This is the authors report the case of a 58-year-old man, who has been on adalimumab for psoriasis for the past three years. A nonsmoker, he presented with a five-month history of dry cough, night sweats and pleuritic chest pain.
Chest X-ray followed by CT thorax showed thoracic lymphadenopathy together with ground glass opacities bilaterally.
Transbronchial biopsy of the right lower lobe confirm presence of non-necrotising granuloma consistent with sarcoid.
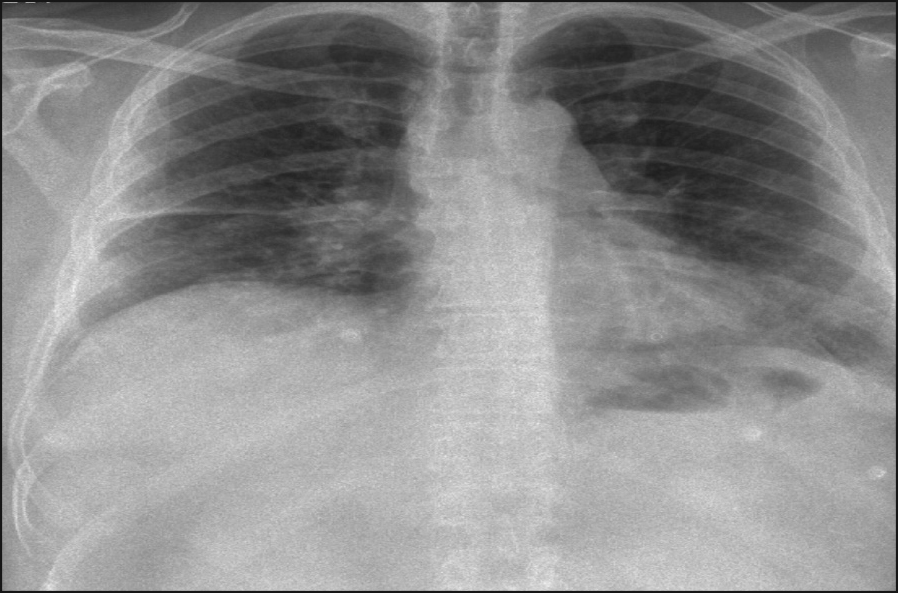
Figure 1. Bilateral lymphadenopathy with left basal infiltrate(click to enlarge)
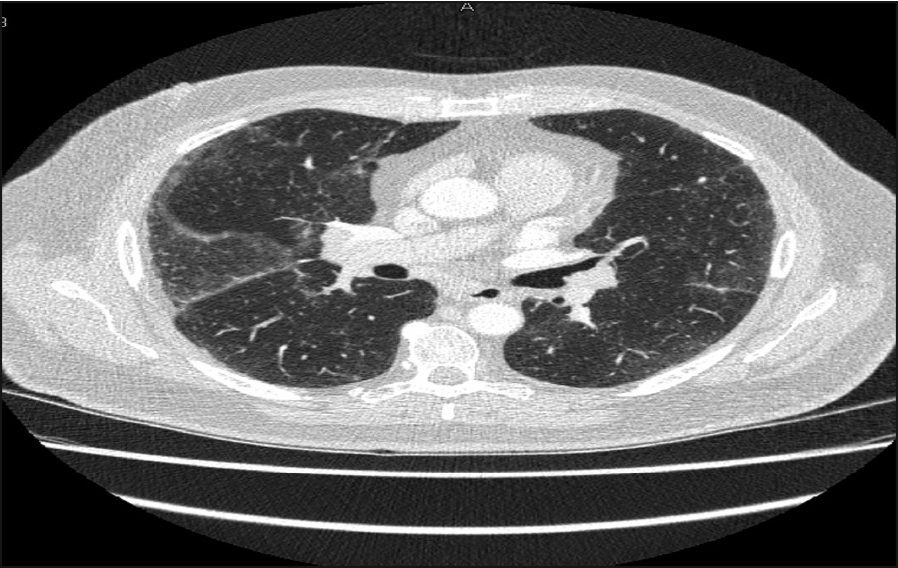
Figure 2. Bilateral ground glass opacities(click to enlarge)
Case report
The patient was diagnosed in 1994 and started on adalimumab three years ago.
He also has a past history of cutaneous lymphoma (in remission) and is being followed up by the oncology team. His other past medical histories include type 2 diabetes, renal stones and a traumatic intracranial bleed post-fall in 2006 and hypothyroidism.
He presented to the emergency department in May 2013 with a five-month history of dry cough, left pleuritic chest pain, night sweats and nausea.
