Innovations in the management of age-related macular degeneration
Advances in treatment and monitoring indicate an optimistic future in the management of ARMD
Dr Yvonne Delaney, Dean of Postgraduate Education, Irish College of Ophthalmologists, Dublin and Dr Melissa Murphy, Higher Medical Ophthalmology Trainee, Royal Victoria Eye and Ear Hospital, Dublin
Age-related macular degeneration (ARMD) is the leading cause of vision loss in Ireland, accounting for 25% of all cases on the national blind register.1 Risk factors for developing ARMD include family history, current smokers and Caucasian race,2 but the greatest risk factor by some margin is increasing age. In Ireland, disease prevalence rises dramatically from 5% in those aged 50-64 years, to 7.8% in the 65-74 age group and 13.2% in those aged ≥ 74.3 Due to its aging population, the disease burden in Ireland will continue to increase significantly in the next decade. Advances in disease prevention, monitoring as well as treatments are urgently sought to mitigate against the present and future burden of ARMD on Ireland’s healthcare system.
(click to enlarge)
Dry macular degeneration with multiple yellow spots of drusen
Symptoms and classification
The main symptoms of ARMD are reduction in central vision and/or metamorphopsia, which is distortion of vision with straight lines appearing wavy or curvy. Central vision is key to performing everyday activities such as reading, watching TV and driving, so patients are usually aware of the change to their visual function.
ARMD can be classified into early, intermediate and advanced stages; the advanced stage is further divided into ‘dry’ (non-exudative, no neovascularisation) and ‘wet’ (exudative, neovascular-type) forms of the disease. Impairment of vision primarily only occurs in advanced stages and therefore a key focus of management is the detection of disease in the early stages in order to slow progression.
Dry macular degeneration
This form of the disease is characterised by drusen which form beneath the retinal pigment epithelium. Drusen are deposits consisting of proteins and lipids, which can become calcified over time. Although drusen can be associated with normal ageing, an increased number or larger ‘soft’ drusen are indicative of ARMD (see Figure 1). It is important to note that patients with drusen will generally be asymptomatic until the late stages of disease, at which point distortions to central vision start to manifest. In the later stages of dry macular degeneration, geographic atrophy (heterogeneous retinal thinning) occurs and can be seen on clinical examination, fundal photography and other imaging.
Current treatment for dry macular degeneration
The mainstay of treatment for dry ARMD involves modifying risk factors for disease progression; these include smoking cessation and vitamin supplementation. Smoking cessation should be encouraged especially in those with a family history, as quitting current smoking can still be beneficial with the relative risk of ARMD approximately halved in ex-smokers.4
Vitamin supplementation is also effective in slowing down the natural history of the disease. The Age Related Eye Diseases Studies (AREDS) trial reported that daily oral vitamin supplementation in at-risk patients (at the intermediate stage) could achieve a 25% reduction in the risk of developing advanced ARMD over a five-year period.5 The exact blend of supplements given was further refined during the AREDS2 trial,6 resulting in the current recommendation: lutein, zeaxanthin, vitamins C and E, as well as the minerals copper and zinc.
A second pillar of management is close monitoring of disease progression by means of serial optical coherence tomography (OCT) scans taken at regular appointments with a specialist. However, this aspect brings significant strain to resources in the healthcare system as well as being inconvenient for patients who are generally older, may have limited mobility and often have to travel significant distances to attend appointments.
Equally important is patient education and self-monitoring as, if patients themselves can identify deterioration in their vision, they can seek help at the most appropriate time. A key tool in this regard is the use of the Amsler grid to monitor for acute changes in vision: this simple tool is a set of vertical and horizontal lines printed onto a card. Patients can look at the grid on a weekly basis, testing each eye at a time. If any lines appear newly distorted this can indicate deterioration, often due to conversion from dry to wet macular degeneration and prompt the patient to seek specialist care more urgently.
