Commonly presenting bladder problems in general practice can have a significant economic burden on society while severely affecting patient health and quality of life
Dr Susmita Sarma, Consultant Obstetrician, University Hospital, Galway
Overactive bladder (OAB) is a highly prevalent and complex condition with a significant economic burden to society. Overactive bladder is defined as urinary urgency, usually accompanied by increased daytime frequency and/or nocturia, with urinary incontinence (UI) (OAB-wet) or without (OAB-dry), in the absence of urinary tract infection or other detectable disease.1
OAB prevalence rates in adults are between 12-14% in those aged over 18 years and 16.6% in adults over 40. The incidence of this condition in women increases with age up to 60, levels off between 60 and 70 and then increases again thereafter.2,3 It is estimated that there are 61-71 million adults living with OAB in Europe and 11-13 million living with chronic OAB with incontinence.
OAB is considered to be a hidden condition. Many patients find it difficult or embarrassing to talk about their condition with others. They often feel that it is normal in older women and don’t wish to bother their GP about it. It is under-reported for this reason. They are also unaware that there is treatment available for this condition.
OAB has a significant economic burden associated with it. From a personal and societal perspective, the costs are significant. These include direct costs such as diagnosis, treatment and continence containment, such as incontinence pads. There are also indirect costs such as lost wages by patients and caregivers and lost work productivity due to absenteeism. This does not include the cost of pain, suffering and decreased health-related quality of life.
The estimated total national cost of OAB with urgency urinary incontinence (UUI) in the US in 2007 was $65.9 billion with a projected cost of $82.6 billion in 2020.4 The cost of medication is considerable with an estimated €16.5 million spent in 2013. On average, 31,400 prescriptions are filled on the GMS scheme every month, with a further 4,200 filled on the Drugs Payments Scheme.5
When looking at quality of life in patients suffering from OAB, most studies found that there are significant effects on daily activities, mental health and sexual function, with 65% reporting that OAB adversely affected their quality of life.3
While isolated symptoms are rare, most studies report that the greater the number of symptoms, the greater the degree of bother from OAB. Generally, urgency alone doesn’t appear to cause as much distress as it does when accompanied by two or more symptoms.
The effect of nocturia is significant, with patients reporting even one episode of nocturia as bothersome. While it is generally felt that one episode of nocturia falls within the normal clinical spectrum, there is evidence that even any episode of nocturia can have a negative effect on quality of life, sleep, work performance and general wellbeing.3
The anatomy and physiology of the bladder are complex. Reduced activation of the sympathetic nervous system (SNS) results in relaxation of the detrusor muscle, closure of the sphincter, and bladder filling. When the volume of urine in the bladder reaches 200-400ml, the sensation of urge to void is relayed via the spinal cord to the brain centres. Voluntary voiding involves the parasympathetic nervous system and the voluntary somatic nervous system. Influences from these systems cause contractions of the detrusor muscle and corresponding somatic nervous activity, leading to sphincter relaxation and voiding. Interruption of these pathways leads to symptoms.
Aetiology and risk factors
There is a multiplicity of factors that contribute to the development of OAB symptoms. There are known age-related changes that occur in the bladder, affecting bladder contractility as well as increasing detrusor overactivity and decreasing urethral closure pressure. The genitourinary syndrome of menopause with resulting atrophy of urethral areas may contribute to symptoms of dryness, burning, itching, dyspareunia and infection as well as frequency and urgency. Other risk factors include difficult vaginal deliveries, high infant birth weight, previous hysterectomy and other pelvic surgery or radiotherapy. Smoking, high body mass index and constipation are all associated with increased risk of UI.6
Pathophysiological causes of urinary incontinence include lesions in higher micturition centres and may be associated with Parkinson’s disease, Alzheimer’s disease, cerebrovascular disease, diabetes, hypertension and obstructive sleep apnoea. In addition, issues with mobility and dexterity as well as reaction time can contribute to urinary incontinence.
