Ulnar neuropathy after removal of contraceptive pill
A case of ulnar nerve neuropraxia after an attempted removal of a subdermal contraceptive implant is presented
Dr Louise Fitzgerald, Plastic Surgery SHO, Beaumont Hospital, Dublin, Dr Jeffrey CY Chan, Plastic Surgery SPR, Department of Plastic, Reconstructive and Hand Surgery, Beaumont Hospital, Dublin, Dr Laura Kearney, Plastic Surgery Registrar, Department of Plastic, Reconstructive and Hand Surgery, Beaumont Hospital, Dublin and Dr Nadeem Ajmal, Plastic Surgery Consultant, Department of Plastic, Reconstructive and Hand Surgery, Beaumont Hospital, Dublin
Implantable hormonal contraceptive devices are an effective, economical and convenient method of reversible long-term contraception. The insertion and subsequent removal are relatively uncomplicated once the upper arm anatomy is appreciated. While ulnar nerve injury has previously been described with Norplant, this has not been reported with Implanon. We present a case of a 30-year-old with ulnar nerve neuropraxia after an attempted removal of Implanon. We discuss the method of insertion and removal of the device, review the literature for reported cases of peripheral nerve injuries and recommended alternative insertion sites.
Case report
A 30-year-old right hand dominant woman was referred to our unit after her general practitioner attempted to remove the Implanon from the medial aspect of her left mid-arm. The patient presented with paraesthesia and clawing of her little and ring fingers. There was weakness of fingers abduction and adduction, and Froment’s sign was positive. Wartenberg’s sign was not present. The Implanon was not clinically palpable but there was minor bruising surrounding the incision.
An ultrasound scan revealed the location of the Implanon. Surgical exploration under general anaesthesia was performed to examine her ulnar nerve and to retrieve the implant which was found under the triceps muscle fascia intramuscularly. The ulnar nerve had a normal macroscopic appearance (see Figure 1) and was surrounded with rather unimpressive localised haematoma and muscle bruising, supporting a diagnosis of ulnar nerve neuropraxia. Her postoperative course was uneventful. Occupational therapy and physiotherapy were commenced to address clawing of her little and ring fingers. While motor function has now improved four months following surgery, her sensory symptoms have not subjectively improved.
Figure 1. The ulnar nerve had a normal macroscopic appearance and was surrounded with rather unimpressive localised haematoma and muscle bruising, supporting a diagnosis of ulnar nerve neuropraxia(click to enlarge)
Discussion
Anatomy10
The compact, dense brachial fascia encloses the muscles of the upper arm. The subcutaneous vessels, nerves, and the lymphatic vessels are vulnerable to damage in their superficial location. Ulnar nerve comes from the medial cord of the brachial plexus (C8-T1). In the arm it lies posteromedial to brachial artery in anterior compartment of upper half arm. It pierces the medial IM septum at the arcade of Struthers approximately 8cm from medial epicondyle and lies medial to the triceps. The arcade of Struthers is an aponeurotic band extending from the medial IM septum to the medial head of the triceps.
The ulnar nerve innervates the skin of the fifth digit and the medial half of the fourth digit, and the corresponding part of the palm. The ulnar nerve and its branches innervate muscles in the forearm and hand. Clinically, nerve injuries may lead to:
Motor deficit – characterised by a weakness in flexion of the hand at the wrist, loss of flexion of ulnar half of digits, or the 4th and 5th digits, loss of ability to cross the digits of the hand. The presence of a claw hand deformity when the hand is at rest is due to hyperextension of the fourth and fifth digits at the meta carpophalangeal joints and flexion at the interphalangeal joints.
Sensory deficit – loss of sensation or paraesthesia in ulnar half of the palm and dorsum of hand, and medial 1.5 digits on both palmar and dorsal aspects of the hand.