Innovations in dry macular degeneration
ARMD is a complex and multifactorial disease with several factors including inflammatory and complement pathways contributing to its pathogenesis. Recent research has focused on the complement pathway with two promising complement inhibitors showing early success in clinical trials.7
One such promising new treatment is pegcetacoplan, a pegylated peptide molecule binds to C3 and C3b complement proteins, inhibiting downstream inflammatory effects. The FILLY phase II trial in 2020 demonstrated significant reductions in growth of geographic atrophy (GA) in patients treated with monthly intravitreal pegcetacoplan compared to those receiving a sham treatment.8 Two subsequent phase III studies, DERBY and OAKS, are ongoing to further investigate the efficacy and safety of this novel treatment, with interim data showing promising results.9
Another drug showing potential is avacincaptad pegol, which is an anti-C5 aptamer designed to decrease the activation of inflammasomes. In a phase III, randomised controlled trial (GATHER 1) patients achieved a statistically significant 28% reduction in the mean rate of GA growth at 18 months compared with the sham group.10 A second confirmatory phase III trial is underway (GATHER 2).
Wet macular degeneration
An estimated 10% of patients with advanced ARMD suffer from the wet form of the disease. In 2017, this translated into a prevalence of over 7,000 patients in Ireland suffering from the disease.11 Wet ARMD is associated with considerably worse visual outcomes than dry ARMD. The hallmark of the disease is choroidal neovascularisation (CNV), characterised by abnormal, new, friable vessels which penetrate the retinal layers from the choroid. CNV leads to a reduction in vision due to these leaking vessels causing intra-retinal fluid and haemorrhage with potential scar formation if left untreated. Traditionally no effective treatments existed for wet ARMD until 2010, when anti-vascular endothelial growth factor (anti-VEGF) agents were introduced. These agents offered a paradigm shift in the treatment of CNV, offering a vast improvement in visual prognosis and now constitute the gold standard of treatment for wet ARMD. OCT and fundus fluorescein angiography (FFA) also play an important role for diagnosis and monitoring of disease progression respectively, with imaging forming an important role in treatment decisions.
(click to enlarge)
Current treatment for wet ARMD or CNV:Intra-vitreal injection performed under local anaesthetic with anti-VEGF have become the gold standard treatment for wet ARMD.
Current treatment for wet macular degeneration
Current treatment for wet ARMD or CNV is serial anti-VEGF injections (see Figure 2), with bevacizumab the most commonly administered agent in Ireland. Once diagnosed, patients receive monthly injections of bevacizumab for a minimum of three months (the loading phase). Regular monitoring and further injections follow, with the interval for further injections tailored depending on response to treatment and disease severity, known as a ‘treat and extend’ protocol. This protocol involves a step-wise increase in the interval between injections up to a maximum interval of 12 weeks provided that the patient remains stable at each follow-up visit. Despite these increased injection intervals, the TREX-AMD study showed that patients still required an average of 10.1 injections in their first year.12 Therefore even with a ‘treat and extend’ protocol, regular visits are required for treatment and/or imaging. A meta-analysis of real-world data clearly shows that patients attending for fewer than the recommended follow-up visits and injections achieve poor visual outcomes.13 This highlights the urgent need for new agents with increased efficacy and longer duration of action to decrease the burden on both the patient and the healthcare system.
Innovations in wet macular degeneration
Research has been focused on two key areas: first, the development of novel agents which are effective for longer and can be administered at greater time intervals; and second, design of novel port-delivery systems (PDS) which can be implanted into the eye, enabling slow release of a drug without the need for repeat injections. Both innovations will translate into fewer injections per year, advantageously reducing the known complications associated with intravitreal injection; these are rare but serious and include cataract formation, vitreous haemorrhage or, in the most serious case, endophthalmitis (with a rate of occurrence of < 0.04%).14
Novel drug treatment
Brolucizumab is a humanised monoclonal single-chain variable fragment (scFv) that binds and inhibits vascular endothelial growth factor A. This novel anti-VEGF agent can be applied with a treatment interval of 12 weeks following the loading phase. The HAWK and HARRIER trials15 showed not only that brolucizumab was non-inferior to a standard treatment, but also that more patients could be maintained on a 12-week dosing schedule (ie. showed no increase in disease activity requiring an interval reduction). Brolucizumab-related inflammatory events have been reported, including rare but serious retinal vasculitis and further studies are required to evaluate its safety in the real world.
Another new treatment on the near horizon is faricimab, a bispecific antibody targeting two distinct pathways, both VEGF-A and angiopoietin-2 (a further cytokine implicated in the pathogenesis of wet ARMD). TENAYA and LUCERNE were phase III trials which demonstrated that faricimab could be administered at 16-week intervals with sustained efficacy, further reducing the treatment burden,16 even as compared to brolucizumab.