Diagnosis and evaluation
Common reversible causes of urinary incontinence include urinary tract infection, constipation and medications. Patients with symptoms should undergo a complete medical evaluation to rule out reversible causes in the first instance. As a minimum, abdominal palpation to rule out gross abdominal or pelvic mass and inspection of external genitalia should be carried out.7
Women presenting for the first time should have a urine dipstick checked for blood, protein, glucose, leucocytes and nitrates and if positive a mid-stream sample should be sent to check for culture and analysis of antibiotic sensitivities.
If there are symptoms of voiding dysfunction or recurrent infections, an assessment of post-void residual should be made by bladder scan or catheterisation. Patients should be asked to complete a three-day bladder diary and given information on lifestyle changes they can make. The diary needs to record times and amounts of urine passed as well as leakage episodes, pads usage, fluid intake, degree of incontinence and urgency. It should cover both working and leisure days.
Women should be asked to reduce their caffeine intake. Bladder training should be offered for a minimum of six weeks. This can have better results if supervised by specialised physiotherapists or nurse continence advisors.8 If bladder training is not effective, then OAB medication may be offered.
Medications for OAB
There are several medications licensed for the treatment of OAB in Ireland. They include anticholinergics and antimuscarinics, which act by competitive antagonism of acetylcholine at postganglionic muscarinic receptors, causing relaxing of bladder smooth muscle. This in turn results in an increased bladder capacity and decreases urgency and frequency. Mirabegron is a beta3-agonist which activates beta adrenoceptors in the detrusor muscle and trigone area of the bladder, allowing urine storage by detrusor relaxation.
In general, there is no recommended first-line medication. The HSE Medicines Management Programme has tolterodine ER as first-line choice for treatment of OAB.5 However, the evidence for treatment for one medication over another has only shown modest differences.7,9 International guidelines do not identify one preferred medication.8 If the first medicine for OAB or mixed UI is not effective or well-tolerated, an alternative medication should be offered.
Transdermal OAB treatment can be useful in women unable to tolerate oral medications. Intravaginal oestrogen can be used to treat postmenopausal women with vaginal atrophy. Medication should be reviewed at four weeks to assess efficacy,4 although in clinical practice reviewing after 12 weeks of use is in keeping with clinical studies unless intolerable side-effects occur.
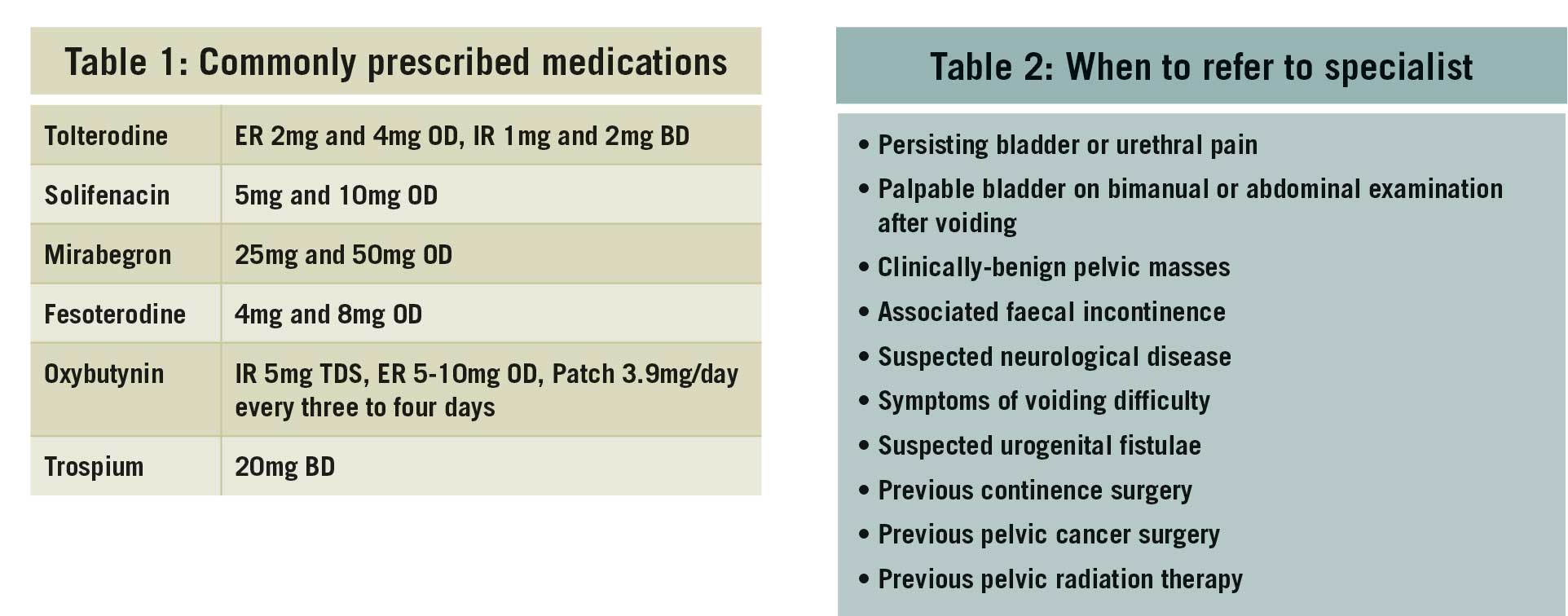
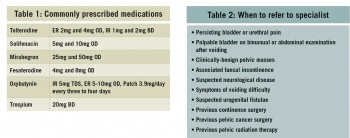
Typical antimuscarinic side-effects include dry mouth, constipation, blurred vision and drowsiness. Prolongation of the QT interval has occurred with tolterodine and caution should be used. Antimuscarinic drugs are contraindicated in myasthenia gravis, significant bladder outflow obstruction, severe ulcerative colitis, toxic megacolon and in gastrointestinal obstruction or atony. Mirabegron has reportedly less antimuscarinic side-effects but has reported tachycardia as a side-effect. See Table 1 for commonly prescribed medications. Flavoxate, propantheline and imipramine are rarely used.
