An extremely rare case of dilated cardiomyopathy that presented as aortic coarctation in an adult patient highlights the need for thorough evaluation of patients with heart failure and hypertension
Dr Abdalla Ibrahim, Cardiology Registrar, Cork University Hospital, Cork, Dr Zahir Satti, Cardiology Registrar, Cork University Hospital, Cork and Dr Ronan Curtin, Consultant Cardiologist, Cork University Hospital, Cork
A 31-year-old male presents with a three-week history of a flu-like illness and symptoms of heart failure with severe global left ventricular dilation and dysfunction on transthoracic echocardiography (TTE) and ejection fraction of 25%. He has no past medical history apart from high blood pressure noted by GP one week prior to admission.
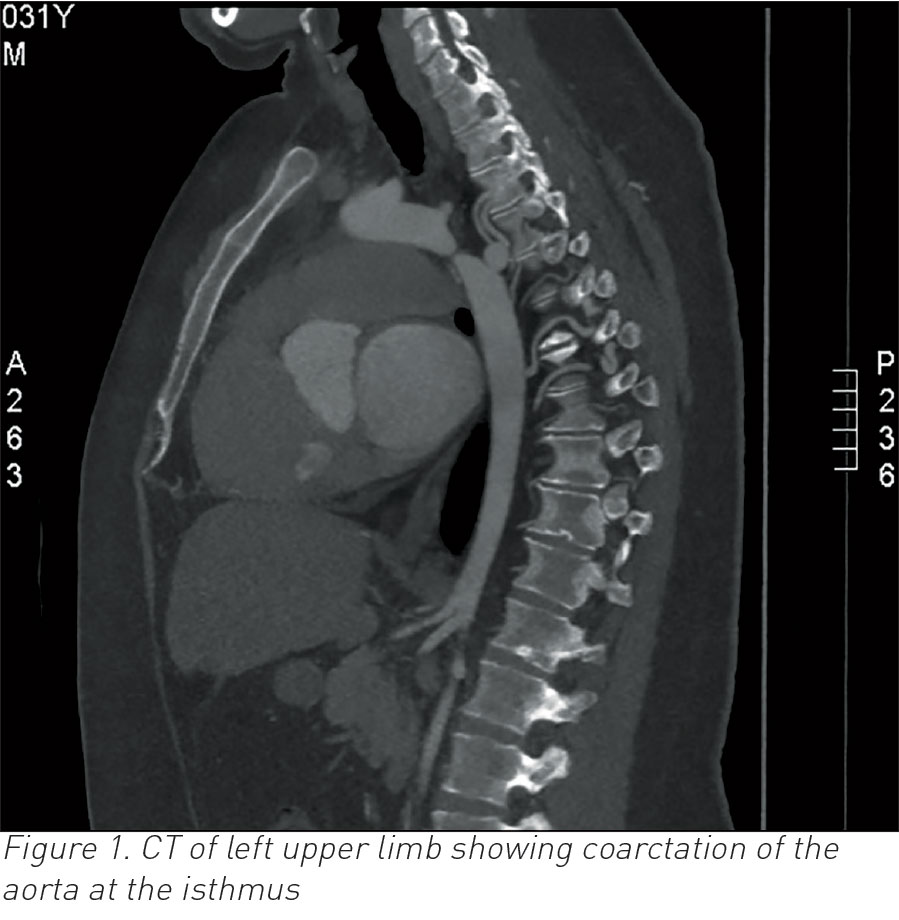
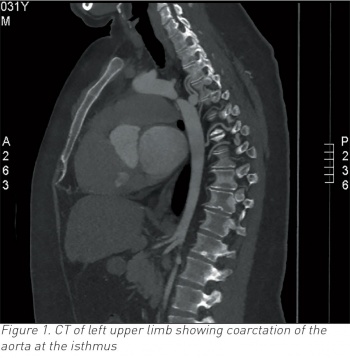
Two weeks following admission he complained of left arm pain and CT upper limb confirmed embolic occlusion of the left brachial artery and incidental severe coarctation of the proximal descending aorta after the origin of the left subclavian artery (see Figure 1).