On examination he was apyrexial, pulse 116, BP- 170/99, RR-18, no cervical lymphadenopathy, heart sound normal with no murmur or added sound, bibasal crackles on auscultation of the chest, abdomen soft and non tender and no ankle swelling.
His full blood count (FBC), renal, liver profile and C-reactive protein (CRP) was normal but his D-dimer was elevated with arterial blood gas (ABG) on room air showing a PO2- 7.48, PCO2 -5.10, pH -7.42, HCO3 -25.
Chest x-ray showed bilateral hilar adenopathy with left basal infiltrates (see Figure 1).
His previous chest x-ray dating back to 2004 was normal. CT pulmonary angiogram (CTPA) did not show any pulmonary embolus, however it showed the presence of thoracic and abdominal lymphadenopathy.
Further investigation showed a normal angiotensin-converting enzyme (ACE), erythrocyte sedimentation rate (ESR)-19, negative anti-neutrophil cytoplasmic antibodies (ANCA), normal lactate dehydrogenase (LDH), negative quantiferon and negative rheumatoid factor, however, ANA was positive.
High resolution computed tomography (HRCT) also demonstrated ground glass opacity involving both lungs (see Figure 2). The man was then booked for a bronchoscopy, which showed inflamed airways but no endobronchial lesions.
However, transbronchial biopsies taken from the right lower lobe showed non-necrotising granuloma consistent with sarcoid.
Discussion
Sarcoidosis is a diagnosis of systemic inflammation characterised by non-caseating granulomas, made after other causes of granulomatoses are excluded. It principally affects the lungs and lymph nodes, but may involve any organs.1
Although exact aetiology remains unknown, it was thought to be driven by antigen-activated CD4+ T cells, especially of type-1 helper (Th-1) variety.
The main cytokines responsible for initiation and maintenance of granuloma are tumour necrosis factor-alpha (TNF-alpha, interferon-gamma and interleukin-22).
There are 30 case reports of TNF-alpha inhibitors being used to treat refractory sarcoidosis effectively.3 It is therefore somewhat surprising that such treatment would cause granulomatosis.
TNF-alpha is a pleomorphic cytokine with both immune and non-immune biological effects.
In the past decade, it has been used increasingly in the treatment of rheumatoid arthritis (RA), and numerous other related rheumatic diseases, as well as inflammatory bowel disease and psoriasis. There have been 34 cases of granulomatous disease associated with TNF inhibitor therapy.4 However, in almost all cases, discontinuation of the TNF inhibitors with or without a course of oral steroids led to resolution of symptoms and survival and this pattern of positive challenge-dechallenge provides the most compelling evidence of causality.5
The lung and surrounding lymph nodes were the areas most commonly affected. The average amount of time to resolution of symptoms after discontinuation of the drug was 5.2 months.4 The pathogenesis of development of granulomatous sarcoid-like disease with TNF inhibitors is suggested to extend beyond simple drug allergy. TNF is a factor in the initiation and maintenance of granuloma.
What could be the result of altered cytokine balance, increased interferon-alpha level, rebound TNF secretion, or even exposure to an infectious agent that stimulates the granulomatous process, or to a combination of these factors, secondary to TNF inhibitors therapy?
It is interesting to know that most case reports to date of sarcoidosis associated with TNF inhibitors occurred in patients being treated with etanercept,6 unlike in our case.
In conclusion, there are increasing reports of this phenomenon with TNF inhibitors therapy. Granuloma development should be considered when unexplained non-primary site manifestations develop in a patient whose primary site is well controlled.
The prognosis appears to be good upon withdrawal of treatment. However, there is still a lack of recommendation on how we should monitor these patients.
References
Iannuzzi M, Rybicki B, Teirstein A. Sarcoidosis medical progress. N Engl J Med 2007; 357: 2153-2165
Wyeth Australia Pty Ltd. Product information on enbrel(R) etanercept. January 2010
Keystone EC. The utility of tumour necrosis factor blockade in orphan diseases. Ann Rheum Dis 2004; 693(2): ii79-83
Cathcart S, Sami N, Elewski B. Sarcoidosis as an adverse effect of tumour necrosis factor inhibitors. Journal of drugs in dermatology 2012; 11(5)
Khasnis AA, Clabrese LH. Tumour necrosis factor inhibitors and lung disease: a paradox of efficacy and risk. Seminars in arthritis and rheumatism 2010; 40, 2, 147-163
Sweiss NJ, Baughman RP. Tumour necrosis factor inhibition in the treatment of refractory sarcoidosis: slaying the dragon? J Rheumatol 2007; 34(11): 21 29-31
 Figure 1. Bilateral lymphadenopathy with left basal infiltrate(click to enlarge)
Figure 1. Bilateral lymphadenopathy with left basal infiltrate(click to enlarge)