Anticholinergic use in the elderly
The extent to which anticholinergics impair CNS function is proportional to their ability to cross the blood-brain barrier. It is of concern that up to 32% of the elderly use two or more drugs with anticholinergic effects.10
Oxybutynin, which is a lipophilic molecule with neutral polarity, is the one most likely to cross the blood-brain barrier. Despite this, it is still widely used to treat OAB in older patients because of the low cost. Tolterodine has low lipophilicity and is thought to be more suitable for older patients. Tolterodine IR and oxybutynin IR have a similar efficacy, but the former has fewer adverse effects in patients over 50 years of age. Trospium is the least likely to impair CNS function based on neuropsychological and co-ordination tests. Fesoterodine is also well tolerated in the elderly.11
Combination therapy
Combination therapy may be considered in patients who fail single medication use. Anti-muscarinic and beta3-adrenoceptor agonist medication may be used in combination if monotherapy with either alone fails.8
When to refer to a specialist
Patients who do not respond to conservative treatment, lifestyle changes and medication or if they meet the criteria in Table 2 should be referred for specialist review.
(click to enlarge)
The role of urodynamic studies
In patients who do not respond to treatment, urodynamic assessment may offer further information regarding their diagnosis. Urodynamic assessments include a variety of measures that evaluate urine flow, including flow rate, post-void residual urine, filling cystometry, bladder pressure and urethral pressure. Detrusor overactivity may be confirmed at urodynamics which can help direct more invasive treatment for OAB. Urodynamic studies should not be offered as first-line investigation but only after conservative treatment and medication has failed to achieve the desired result in uncomplicated OAB.
Invasive treatments for OAB
Botulinum toxin type A injection can be offered to women who fail medical treatment.7 The risks and benefits of treatment need to be explained to the women along with the likelihood of complete or partial symptom relief and the possibility of voiding dysfunction and increased risk of urinary tract infection. This should only be offered if the woman is willing in the event of developing a significant voiding dysfunction to either perform clean intermittent catheterisation or accept a temporary indwelling catheter. There is no data on long-term side-effects of botox treatment. Treatment needs to be repeated when symptoms reoccur.
PTNS has been shown to be useful in the treatment of OAB but is not widely available. It is an alternative, less invasive method of neuromodulation, which is therefore considerably cheaper. There are fewer published high-quality data supporting the use of PTNS and so it should only be offered after a multidisciplinary team review in women who have failed conservative therapy, including anticholinergic drug treatment, and who do not want botulinum toxin treatment or SNS.
