A rare case of osteomyelitis due to topical tacrolimus abuse
This case report outlines where long-term and persistent use of topical tacrolimus for eczema in conjunction with persistent pruritus led to skin abrasion and a cascade of reaction
Atopic eczema is a chronic relapsing skin condition that affects 2-10% of adults. The presentation of this condition in adults is often severe and chronic. Steroids are the firstline of treatment. Topical tacrolimus belongs to a class of new immunomodulators, which is a class of immunosuppressant drugs that work by reducing inflammation through suppression of T-lymphocytes.
It is recommended as a secondline treatment for moderate to severe atopic eczema. Topical tacrolimus has mainly localised side effects. This case report brings to light a rare adverse effect of extensive and unmonitored use of topical tacrolimus in a steroid refractory atopic eczema.
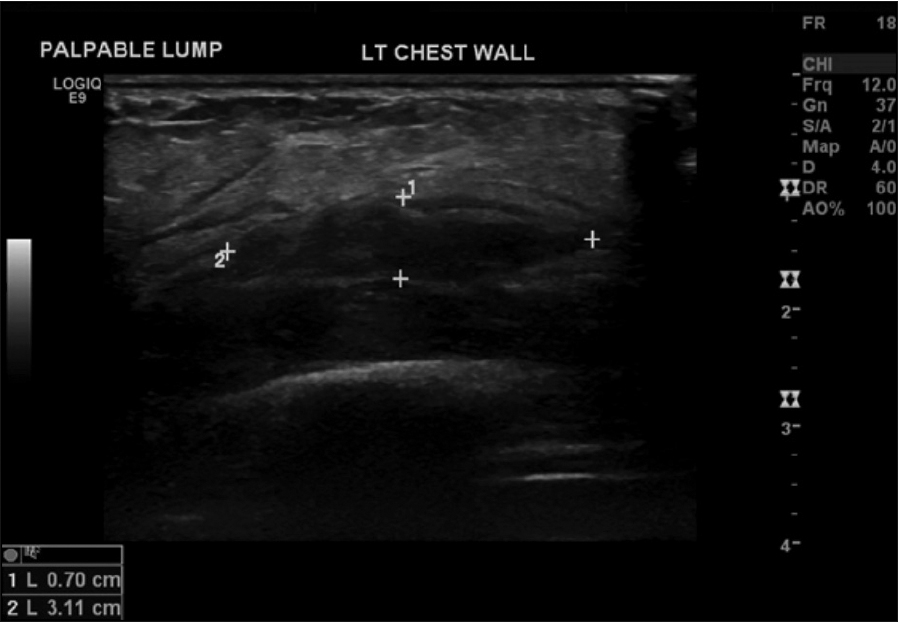
Figure 1: Ultrasound of anterior chest wall – hypoechoic complex fluid collection in the left chest wall(click to enlarge)