(click to enlarge)
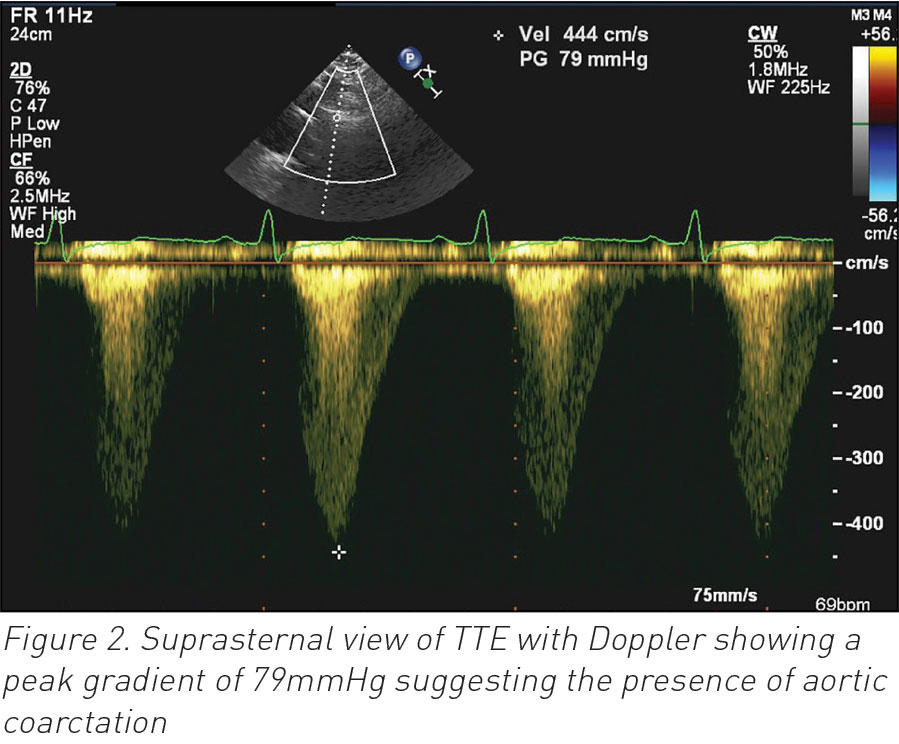
Follow up TTE suggested the presence of coarctation of the aorta on a suprasternal view which was not performed at the time of his first TTE (see Figure 2).
(click to enlarge)
His heart failure and blood pressure responded very well to medical therapy and he has been referred for surgical correction of his aortic coarctation.
Background
We report this case to emphasise the importance of thorough history and examination when evaluating patients, and to always consider all possible diagnoses including uncommon ones such as coarctation of the aorta.
This case also highlights the significance of a standardised approach when performing imaging studies. A suprasternal view was not performed during our patient’s first TTE study which could have suggested the underlying diagnosis earlier.
Case presentation
A 31-year-old male presented with dyspnoea on exertion NYHA class II, orthopnoea and lower limb oedema for three weeks. These symptoms were preceded by flu-like symptoms. He was also noted to be hypertensive by his GP a week prior to admission and was started on ramipril 5mg. He has no other significant past medical history apart from a high body mass index of 38. He consumed about 40 units of alcohol per week and has a positive family history of ischaemic heart disease (father and two grandfathers had myocardial infarction at the age of 50).
Examination revealed a blood pressure of 160/70mmHg, heart rate of 110 beats per minute, oxygen saturation of 97%, raised jugular venous pressure, bibasal crepitations, lower limb oedema and no cardiac murmurs. Radiofemoral delay was not checked during initial assessment but was detected following the result of the CT scan.
Investigations
ECG showed sinus tachycardia with left ventricular hypertrophy
High sensitivity troponin-T was 55ng/L (upper limit 14ng/L), no rise on serial testing
Chest x-ray showed marked cardiomegaly with a cardiothoracic ratio of 0.68 and pulmonary congestion but there was no rib notching
Echocardiogram showed severely dilated left ventricle (left ventricular internal dimension-diastole of 6.9cm) with severe global systolic dysfunction and moderate concentric left ventricular hypertrophy. Ejection fraction of 25-30%
CT left upper limb showed coarctation of the aorta at the isthmus (see Figure 1). The coarctation measures approximately 0.5-0.6cm, compared with 2.0cm in the distal arch and 2.7cm in the proximal descending and occlusion of the left brachial artery at the level of the distal third of the humerus.