The mode of action of PTNS is unclear. The posterior tibial nerve contains mixed sensory motor fibres and emerges from the same spinal segments as the sacral nerve. Neuromodulation of the sacral nerve plexus via the posterior tibial nerve is thought to produce the effects on bladder symptoms.
Percutaneous sacral nerve stimulation is believed to work by electrically stimulating the sacral nerves which carry signals between the pelvic floor and the brain. The latest version of sacral neuromodulation allows a patient to operate a hand-held programmer to adjust therapy to achieve optimal outcome. Women need to be aware of the need for surgery, for test stimulation and the risk of failure, long-term commitment, the need for surgical revision and adverse effects.
For some patients, their OAB symptoms can be refractory to all the treatments outlined above. For these patients the treatment options are limited to major surgical procedures or long-term catheterisation. A detailed consideration of these is beyond the scope of this article, but after appropriate multidisciplinary review and detailed counselling, severely affected patients may be offered urinary diversion into an ileostomy or clam ileo-cystoplasty. Both are major and complex surgical procedures with significant short- and long-term morbidity and mortality (approximately 1% postoperative mortality rate).
Long-term indwelling urinary catheterisation is often overlooked as a simple and effective means of restoring continence. Complications do occur but these are usually symptomatic urinary tract infection and catheter-related complications, including encrustation and bypassing. However, for some patients an indwelling catheter (either urethral or suprapubic) can be an acceptable long-term solution.
Interstitial cystitis/bladder pain syndrome
Interstitial cystitis/bladder pain syndrome (IC/BPS) is defined as an unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder, associated with lower urinary tract symptoms of more than six weeks duration, in the absence of infection or other identifiable causes.12
Women between the ages of 40 and 60 years are most commonly affected. The condition occurs far more frequently in Caucasians and there is a 9:1 female predominance.13
Up to 50% of women experience spontaneous remissions unrelated to treatment, with a duration ranging from 1-80 months. Reported prevalence rates for this condition vary widely as there is no universally accepted definition. The pathophysiology of interstitial cystitis remains elusive and many theories have been formulated.
Pain typically occurs in the pelvic area and can manifest in the bladder, vagina, urethra, rectum or perineum. It can be sharp in nature but there can also be feelings of pressure or burning. It can also be related to sexual intercourse.
Diagnosis
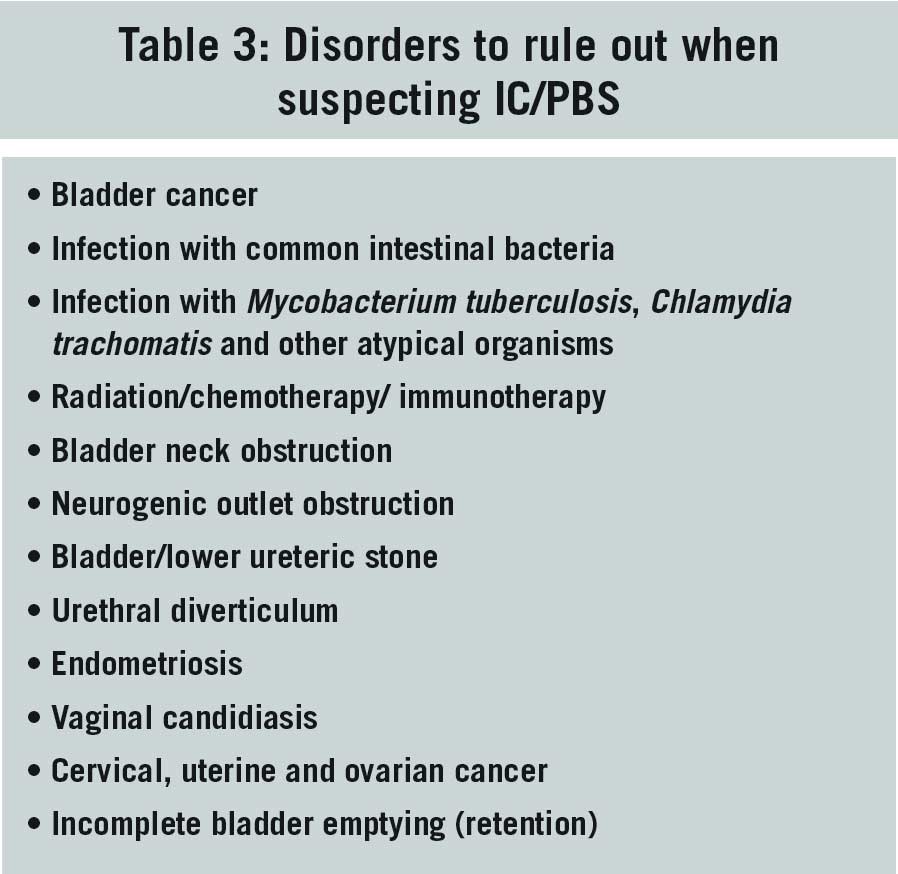
Basic assessment should include a careful history, physical examination and urinalysis to rule in symptoms that characterise IC/PBS and rule out other disorders (see Table 3).
