Patient-specific rehabilitation is required to prevent long-term physical and cognitive consequences of stroke
Dr Linda Brewer, Clinical Research Fellow, Royal College of Surgeons in Ireland, Dublin and Prof David Williams, Consultant in Stroke Medicine, Beaumont Hospital and Royal College of Surgeons in Ireland, Dublin
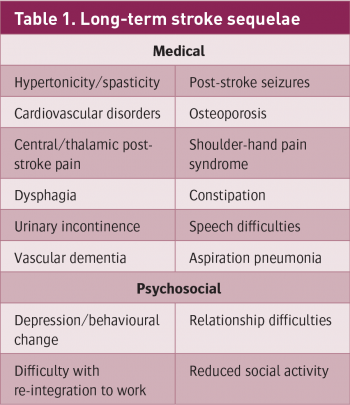
Stroke is the most common cause of long-term adult disability in Europe.1 Approximately 10,000 people have a stroke each year in Ireland, with at least 30,000 people alive having survived a stroke. A substantial proportion of these patients are left with significant residual disability, including hemiparesis in almost one-half of patients.2 Consequently, one of the greatest health effects for patients, their families and the economy results from the long-term physical and cognitive consequences of stroke (see Table 1). With an ageing population, the incidence of stroke is expected to rise. The Cost of Stroke in Ireland (COSI) report forecasts a 50% increase in stroke incidence and a 50% increase in the overall cost of stroke to the economy by 2021.3
(click to enlarge)
(click to enlarge)
A large proportion of the focus of stroke research still remains on the acute management of stroke. Significant progress has occurred in recent years, including the more widespread use of thrombolytic therapy and the reduction in early post-stroke complications due to the development of stroke units. However, with a high incidence of residual disability among stroke survivors, neuro-rehabilitation remains one of the cornerstones of post-stroke treatment. It plays a central role in successfully reducing the long-term effects of stroke and achieving optimal functional recovery for community integration.
Although recovery varies among stroke patients, studies have suggested that functional recovery is predictable in the first days after stroke4,5 and that long-term survival can be predicted by functional outcome at six months. The evidence base for stroke rehabilitation continues to grow. This includes the study of novel therapies and techniques, which may influence stroke rehabilitation practice and policy in the future.
The effects of stroke
As most patients with stroke survive the initial period, the greatest long-term effect is development of impairment, disability (limitations of activities) and handicap (reduced participation). The long-term effect of stroke is determined by the site and size of the initial stroke lesion and by the extent of subsequent recovery.6 Stroke recovery is heterogeneous and complex and probably occurs through a combination of spontaneous and learning-dependent processes.4 (see Table 2)
Stroke can result in a large variety of symptoms and signs (see Table 3) but the most common and widely recognised impairment caused by stroke is motor impairment. This can be regarded as a loss or limitation of function in muscle control or movement or a limitation in mobility.7 Motor impairment after stroke typically affects the control of movement of the face, arm and leg of one side of the body and affects about 80% of patients.
The focus of stroke rehabilitation is largely on the recovery of impaired movement and function in an effort to reduce disability and encourage participation in everyday activities.
(click to enlarge)
(click to enlarge)
(click to enlarge)
Stroke scales
It is becoming increasingly important to assess the effects of disease on quality of life. Stroke scales are useful tools for measurement of impairment and disability after stroke. The National Institutes of Health Stroke Scale (NIHSS) measures general stroke impairment and is useful for both clinical and research purposes. Scales to measure specific types of deficits have also been developed and validated in patients with stroke (eg. the Berg Balance Scale, the Rivermead Mobility Index and the Frenchay Aphasia Screening Test).
The Barthel Index (BI) and modified Rankin Scales (mRS) are the most widely used measures of stroke-related disability and handicap, respectively, and the mRS is frequently used as a global measure of the functional impact of stroke (see Table 4). Health-related quality of life (HRQOL) may be measured using a stroke-specific instrument such as the Stroke Impact Scale (SIS). Stroke scales are widely used by therapists in clinical practice to measure neurological deficits, to communicate these deficits to multidisciplinary team (MDT) colleagues and to monitor progress during therapy.
Figure 1: There is substantial evidence in support of the MDT for effective delivery of stroke rehabilitation(click to enlarge)
Figure 2: The cyclical process involving assessment, goal setting, intervention and reassessment is typical of stroke rehabilitation(click to enlarge)
Principles of stroke rehabilitation
Rehabilitation is a dynamic process with the overall aim of reducing stroke-related disability. There is substantial evidence in support of the MDT (see Figure 1) for effective delivery of stroke rehabilitation.8,9 MDTs provide an organised package of care co-ordinated through regular team meetings to discuss patient assessments and progress and to review future goals. This cyclical process involving assessment, goal-setting, intervention and reassessment is typical of stroke rehabilitation10 (see Figure 2). Involvement of the patient (and carer) in patient-centred interdisciplinary goal-setting has been shown to encourage patient motivation and engagement in therapy and is associated with better rehabilitation outcomes.
There is strong evidence to show that task-oriented and context-oriented training can assist the natural pattern of functional recovery.4,11 This is driven mainly by adaptive strategies that compensate for impaired body functions. By creating specific learning situations in stroke recovery, neural plasticity is promoted. Training should be targeted to goals that are relevant for the needs of the patient and, if possible, should be given in the patient’s own environment. Training should begin as soon as possible after stroke at an increased level of intensity, as tolerated by the patient. Recovery may continue well beyond the period of formal rehabilitation – for months or years after stroke. Motivation and self-management may help patients to continue their training on discharge from formal rehabilitation services.