New port delivery systems
The development of PDS represents a true innovation in the treatment of wet ARMD. A PDS is a drug reservoir that is surgically implanted into the eye which can be refilled as required, potentially allowing for up to 15 months of drug delivery into the eye between refills, as evidenced by the phase II clinical trial LADDER.17 A treatment group receiving the first PDS refill at 15 months achieved similar visual outcomes as a control group receiving monthly intravitreal injections. In the subsequent ARCHWAY trial, comparing a PDS-treated cohort with patients receiving four-weekly intravitreal injections of ranibizumab, 98.4% of PDS-treated patients required no supplemental ranibizumab treatment before the first refill at 24 weeks;18 90% of PDS-treated patients also reported a preference for the PDS treatment (despite still attending for monthly follow-up visits) demonstrating both the efficacy of this new system and a reduced burden for patients.18
Imaging in ARMD
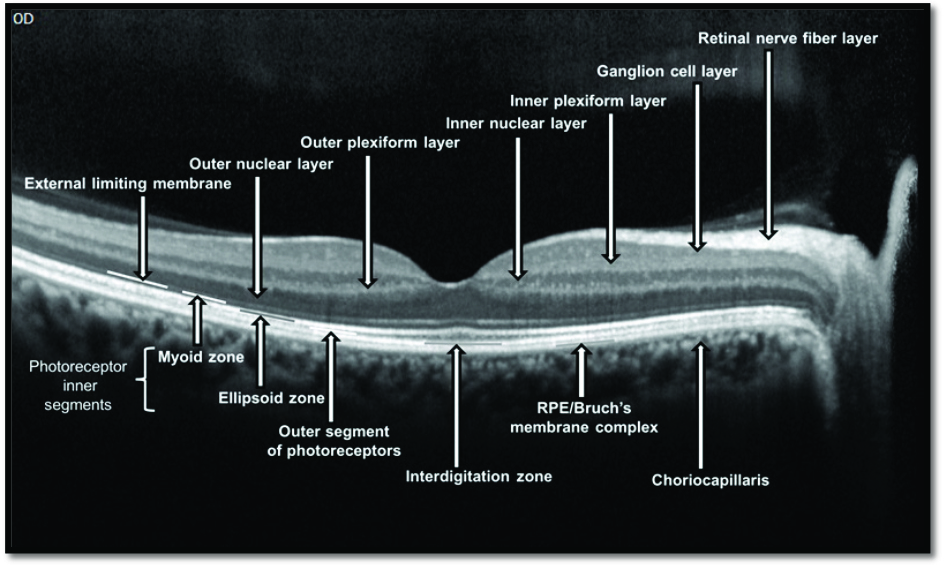
The primary imaging modalities used in both diagnosis and follow-up of ARMD are OCT and FFA. OCT is a non-invasive technique which allows for visualisation of the macula in high-resolution cross-sectional images. One drawback is that traditional OCT is of very limited use for imaging vessels at the back of the eye, posing a problem for detecting CNV in wet ARMD. By contrast, FFA and a related modality, indocyanine green angiography (ICGA), are highly effective at detecting vessels and fluid leakage at the back of the eye, which are critical for diagnosing wet ARMD. There are two major disadvantages to these techniques, in that they are invasive, requiring insertion of a needle into the patient’s arm, and they carry the risk associated with a contrast dye injection, including, although rare, anaphylaxis.
(click to enlarge)
‘In vivo’ retinal biopsy: OCT with resolution of 2-3ums demonstrating detailed retinal anatomy but with limited ability to image retinal vasculature.