(click to enlarge)
Baseline voiding symptoms using a frequency volume chart and measurement of post-void residuals as well as pain levels should be obtained in order to measure subsequent effects. Cystoscopy and/or urodynamics should only be considered as an aid to diagnosis in uncomplicated presentations.1
Management
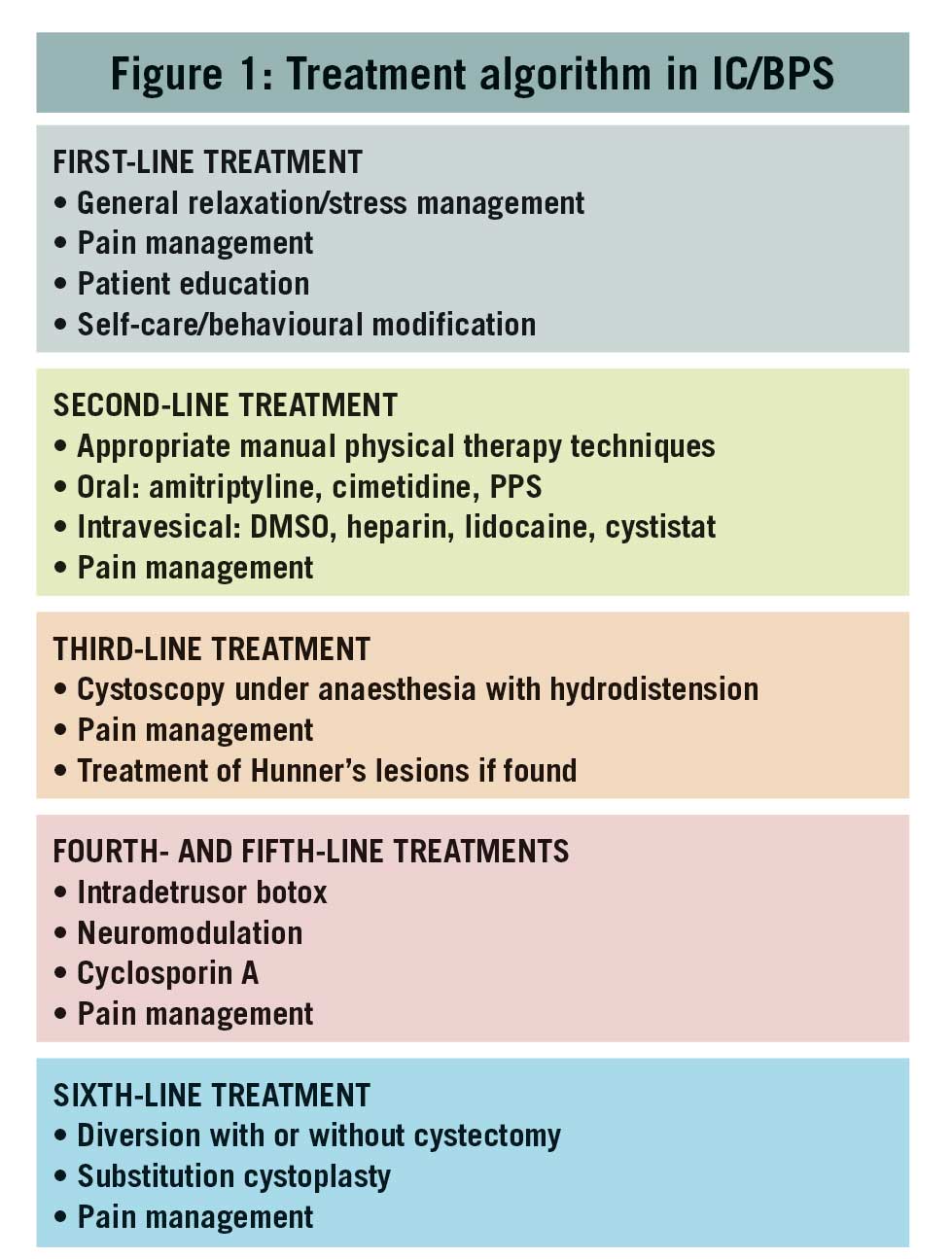
Conservative treatment is first-line management. Patients should be educated about normal bladder function and what is known and not known about IC/BPS, the benefits and risks of treatment, that no single treatment has been found to be suitable for all patients and that multiple approaches may be required to achieve symptom control.1See Figure 1.
(click to enlarge)
Initial treatment should depend on symptom severity as well as patient preference and clinical judgement. Ineffective treatments should be stopped after a reasonable period. Pain management should be continuously assessed because of its importance to quality of life. The ICS/BPS diagnosis should be reconsidered if no improvement occurs after a period of time.
Antihistamines have been shown to be useful for the symptomatic treatment of IC/BPS, possibly by preventing the release of histamines that can cause inflammation. An improvement should be seen within six to eight weeks of continuous use.
Amitriptyline is frequently used in pain management. Its safety and efficacy in women with interstitial cystitis showed significant change in the symptom score and improvement of pain and urgency intensity when compared with placebo.14
When to refer to a specialist
When medication has failed in a primary setting the following may then be considered:
Hyaluronic acid (Cystistat) temporarily replaces the deficient glycosaminoglycan (GAG) layer on the bladder wall, helping to relieve the pain, frequency and urgency of interstitial cystitis. For the first four weeks of treatment, women with interstitial cystitis receive one instillation each week. After that, treatments are usually given once a month until the symptoms resolve. Five or six instillations can be necessary before symptoms begin to resolve. Treatment can be repeated if symptoms return