Systems of rehabilitative care after stroke
Inpatient care
Rehabilitation is commenced as soon as possible after stroke. This usually occurs once the patient is stable, following acute stroke management. Evidence strongly supports an organised specialist system of care for stroke patients. On admission to hospital all patients with stroke should be transferred to a stroke unit.
A Cochrane review8 from 2007 of 31 trials (n = 6,936) confirmed the benefits of organised specialist care for patients with stroke. Compared with generic care on a general ward the number needed to treat in a specialist unit was 22 to prevent one death and 16 to prevent one patient losing their independence.
This compares very favourably with other interventions for stroke. This benefit applies to all ages, stroke subtypes and severities and has persisted in studies with longer follow-up periods. Care in stroke units is also cost-effective. Many countries are now moving towards a system involving direct admission of patients with acute stroke to a stroke unit instead of to general wards. One essential component in the success of stroke unit care is the involvement of an MDT with a specialist interest in stroke (see Table 5). On discharge from the stroke unit, patients with persistent neurological deficits may continue an inpatient rehabilitation programme, either within the acute hospital or in a separate rehabilitation facility. On discharge home, they may be referred for ongoing therapy in an ambulatory setting.
Outpatient care
Stroke patients are discharged from hospital when medically and functionally able to return to their home. This decision is individualised for each patient based on their neurological deficits, suitability of their home environment and availability of carer support. If required, ongoing rehabilitation may continue after discharge, either in hospital (outpatient or day hospital setting) or in the patient’s home through community rehabilitation teams. The location where these services are best provided is still unclear.
For suitable patients, early discharge from hospital with a programme of rehabilitation provided by an MDT at home is an alternative. Early supported discharge (ESD) services have been available in the UK and Scandinavian countries for some years and reviews of this type of service have been positive.9,12 ESD results in patients returning home earlier with less need for long-term institutional care and an increased likelihood of regaining independence in daily activities. For successful outcomes, these services should be offered to suitable patients only (medically stable with mild-to-moderate disability) and be provided by well co-ordinated MDTs who meet regularly. Ongoing medical input is also important to manage any medical complications following ESD.
Future novel therapies in stroke rehabilitation
Trials are under way to evaluate several novel therapies to enhance neural plasticity, which may be used in conjunction with task-specific training in the future. Examples include:
Stem-cell therapy
Repetitive transcranial magnetic stimulation
Motor imagery
Virtual reality
Robotic therapies
Drug augmentation of exercise training.
To date, the effect of these interventions on functional recovery is unknown, but it is likely that their usefulness in the real world will emerge over time.
Stroke rehabilitation in Ireland and the future
The COSI3 report indicated that less than €7 million per annum is being spent on stroke survivors in Ireland, an average spend of just over €200 per person (the rough equivalent of a single session of physiotherapy per year for each patient).
INASC2 data demonstrated considerable deficiencies in timely access to rehabilitation therapists in hospital. It also suggested that community-based rehabilitation was inadequate and described a range of barriers to the development of multidisciplinary team services, including the absence of a strategic plan, funding and staff employment.
Action on Secondary Prevention Interventions and Rehabilitation in Stroke (ASPIRE-S) is a research study, funded by the Health Research Board of Ireland and conducted by a team of researchers based at Royal College of Surgeons in Ireland. It is currently underway in north Dublin and will assess secondary prevention and rehabilitation care of community-discharged patients six months after their stroke.
Data from this study will allow identification of gaps between service need and provision and will help to guide the future allocation of resources. This will allow a more strategic approach to stroke care, including secondary prevention, both locally and nationally, in Ireland.
Key points to remember
Stroke is a common and disabling global health problem.
Well organised neuro-rehabilitation following stroke is key in regaining optimal function.
Goals should be patient-centred and training should be task and context specific for each patient.
Rehabilitation should begin as soon as possible after stroke at the highest level of intensity tolerated by the patient.
Early supported discharge services offer an effective alternative to ongoing inpatient rehabilitation.
References
Truelsen T, Piechowsji-Jozwiak B, Bonita R et al. Stroke incidence and prevalence in Europe: a review of available data. Eur J Neurol 2006; 13: 581-598
Irish Heart Foundation. National Audit of Stroke Care, Dublin, 2008
Irish Heart Foundation. Cost of stroke in Ireland. Estimating the annual economic cost of stroke and transient ischaemic attack (TIA) in Ireland. Report 2010.
Kwakkel G, Kollen B, Linderman E. Understanding the pattern of functional recovery after stroke: facts and theories. Restor Neurol Neurosci 2004; 22: 281-299
Nijland R, van Wegen E, Verbunt J et al. A comparison of two validated tests for upper limb function after stroke: the Wolf Motor Function Test and the Action Research Arm Test. J Rehabil Med 2010; 42: 694-696
Wade D. Measurement in neurological rehabilitation, Oxford University Press, Oxford, 1992
Stroke Unit Trialists’ Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database Sys Rev 2007; 4: CD000197
Early Supported Discharge Trialists. Services for reducing duration of hospital care for acute stroke patients. Cochrane Database Syst Rev 2005; 2: CD000443
Warlow CP, van Gijn J, Dennis MS et al. Stroke: practical management, 3rd edn. Oxford: Blackwell Publishing, 2008.
Murphy TH, Corbett D. plasticity during stroke recovery: from synapse to behaviour. Nat Rev Neurosci 2009;10: 861-872
Brewer L, Williams D. A review of Early Supported Discharge after Stroke. Rev Clin Gerontol 2010; 20: 1-11
 (click to enlarge)
(click to enlarge)