The device
Implanon is a single-rod contraceptive implant2 consisting of a core containing the selective progestin etonogestrel and ethylene vinyl acetate (EVA) copolymer surrounded by a rate-controlling EVA membrane. The rod is 40mm in length and 2mm in diameter. The reported incidence of complications from its insertion (0.3%) and removal (0.2%) is low.2,6
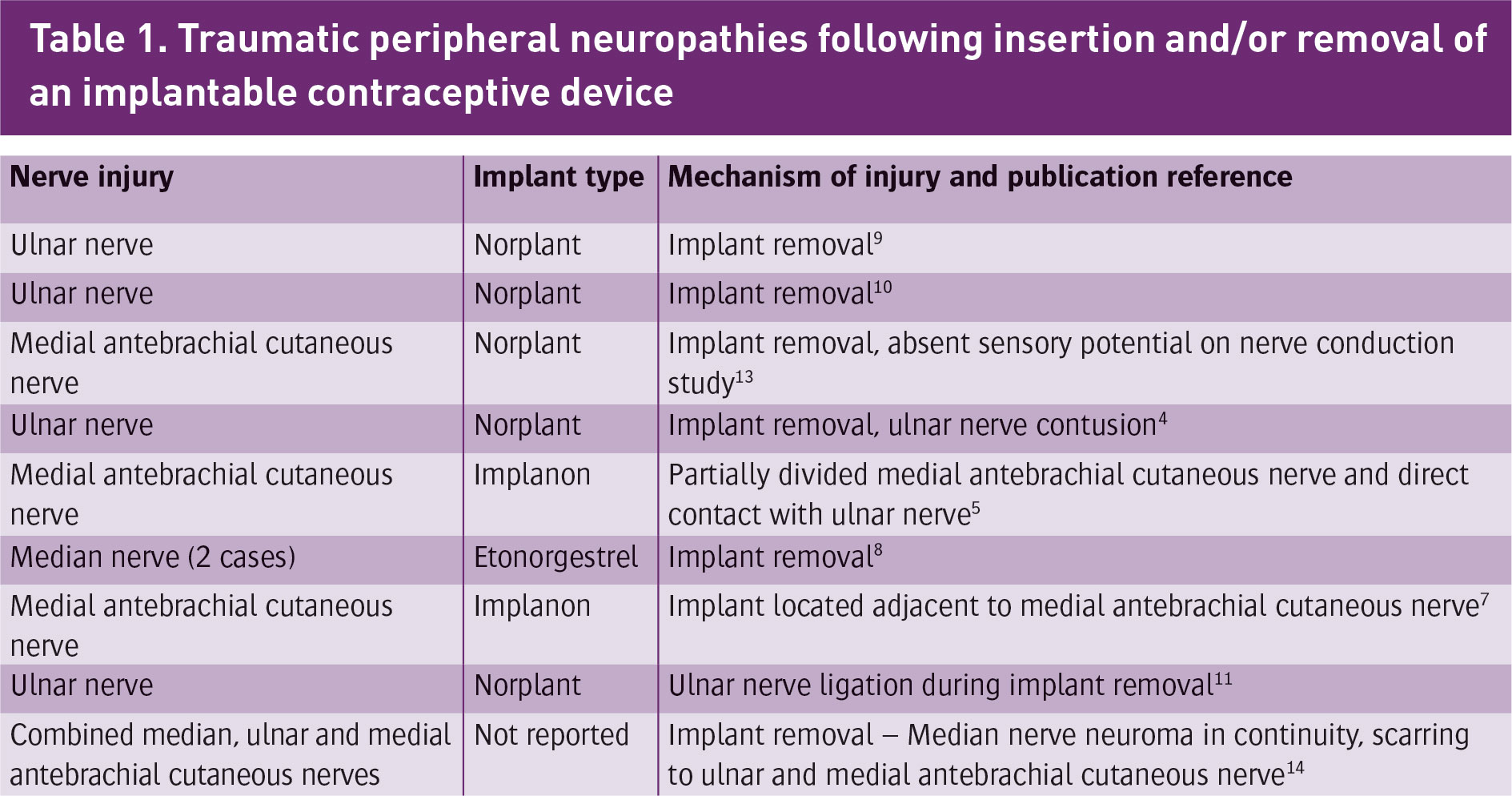
Injuries to peripheral nerves from insertion or removal of Implanon have been previously documented in the literature (Table 1) and have led to litigations.4,5 Wechselberger et al and Brown et al reported injuries to the medial cutaneous nerve of the forearm associated with Implanon.5,7 Spinner et al reported on a combined median, ulnar and medial antebrachial cutaneous nerves injuries, while Gilles et al reported two cases of median nerve injuries.8 Other authors had previously reported injuries to the ulnar nerve associated with Norplant.4,9,10,11 Norplant, an older generation of subdermal contraceptive implant, consisted of a set of six subdermal rods therefore proportionally increasing the size of implantation area and risk.