Figure 2: CT thorax – low attenuating lesion in overlying anterior ribs/costochondral areas 5 to 7 with associated intercostal muscle thickening(click to enlarge)
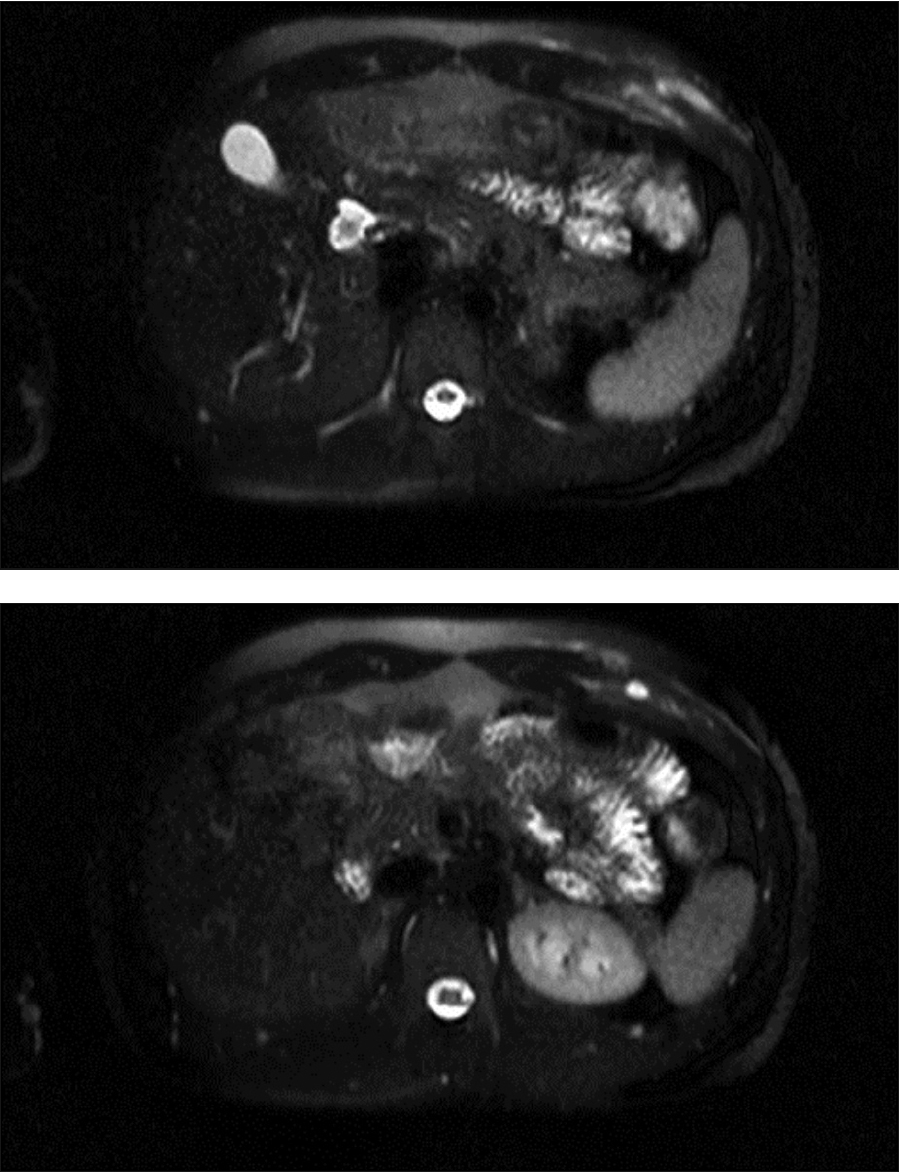
Figure 3: MRI post contrast – small intramuscular fluid collection that demonstrates rim enhancement. There is diffuse periosteal enhancement of the sixth rib. The appearance is suggestive of infectious process with an intramuscular abscess and associated osteomyelitis anterior rib(click to enlarge)
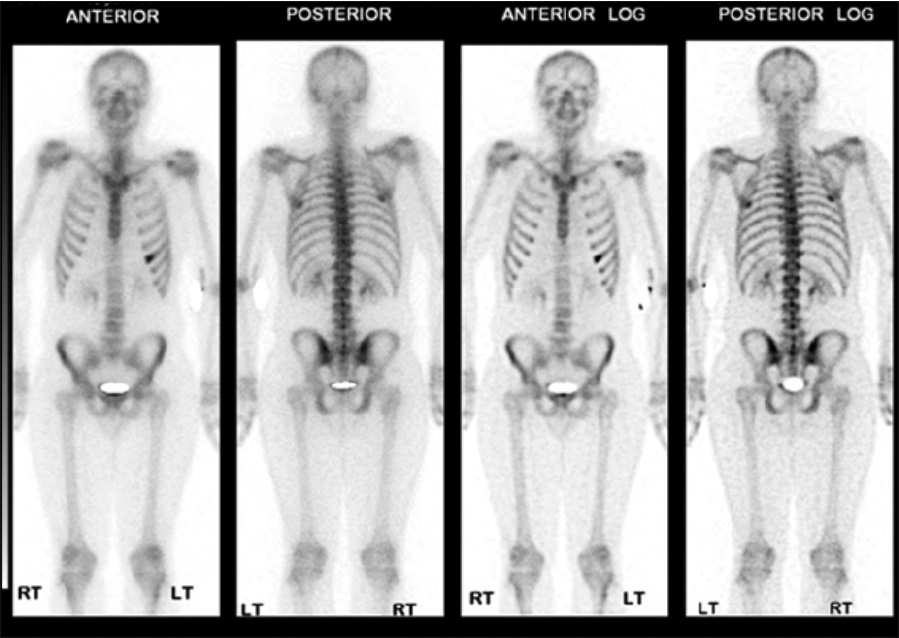
Figure 4: Nuclear imaging of whole body scan – radioisotope uptake of the sixth rip on anterior view(click to enlarge)
Case report
A 21-year-old Caucasian male presented to the emergency department with left lower chest pain. The pain was localised, severe in intensity and exacerbated on movement and deep inspiration. The patient also reported difficulty in sleeping and was unable to cope with pain.
