This case illustrates the impact of undiagnosed obstructive sleep apnoea (OSA) on the right chamber of the heart and on the cardiovascular system as a whole, with an emphasis on the need to be vigilant to avoid missing the diagnosis.
The case highlights the complex interplay between the respiratory and cardiovascular systems in disease states and the need to be more aware of sleep apnoea and its effects.
Figure 1: ECHO image of the patient's heart(click to enlarge)
Figure 2: ECHO image of the patient's heart(click to enlarge)
Man presents with arm pain and discomfort
A 43-year-old man presented to the acute medical unit with left arm pain and retrosternal discomfort.
He was moderately obese, hypercholesterolaemic, hypertensive and he did not smoke.
Initial evaluation showed:
His resting ECG was quite abnormal, showing pronounced T-wave inversion antero-laterally more so in the right ventricular leads
An urgent troponin was negative
He was hypertensive with BP 170/95 despite being on a β-blocker
Sats on RA 95%.
His initial physical examination was quite informative, revealing restricted cervical axial rotation to the left, restricted left shoulder movements and tenderness over C6, C7 and the left trapezius. This suggests a musculoskeletal/cervicogenic cause for his left arm pain.
In other regards it was quite unremarkable.
However, the examining physician was struck by his noisy breathing, nasal speech and that he appeared rather drowsy.
Investigations
CXR showed no obvious pathology.
Cervical x-ray was performed.
Degenerative changes and joint space narrowing at C4, C5 and C6 was noted.
An echocardiogram was performed.
Interestingly, the sonographer noted that the patient dozed off several times during examination.
ECHO revealed a hypertrophied and hypokinetic dilated right ventricle with marked trabeculations and evidence of pulmonary hypertension and right ventricular pressure overload. There was mild-to-moderate tricuspid regurgitation.
Left ventricular systolic function was preserved. There was moderate left ventricular hypertrophy and diastolic dysfunction. These findings were consistent with a history of sub-optimally controlled systemic hypertension. There was no significant left-sided valvular disease.
The quest for a unifying diagnosis
ECHO and electrocardiographic evidence of right ventricular dysfunction and pulmonary hypertension in an unusually somnolescent patient raised the possibility of obstructive sleep apnoea as a unifying diagnosis.
On further questioning the patient admitted to snoring heavily, unsatisfying sleep and episodes of daytime somnolence such as dozing off at traffic lights.
He also had several unresolved ENT conditions, such as enlarged tonsils, and had suffered from several bouts of sinusitis annually over the preceding two decades.
Evaluation, sub-specialist input and treatment
ENT
An ENT consult confirmed severe upper airway obstruction by hypertrophied tonsils and a prolapsed and chronically inflamed posterior nasopharyngeal wall. The posterior nasopharyngeal space was almost non-existent. He was commenced on intranasal steroids to diminish inflammation and will require corrective surgery.
Respiratory
The patient was assessed by a respiratory physician who agreed with our clinical assessment and made arrangements for urgent polysomnography, which confirmed the diagnosis of obstructive sleep apnoea and upper airway obstruction. He was provided with a CPAP device. This should alleviate his airway obstruction, diminish pulmonary hypertension and reduce his perioperative risk and act as a bridge to ENT surgery.
Coronary
Coronary angiography was performed and revealed minimal coronary artery disease. A right heart study was deferred.
BP
A 24-hour BP monitor confirmed poorly controlled hypertension. He was commenced on ARB, a statin, a calcium channel blocker and aspirin.
Holter monitor
He did not have a Holter monitor.
Diagnoses
Pulmonary hypertension and severe right ventricular dysfunction caused by obstructive sleep apnoea and severe upper airway obstruction.
Radiculopathic left arm pain and cervical spondylosis.
Follow-up
A month after commencing CPAP and nasal corticosteroids, he feels much better and admits to being less drowsy in the daytime, his blood pressure is well controlled and his lipid profile has improved.
He has been less successful at losing weight and his radicular arm pain is still bothersome.
He should have his ENT pre-operative assessment soon.
Discussion
Untreated OSA has significant cardiovascular effects and important implications on morbidity and mortality.
1. Pulmonary hypertension
Sleep apnoea can cause pulmonary hypertension which, over time, results in right ventricular hypertrophy dilatation and ultimately right heart failure as described above.
2. Systemic hypertension
OSA episodes are associated with adrenergic discharges and result over time in altered function of central and peripheral blood pressure control mechanisms. Patients with OSA frequently lack the normal nocturnal dip in systemic blood pressure and often have blood pressure that is harder to control. Treating OSA may improve BP control and diminish overall cardiovascular risk.
3. Atrial arrhythmias
Recently, sleep apnoea has been associated with increased frequency of arrhythmias, especially atrial arrhythmias.
With our increased understanding of the autonomic changes that occur during apnoeic episodes came the realisation that nocturnal hyperadrenergic states and episodes of desaturation in conjunction with atrial remodelling associated with raised pulmonary pressures may result in an increased incidence of paroxysmal atrial arrhythmias including atrial fibrillation. There have been suggestions that patients with predominantly nocturnal episodes of paroxysmal atrial fibrillation should be screened for sleep apnoea.
4. Neuro-endocrine effects
These may affect glucose and energy metabolism and mood.
5. ENT pathology as contributory factor
Despite its association with an increased BMI this often under-diagnosed condition may be present in patients without the classic ‘Pickwickian’ habitus in whom (as in this case) correctable ENT pathology may be a contributory factor.
Subtle and apparently unrelated clues such as fatigue, irritability and loss of concentration or more obvious ones such a deviated nasal septum or a history of previous facial trauma should not be ignored.
Conclusion
OSA is a perfectly treatable condition with significant health and socioeconomic implications for the patient ranging from cardiovascular implications as described above to increased accident proneness caused by excessive somnolence.
It is by no means benign, and every effort should be made not to miss the diagnosis. Its manifestations are subtle and presentations are often non-classical in non-obese patients.
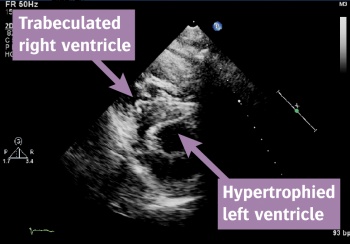 Figure 1: ECHO image of the patient's heart(click to enlarge)
Figure 1: ECHO image of the patient's heart(click to enlarge)