Cystoscopy with hydrodistension is the most commonly performed intervention in women with IC/BPS. Hydrodistension is thought to work by disrupting the neuronal pathways of the bladder, thereby disrupting pain transmission. Treatment efficiency ranges from 12-70%. The benefits are, however, short-lived and it can cause ischaemia, damage and even bladder rupture.
Reconstructive surgery is considered where other treatments have failed, and symptom severity is such that the woman’s quality of life is seriously affected. Surgery is invasive and irreversible and there is no guarantee that the symptoms will improve. Some can, in fact, become worse. Potential complications from surgical procedures also need to be considered. Options available include partial cystectomy, augmentation cystoplasty and urinary diversion with or without cystectomy.
Recurrent urinary tract infections in women
Recurrent urinary tract infection (UTI) refers to ≥ 2 infections in six months or ≥ 3 infections in one year. UTI recurrences are typically acute simple cystitis rather than complicated UTI. Most recurrences are thought to represent reinfection rather than relapse, although occasionally a persistent focus can produce relapsing infection.
Approximately 60% of women will experience symptomatic acute bacterial cystitis in their lifetime; 20-40% of these will experience a further episode and 25-50% will experience multiple episodes.15 Women with an uncomplicated UTI have no known risk factors that would make them more susceptible to developing a UTI. Women with complicated UTI have higher risk for developing a UTI and a greater chance of not responding to treatment. These risk factors include anatomic or functioning abnormality of the urinary tract such as stones or diverticulum, suffering from an immunocompromised condition or infection by a multidrug resistant organism. UTI usually refers to culture-proven acute bacterial cystitis. Women are predisposed to developing UTIs due to a short urethra. Intercourse assists bacteria in ascending into the bladder. Constipation also increases the likelihood of developing UTIs.
