A case on the diagnosis and management of a small bowel obstruction
Dr Brian Cristopher, Specialist Registrar in Gastroenterology/Hepatology, Connolly Hospital, Blanchardstown and Dr Orlaith Kelly, Consultant Gastroentrologist, Department of Gastroenterology, Connolly Hospital, Blanchardstown, Dublin
A 45-year-old woman attended our care with chronic right iliac fossa pain, nausea and diarrhoea. She was admitted four months previously with respiratory symptoms and was treated for severe bilateral pneumonia and also conservatively treated for small bowel obstruction. Her clinical condition was critical at that point in time, she was intubated and managed in the intensive care unit. She had a previous history of retained placenta post-delivery and associated peritonitis and sepsis. She also had history of oophorectomy and salphingectomy in 1994. She previously had a history of small bowel obstruction with zone of transition at right iliac fossa, which subsequently resolved with conservative treatment.
A computed tomography (CT) of abdomen and pelvis performed showed zone of transition at distal ileum. Her inflammatory markers C-reactive protein (CRP) was raised and she was covered with antibiotic, piperacillin-tazobactam 4.5g tds intravenously. Her CRP was improving with albumin of 18g/dL (30 to 40). After a multidisciplinary meeting discussion, the plan was for ileo-colonscopy when she was clinically better.
Unfortunately, she developed worsening pain at her right iliac fossa and a trial of intravenous steroid was given. She did not respond to the steroids and her repeat imaging showed evidence of small bowel obstruction and perforation (see Figure 1). Emergency laparotomy was performed and this showed dilated small bowel to the level of mid distal ileum. A stricture of small bowel was seen 40cm from ileocaecal valve with evidence of tiny perforations at ileum. Approximately 120cm in length of small bowel was resected (see Figure 2). The histology was consistent with a diagnosis of Crohn’s colitis, with fissuring ulcer and scarring of small bowel mucosa and transmural inflammation (see Figure 3). An anti-tumour necrosis factor (anti-TNF) blood screen was sent. She continued to have unremarkable post-operative recovery with nutritional support and engagement with physio-therapist. She was reviewed eight weeks later and was initiated on infliximab infusion.
Figure 1. CT abdomen/pelvis shows distended loops of mid small bowel (SB) with a transition from distended SB to normally distended SB and a transition from normally distended sb to collapsed bowel more inferiorly. Findings consistent with small bowel obstruction(click to enlarge)
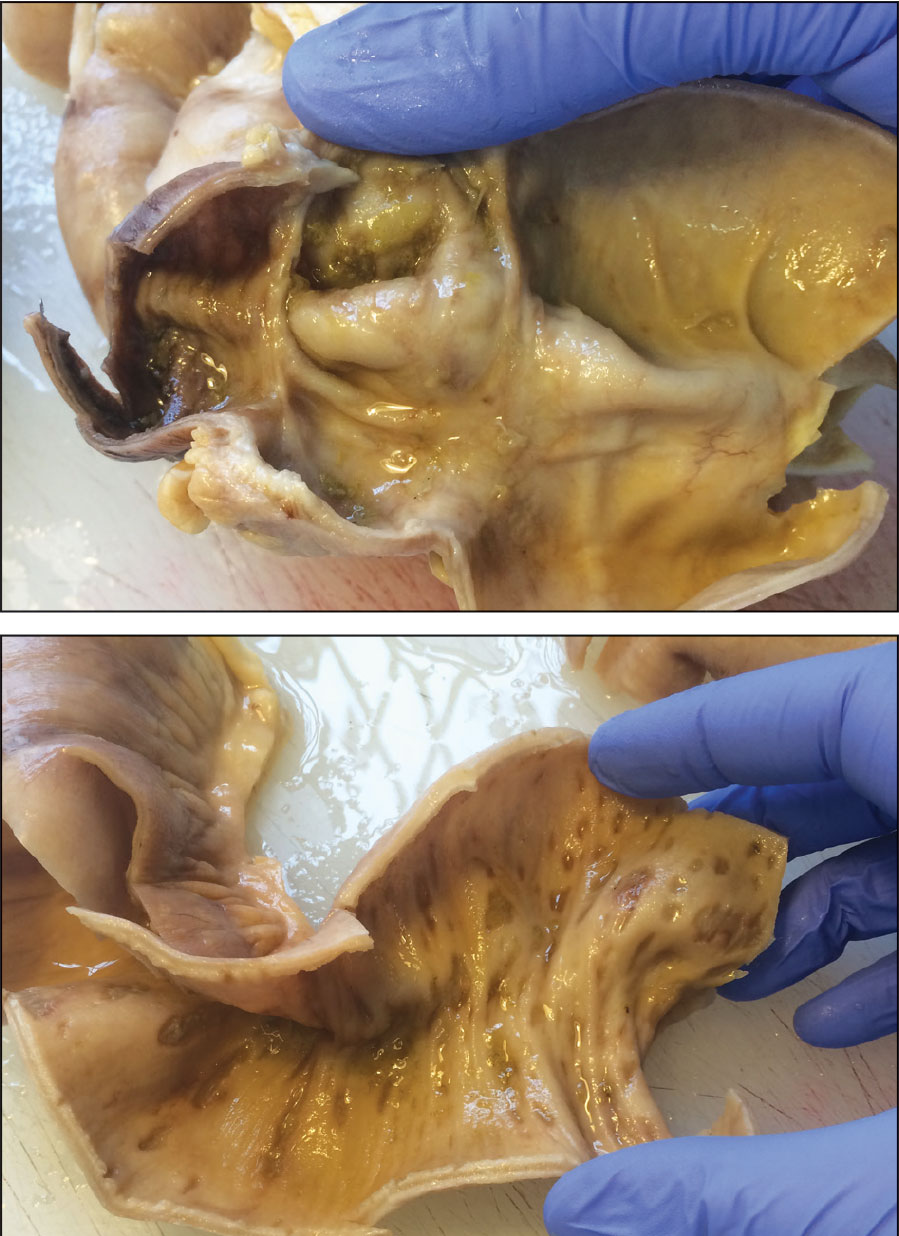
Figure 2. Small bowel with features of focal cobblestone, early stricture and patchy ulceration(click to enlarge)
Figure 3. Small bowel mucosa with fissuring ulcer, scarring and transmural inflammation(click to enlarge)
Discussion
In reference to European Crohn’s and Colitis Organisation (ECCO)1 statement 5E, extensive small bowel Crohn’s disease should be treated with systemic corticosteroids and thiopurines or methotrexate. For patients who relapsed, anti-TNF therapy with or without thiopurine is an appropriate option if there is objective evidence of moderate or severely active disease [EL5, RG D]. Surgical options should also be considered and discussed at an early stage. Indications for urgent surgery include perforation, uncontrolled haemorrhage, toxic megacolon, bowel obstruction and abscess. Elective surgery is considered in patients with stricture, fistula, malignancy, malnutrition, poorly controlled disease despite optimised medical management and extra-intestinal manifestation.2