(click to enlarge)
Insertion and removal
The Implanon applicator facilitates the placement of the implant by keeping the needle in a superficial plane and permitting a withdrawal method of insertion.7 The manufacturer recommends the inner aspect of the non-dominant upper arm, approximately 8-10cm above the medial epicondyle of the humerus. After a maximum of three years, the removal of Implanon is performed under local anaesthetic through a longitudinal incision over the distal tip of the implant (2-3mm).3
The removal is performed either with the described ‘pop-out’ technique or a grasping method using a small curved sterile haemostat.3
Occasionally, the implant is not palpable, which is usually the result of incorrect insertion (or non-insertion), large amount of subcutaneous fat, migration or development of dense fibrous sheaths.6 Blind removal should not be attempted, ultrasound localisation and guided removal technique6,12 and magnetic resonance imaging (MRI) may also be appropriate where placed within the muscle or beneath the muscle fascia.6 If non-insertion is suspected, serum ENG levels could confirm whether the Implanon is in situ but does not localise it.6 Where an inadvertent injury to a nerve occurs an urgent plastic surgery opinion sought.
Consistent subcutaneous fat thickness and low rate of migration in the medial arm were factors that influence the choice of the medial arm as the desired site. Since the technique of insertion and removal of Implanon are essentially blind, the commonly chosen biceps-triceps groove is potentially the most hazardous site for the device due to proximity of neurovascular structures. The use of alternative sites has been previously suggested by other authors to prevent these avoidable nerve injuries. Bragg et al recommended the medial arm proximal to the midpoint of the humerus, the anteromedial aspect of the arm over the biceps or the deltoid area.4 These positions are anatomically safer but are cosmetically exposed and anecdotally may be associated with a higher incidence of fat atrophy and keloid scar.4 The median supraumbilical region, buttocks and lower limb have also been proposed but is associated with a higher risk of migration.4,5
Conclusion
Meticulous insertion technique and familiarity with the anatomy of the arm will minimise complications at the time of insertion and removal of subdermal contraceptive devices. Patients choosing to have this contraceptive method should be counselled regarding the higher risk of nerve injuries in the medial arm, against the potential aesthetic sequalae of fat atrophy and scarring in more exposed but safer alternative sites in the arm, and risk of implant migration in the abdomen or lower limb. When a non-palpable implant is encountered, radiological-guided removal techniques should be utilised to minimise complications and facilitate removal.
References
Darney PD. Implantable contraception. Eur J Contracept Reprod Health Care 2000;5(Suppl 2):2-11
Dunson TR et al. Complications and risk factors associated with the removal of Norplant implants. ObstetGynecol 1995;85:543-8
Mascarenhas L. Insertion and removal of Implanon. Eur J Contracept Reprod Health Care 2000;5(Suppl 2):29-34Bragg TWH, Jose RM, Bland JW, Matthews RN, Srivastava S. Implantable contraceptive devices: primum non nocere. J Fam Plann Reprod Health Care 2006; 32:190-192
Wechselberger G et al. Nerve injury caused by removal of an implantable hormonal contraceptive. Am J Obstet Gynecol 2006; 195:323-326
Management and localization strategies for the nonpalpable Implanon rod Lee P. Shulman, Contraception 73 (2006) 325-330
Brown et al. Neuropathy associated with etonogestrel implant insertion, Contraception 86 (2012) 591-593
Gillies R et al. Etonogestrel implants—case studies of median nerve injury following removal. Aust Fam Physician. 2011;40(10):799-800
Marin R, McMillian D. Ulnar neuropathy associated with subdermal contraceptive implant. Southern Med J 1998; 91:875-878
Smith JM, Conwit RA, Blumenthal PD. Ulnar nerve injury associated with removal of Norplant implants. Contraception 1998; 57:99-101
Adkinson et al, Ulnar nerve ligation after removal of Norplant: a case report, Hand (2013) 8:92–96 DOI 10.1007/s11552-012-9454-9
Persaud T, Walling M, Geoghegan T et al. Ultrasound-guided removal of Implanon devices. Eur Radiol 2008;18:2582-5
Nash C, Staunton T. Focal brachial cutaneous neuropathy associated with Norplant use: suggests careful consideration of the recommended site for inserting contraceptive implants. J Fam Plann Reprod Health Care 2001; 27:155-156
Robert J spinner et al. Major Nerve Injury after contraceptive implant removal: case illustration. J Neurosurgery 2015; DOI: 10.3171/2015.1.JNS142642
 Figure 1. The ulnar nerve had a normal macroscopic appearance and was surrounded with rather unimpressive localised haematoma and muscle bruising, supporting a diagnosis of ulnar nerve neuropraxia(click to enlarge)
Figure 1. The ulnar nerve had a normal macroscopic appearance and was surrounded with rather unimpressive localised haematoma and muscle bruising, supporting a diagnosis of ulnar nerve neuropraxia(click to enlarge)