A week prior to presentation, he had a course of antibiotics for flu-like symptoms prescribed by his GP. He had a history of asthma and atopic eczema, for which he was attending a dermatologist. His medications included hydroxyzine, fexofenadine, fluticasone/salmeterol inhaler, albuterol inhaler and tacrolimus 0.1% topical.
On examination the patient was pyrexic and had widespread, atopic, eczematous lesions. An oval shaped tender subcutaneous skin swelling was noted on the left lower chest overlying the sixth rib anteriorly. Minor visible skin abrasions were also noted as a mark or scratch. The rest of his physical examination was unremarkable.
On investigations inflammatory markers were raised. Ultrasound of the affected side of the chest wall showed a 4cm soft tissue lesion with heterogeneous echotexture and decreased Doppler signal, suggesting further evaluation with CT (Figure 1).
A CT evaluation showed a low attenuating lesion overlying the anterior fifth-seventh ribs associated with intercostal muscle thickening (Figure 2), which may represent resolving haematoma or abscess formation.
After a week’s course of antibiotic therapy, the patient continued to spike temperature and repeat ultrasonography showed no change.
Work up for endocarditis and abscess elsewhere was unremarkable. An ultrasound-guided needle aspiration of the swelling was inconclusive. An MRI thorax was arranged and showed periosteal enhancement of the sixth anterior rib, suggestive of infectious process (osteomyelitis) with an intramuscular abscess (Figure 3). The findings were reconfirmed by a whole body isotope scan with no other hot spot (Figure 4). The patient was treated for osteomyelitis for six weeks as per hospital guidelines. The patient responded clinically and biochemically.
Discussion
Atopic eczema is a chronic, pruritic inflammatory skin disease with clinical features of skin dryness, erythema, oozing and crusting, and lichenification. Pruritus is a hallmark of the condition. Staphylococcus aureus colonisation is common and causes secondary infection, especially in skin lesions refractory to conventional therapy.
Topical tacrolimus (calcineurin inhibitors) reduce immunological response to antigens through its inhibitory effect on cytokine production and alteration in epidermal antigen presenting dendritic cells. The long-term safety of this agent is unknown.
In our case, persistent and long-term use of this medication for eczema in conjunction with persistent pruritus led to skin abrasion, which in itself led to a cascade of reaction. It did this by creating an easy pathway for microbes to penetrate the skin down to the soft tissues and bone, leading to abscess and bone infection in the background and a localised immune response modulation.
The Irish Medicines Board recommends that treatment should not be continued on a long term basis and where this use is deemed necessary it has issued advice for health professionals. It may be worth checking the serum level of tacrolimus if drug abuse is suspected.
References
Ashcroft DM, Dimmock P, Garside R, Stein K, Williams HC. Efficacy and tolerability of topical pimecrolimus and tacrolimus in the treatment of atopic dermatitis: meta-analysis of randomised controlled trials. BMJ 2005; 330(7490):516
NICE guidelines
Berbari EF, Steckelberg JM, Osmon DR. Osteomyelitis. In: Principles and Practice of Infectious Diseases, 6, Mandell GL et al (eds) (Ed), Elsevier, Philadelphia 2005: 1322
Furue M1, Terao H, Moroi Y et al. Dosage and adverse effects of topical tacrolimus and steroids in daily management of atopic dermatitis. Dermatol 2004; 31(4):277-83
Irish Medicines Board. Topical tacrolimus (Protopic) – Important recommendations for appropriate use to minimise risks. Drug Safety Newsletter; 2012 (June); 48:1-2
 Figure 1: Ultrasound of anterior chest wall – hypoechoic complex fluid collection in the left chest wall(click to enlarge)
Figure 1: Ultrasound of anterior chest wall – hypoechoic complex fluid collection in the left chest wall(click to enlarge)