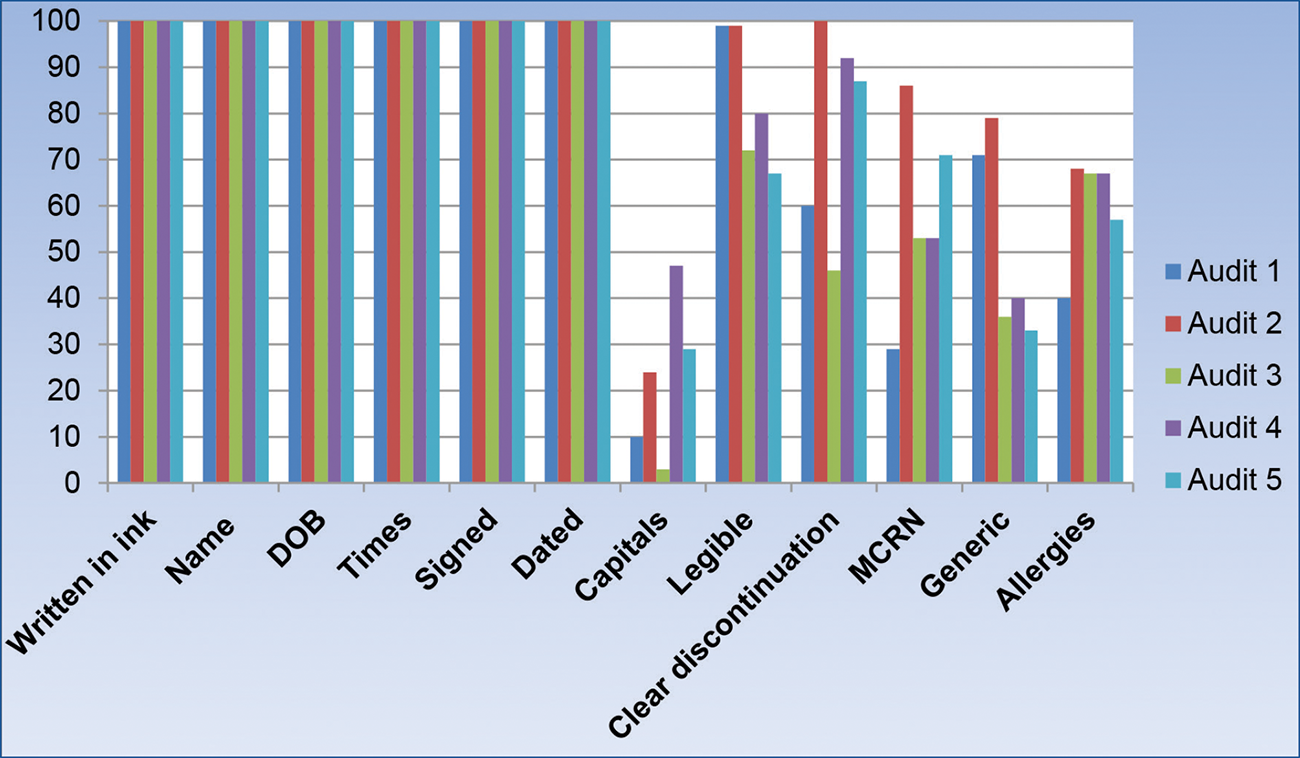
Figure 1: Prescribing audit results (shown in percentages)(click to enlarge)
100% of medication sheets were written in ink, with the name, date of birth, dosage and times of administration documented. This finding was consistent throughout the audit process. 100% of prescriptions were also consistently signed and dated.
Quality indicators such as prescribing in capital letters, legibility and clear discontinuation improved immediately after the first feedback session, but this improvement was not sustained when re-audited after one year. The second feedback session also failed to have an impact on improving these parameters, with all having deteriorated between the third and fourth audit despite the feedback session.
Prescribing in capital letters was the worst performing parameter, with fewer than 50% of prescriptions consistently being capitalised.
Documentation of Medical Council registration numbers and generic prescribing consistently fell below the audit standard expected of 100%, although documentation of the former improved after each feedback session.
While documentation of drug allergy status improved after the first audit feedback, it remained consistently below 70%, which was worrying below the audit standard.
Conclusion
Audit and feedback improved the quality of prescribing after the first feedback session, but not the second. Reasons for this are unclear. Attendance at the weekly educational session is affected by factors such as doctors’ leave entitlements and urgent clinical duties. For improvements to be sustained, feedback is likely to be needed more frequently than every six months.
The arrival of new medical staff every six months poses a challenge in terms of consistency of quality prescribing. It may also present an opportunity for educational feedback during induction sessions in relation to standards expected. These induction sessions alone are insufficient for improvements in prescribing practices and so frequent feedback, with repeat sessions for those absent initially, is recommended.
Subjectivity in terms of assessing legibility may account for the deterioration in this quality parameter, with different assessors estimating this. A consistent assessor, permanently employed in the hospital, may avoid potential differences in assessment of legibility.
The parameter of most concern in terms of its omission is that of allergy status. Potentially catastrophic consequences could arise as a result of failure to document a medication allergy.
Unnecessary adverse events can be avoided by accurately documenting any known allergies on admission to hospital.11 This represents a potentially avoidable medical error.
This audit cycle showed that although it has previously been found that serial audit and feedback can improve prescribing practices, this may not always be successful and may depend on multiple factors. The authors recommend increasing the frequency of feedback in order to capture as many prescribers as possible. In addition, consideration should be given to varying the setting in which feedback is given so as not to avoid feedback fatigue.
References
Dickens G. Inpatient psychiatry: three methods to detect medication errors. Nurse Prescr 2007; 5(4):167-71
White CS. Advanced practice prescribing: issues and strategies in preventing medication error. J Nurs Law 2011; 14(3&4):120-7
Gommans J, McIntosh P, Bee S, Allan W. Improving the quality of written prescriptions in a general hospital: the influence of 10 years of serial audits and targeted interventions. Intern Med J 2008; 38:243-8
Institute of Medicine. To err is human: Building a safer health system. Kohn L, Corrigan J, Donaldson M, editors. Washington, DC: National Academy Press; 1999
Lesar T, Bryceland L, Stein D. Factors related to errors in medication prescribing. J Am Med Assoc 1997; 277:312-7
Velo GP, Minuz P. Medication errors: prescribing faults and prescription errors. Br J Clin Pharmacol 2009; 67(6):624-8
Gray J. Changing physician prescribing behaviour. Can J Clin Pharmacol 2006; 13(1):e81-e84
Relihan E, Harbison J, Silke B, Ryder S. Audit and feedback to improve the quality of prescription writing. Int J Clin Pharm [Internet] 2012; 34(1):256. Available from: www.springerlink.com/content/0160679634101l12/fulltext.pdf
Kripalani M, Badanapuram R, Bell A. Audit on inpatient prescription writing guidelines. J Psychiatr Ment Health Nurs 2007; 14:598–600
British National Formulary. 66th ed. London: British Medical Association and the Royal Pharmaceutical Society of Great Britain; 2013
Khalil H, Leversha A, Khalil V. Drug allergy documentation – time for a change? Int J Clin Pharm 2011; 33(4):610-3
 Figure 1: Prescribing audit results (shown in percentages)(click to enlarge)
Figure 1: Prescribing audit results (shown in percentages)(click to enlarge)