Symptoms
In young women, an acute UTI usually presents with dysuria associated with urinary urgency, frequency and sometimes suprapubic pain, haematuria or worsening incontinence. Acute dysuria is a highly specific symptom with 90% accuracy for UTI.16 In older women, symptoms of UTI may be less clear but acute dysuria as well as the above symptoms remain reliable for diagnosis.
Diagnosis
For a diagnosis of a UTI, there should be symptoms plus laboratory culture of a urinary pathogen. The most common bacteria is E coli (75-97%) followed by Enterobacteriaceae, P mirabilis, K pneumoniae and S saprophyticus.
The definition of clinically significant bacteria was described more than 60 years ago and was based on an arbitrary cut-off aimed at reducing overtreatment of asymptomatic patients. The cut-off of 105 colony-forming units (CFU)/ml may not identify women who are symptomatic of a UTI. In women who are symptomatic, studies have shown that they may culture bacteria as low as 102CFU/ml.17 Hence, clinical symptoms in the absence of laboratory-proven culture is enough to warrant treatment for UTI in women.
In women with recurrent UTIs, a complete history and pelvic exam should be carried out. Repeat samples may need to be taken and consideration for the need to obtain a catheter sample should be given. Asymptomatic bacteriuria, which is the presence of bacteria in the urine in the absence of symptoms or illness, does not need to be treated in women with no other risk factors.
General advice to women with recurrent UTIs
Women should be advised to wipe from front to back to avoid introducing bacteria into the urethra. They are also advised not to hold onto urine for more than three to four hours and to empty directly after sexual intercourse and avoid getting dehydrated.18 Some women may find it useful to avoid taking baths, using cotton underwear and keeping underwear off at nighttime.
Antibiotic treatment
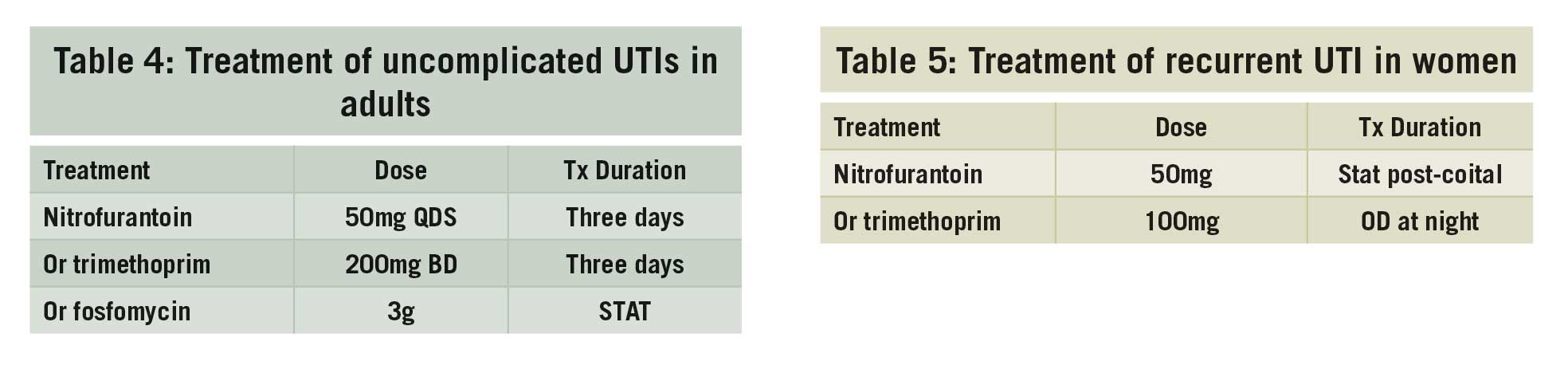
The choice of antibiotic use depends on local sensitivities. The HSE guidelines for treatment for acute uncomplicated UTIs in adults are shown in Table 4.