Patients who have clinical features that suggest a poor prognosis currently appear to be the most suitable patients for early introduction of thiopurines, methotrexate and/or anti-TNF therapy (ECCO statement 5F1) [EL5 RG D]. The inflammatory burden is greater in extensive (> 100cm) than in localised small bowel disease involvement, often resulting in nutritional deficiencies. Early introduction of anti-TNF therapy should also be considered, especially in those who have clinical indicators of poor prognosis.
There are a few considered predictors of early post-operative recurrence after ileocolonic resection. These include patient-related risk factors such as smoking, disease-related risk factors such as prior intestinal surgery [EL 1 and RG A], penetrating disease behaviour, perianal location and surgery-related risk factors such as extensive small bowel resection (ECCO statement 8A1) [EL2b, RG B].
In recent ECCO guidelines,1 ileocolonoscopy is recommended within the first year after surgery where treatment decisions may be affected (statement 8C). Thiopurines are more effective than mesalazine or imidazole antibiotics alone in post-operative prophylaxis (statement 8F). The use of internationally recognised Rutgeerts’ score3 in post-operative endoscopic assessment is beneficial (i0 and i1 imply endoscopic remission while i2 - i4 imply recurrent endoscopic disease) (see Table 1 and Figure 4).
Absence of prophylactic treatment [EL1a, RG A] is associated with a higher risk of relapse. Prophylaxis is best started within two weeks of surgery, although an early start has not been proven superior to later treatment [EL5, RG D] (ECCO statement 8H1). The duration of prophylaxis should be at least two years [EL1a, RG B].
In a randomised, Post-Operative Crohn’s Endoscopic Recurrence (POCER) Trial,4 a study was conducted to evaluate a therapeutic strategy based on a risk stratification of patients, with further treatment step-up and adjustment if recurrence occurs on the basis of ileocolonoscopy. The study involved 17 centres from Australia and New Zealand with 174 patients who had intestinal resection enrolled. In the active care group, endoscopic recurrence was defined at six-month colonoscopy using the Rutgeerts’ score; if the score was ≥ i2, the treatment was stepped up to thiopurine, adalimumab every two weeks combined with thiopurine or weekly adalimumab.
Conclusion
Small bowel obstruction is one of the presentation complication features of Crohn’s colitis. Surgical treatment should not be viewed as a last resort or treatment failure but as part of the overall management plan. Post-operative prophylactic treatment is crucial to reduce recurrence risk. Ileocolonoscopy should be performed within six to 12 months after surgery to guide further management.
References
European Crohn’s and Colitis Organisation (ECCO) clinical practice guidelines 2016
Sachar DB. Indications for Surgery in Crohn’s Disease. The American Journal of Gastroenterology 102, S76–S78 (June 2007)
doi: 10.1111/j.1572-0241.2007.01307
Rutgeerts P, Geboes K, Vantrappen G et al. Gastroenterology 1990; 99: 956-983
De Cruz P, Kamm M, Hamilton AL et al. Crohn’s disease management after intestinal resection: a randomised trial. Post-Operative Crohn’s Endoscopic Recurrence (POCER) trial. The Lancet April 2015; 385(9976): 406-1, 417
 Figure 1. CT abdomen/pelvis shows distended loops of mid small bowel (SB) with a transition from distended SB to normally distended SB and a transition from normally distended sb to collapsed bowel more inferiorly. Findings consistent with small bowel obstruction(click to enlarge)
Figure 1. CT abdomen/pelvis shows distended loops of mid small bowel (SB) with a transition from distended SB to normally distended SB and a transition from normally distended sb to collapsed bowel more inferiorly. Findings consistent with small bowel obstruction(click to enlarge)