Differential diagnosis
Hypertensive cardiomyopathy
Alcohol-induced cardiomyopathy
Myocarditis-induced cardiomyopathy
Treatment
The patient was treated with intravenous diuretics along with other usual heart failure measures. He also had emblectomy and anticoagulation for the upper limb ischaemia and was referred to vascular surgery for the intervention to his aortic coarctation.
Outcome and follow-up
The patient’s heart failure responded very well to treatment. He was diuresed 20kg and his blood pressure was adequately controlled. He also had successful embolectomy of his left brachial artery and was put on intravenous heparin and then oral anticoagulation with warfarin. He is on regular follow-up in the cardiology clinic and is awaiting surgical intervention for his aortic coarctation.
Discussion
In this report, we presented a case of aortic coarctation that remained undiagnosed until the development of congestive cardiac failure in adulthood.
Most cases of aortic coarctation are diagnosed in childhood due to the development of congestive cardiac failure or during adulthood due to treatment-refractory hypertension.
Dilated cardiomyopathy is a rare clinical presentation of coarctation of aorta in infants.1,2 One such case of dilated cardiomyopathy was reported by Agac et al in 2012. The patient was a 55-year-old man who presented with symptoms of recent-onset cardiac failure.3 The patient was successfully managed with stent implantation. Our patient, although stabilised at present, is still awaiting surgical intervention for correction of the coarctation at the time of preparation of this article.
More recently, another case of dilated cardiomyopathy secondary to aortic coarctation was reported; however, this patient had coarctation at an atypical location, namely the aortic arch.4 Our patient had the coarctation at the isthmus.
With regard to other symptoms at presentation, our patient also had newly diagnosed hypertension. However, during the initial evaluation his cardiac failure was attributed to the history of excessive alcohol consumption or possible myocarditis.
No single intervention is superior in minimising restenosis. The preferred technique is usually determined by the anatomy of the lesion and institutional experience but stent implantation has become the method of choice in adults in many centres.
Put together, our experience in this case highlights the need for the thorough evaluation of patients with heart failure and hypertension to rule out various causes of heart failure, including cardiomyopathy secondary to aortic coarctation. In conclusion, we presented an extremely rare case of dilated cardiomyopathy as a presentation of aortic coarctation in an adult patient. To the best of our knowledge, this appears to be only the third such case report in English literature.
Learning points
Coarctation of the aorta should always be considered in young adults with hypertension.
Patients with de novo acute heart failure should have careful evaluation to cover all possible underlying aetiologies, including hypertensive cardiomyopathy secondary to coarctation of the aorta.
All standard TTE views should be performed to ensure that pathology is not missed and to enable comparison with previous studies.
References
Hwang MS, Chu JJ, Chang YS, Su WJ. Dilated cardiomyopathy: an unusual presentation of aortic coarctation in an infant. Cardiology 2006; 106(1):56-58 [Epub 2006, Apr 10]
Wiegand G, Schlensak C, Hofbeck M. Pitfalls in Echocardiography: Coarctation of the Aorta Presenting as Dilated Cardiomyopathy (DCM). Ultraschall Med 2015(Jun 17) [Epub ahead of print]
Agaç MT, Acar Z, Akdemir R, Korkmaz L, Kiris A, Akyüz AR, Erkan H. Dilated cardiomyopathy secondary to coarctation of the aorta was completely resolved after stent implantation. Cardiovasc J Afr 2012(Jul 12); 23(6):e12-13 doi: 10.5830/CVJA-2011-061
Alsemgeest F, Kamp O, Marcu CB. Atypical aortic coarctation as a cause of a cardiomyopathy. Neth Heart J 2015(Jul); 23(7-8):381-382 doi: 10.1007/s12471-015-0716-3
 (click to enlarge)
(click to enlarge)