From a clinical perspective, doctors may offer patient-initiated treatment to select women while awaiting culture sensitivities. After discussion of the risks and benefits, doctors may prescribe antibiotic prophylaxis to decrease the risk of future UTIs in women of all ages previously diagnosed with UTIs (see Table 5).16
(click to enlarge)
Although the evidence is not robust, some women find cranberry prophylaxis useful in the management of recurrent UTIs. There is sufficient evidence to recommend vaginal oestrogen, topical or tablet form to peri- and post-menopausal women with recurrent UTIs where there is no contraindication to oestrogen therapy.15
When to refer to a specialist
Specialist referral is recommended where complicated UTIs occur as mentioned above. Cystoscopy and upper tract imaging should not be routinely carried out in uncomplicated patients but may be necessary in those with a higher index of suspicion of abnormalities. Women who are initially treated for an uncomplicated UTI who recur rapidly such as within two weeks, may also require imaging or cystoscopy.
Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn, 2010,29:4-20; International Urogynecology J, 2010; 21: 5-26
Irwin DE, Milsom I, Hunskaar S, et al. Population-based survey of urinary incontinence, overactive bladder and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006; 50(6): 1306-1315
Milsom I, Abrams P, Cardozo L, Roberts RG, Thüroff J, Wein AJ. How widespread are the symptoms of an overactive bladder and how are they managed? A population based prevalence study. BJU Int. 2001; 87(9): 760-766
Coyne KS, Wein A, Nicholson S, Kvasz M, Chen CI, Milsom I. Economic burden of urgency urinary incontinence in the United States: a systematic review. J Manag Care Pharm. 2014; 20(2): 130-40
Medicines Management Programme: Oral Medicines for the Management of Urinary Incontinence, Frequency & Overactive Bladder 17th October 2014. Accessible on https://www.hse.ie/eng/services/publications/clinical-strategy-and-programmes/oral-medicines-for-the-management-of-urinary-incontinence-frequency-overactive-bladder.pdf
Danforth KN, Townsend MK, Lifford K, et al. Risk factors for urinary incontinence among middle-aged women. Am J Obstet Gynecol. 2006; 194(2): 339-345
NICE guideline on Urinary Incontinence in Women 2015. Accessible on https://www.nice.org.uk/guidance/cg171
Diagnosis and Treatment of Non-Neurogenic Overactive Bladder (OAB) in Adults:an AUA/SUFU Guideline (2019)
Thuroff JW et al. EAU Guidelines on Urinary Incontinence. European Urology 2011; 59:387-400 (updated March 2013)
Kay GG, Granville LJ. Antimuscarinic agents: implications and concerns in the management of overactive bladder in the elderly. Clin Ther 2005; 27: 127-38
Wagg A, Khullar V, Marschall-Kehrel D, Michel MC, Oelke M, Darekar A, Bitoun CE, Weinstein D, Osterloh I. Flexible-dose fesoterodine in elderly adults with overactive bladder: results of the randomized, double-blind, placebo-controlled study of fesoterodine in an aging population trial. J Am Geriatr Soc. 2013; 61(2): 185-93
Diagnosis and Treatment Interstitial Cystitis/Bladder Pain Syndrome (2014). American Urological Association Guideline
Parsons M, Toozs-Hobson P. The investigation and management of interstitial cystitis. J Br Menopause Soc 2005; 11: 132-9
van Ophoven A, Pokupic S, Heinecke A, Hertle L. A prospective, randomized, placebo controlled, double-blind study of amitriptyline for the treatment of interstitial cystitis. J Urol 2004; 172: 533-6
Recurrent Uncomplicated Urinary Tract Infection in Women: AUA/CUA/SUFU Guideline (2019)
Hooton TM: Clinical practice. Uncomplicated urinary tract infections. N Engl J Med 2012; 366: 1028
Hooton TM, Roberts PL, Vox ME et al: Voided midstream urine culture and acute cystitis in premenopausal women. N Engl J Med 2013; 369: 1883
NICE Guideline on Urinary Tract Infections. Accessible at https://www.nice.org.uk/guidance/ng112
 (click to enlarge)
(click to enlarge)