(click to enlarge)
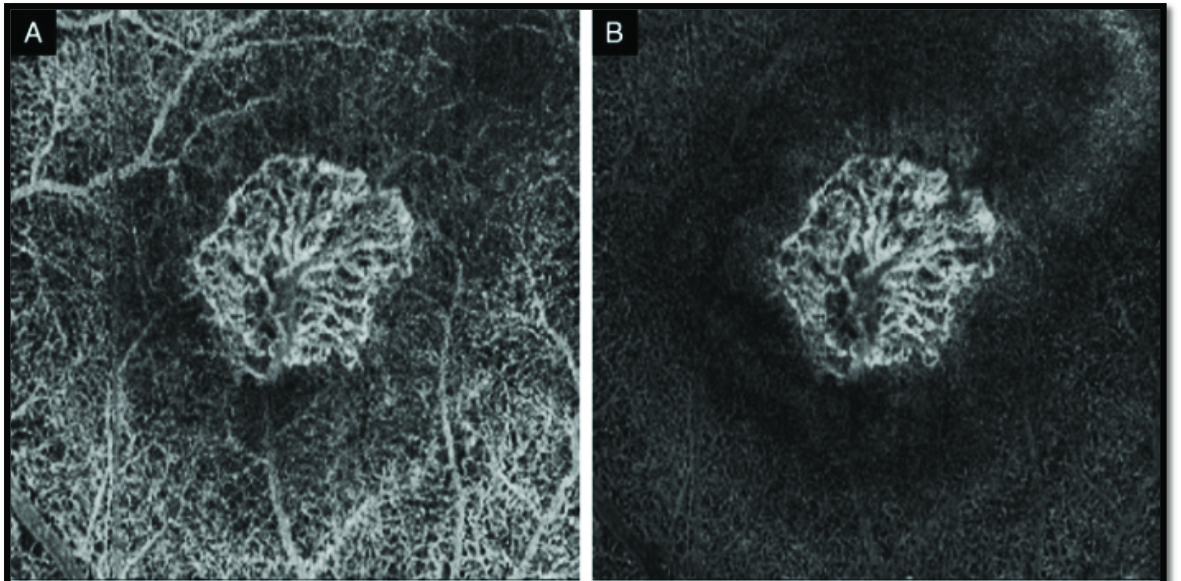
A. OCT angiogram of a type 2 CNV with projection artefact. B. Same lesion with projection artifact removal.
Innovations in imaging
The new modality of OCT-angiography (OCT-A) offers a non-invasive technique capable of producing high-resolution images of both the retinal and choroidal vasculature). No intravenous contrast dye is required, and imaging quality with OCT-A is superior to FFA in many aspects, including:
Higher resolution for outlining retinal vasculature19
Images not obscured due to hyper-fluorescence following contrast leakage.20
Furthermore, standard OCT images are recorded simultaneously during OCT-A, such that OCT-A sequences can be directly mapped onto OCT imaging.
Although one obstacle to the use of OCT-A is a steep learning curve (to be expected with any new modality), its use is rapidly expanding for both diagnosis and follow-up of wet ARMD. Compared to FFA, it is faster to perform and does not require a nurse for catheter insertion, representing a reduced burden on limited resources in Ireland’s healthcare system.
Innovations in care pathway design
Before the introduction of anti-VEGF treatments, traditional ARMD eye-care involved in-person consultations following a simple one-two-three sequence of arrival, exam and further review or discharge. Currently, overwhelmed by the numbers of injections as well as the demands of frequent best-practice multi-modal retinal imaging, more innovative ways to deliver eye care must be explored.
Teleophthalmology
Teleophthalmology is defined as the use of digital means and information sharing to provide eye care from a distance. Innovations in both software and hardware including electronic medical records (EMRs) combined with powerful communication technologies have given rise to a variety of teleophthalmology models showing various degrees of success in screening, triage and decision support for different ocular conditions.21
The specialty of ophthalmology is fortunate that both the retina and associated vasculature lend themselves particularly well to imaging. Retinal imaging has transformed in the past 20 years from analogue two-dimensional photographs to wide-field three-dimensional digitised images with resolution of 2ums, capable of showing the retinal layers as per an in vivo biopsy. Equally important is the capturing of these digital images and their transmission using secure networked platforms. Enabling remote viewing has opened up new opportunities for the delivery of eye care and proven to be a strong catalyst for the emergence of virtual or remote retinal clinics.
Remote or virtual retinal clinics with diagnostic hubs
Virtual retinal clinics have been emerging in Ireland and in the UK in recent years, with their development further encouraged by the Covid-19 pandemic. The most common model is the asynchronous hybrid model where patients attend for testing and imaging but do not have a face to face consultation with the ophthalmologist. Technicians and/or nurses see the patients and perform the necessary clinical and imaging tests, the results of which are inserted into the EMR. The updated EMR, with the retinal images, is uploaded and, via a shared network, are available for remote, synchronous or asynchronous viewing by the clinician. Appropriate management and diagnosis is determined by the clinician and communicated to the patient and to the patient’s GP or physician. Using this model, the Moorfields Medical Retina Virtual Assessment Study Group in London has shown, with 1,006 patients seen over six weeks, both an improved patient experience but also improved efficiencies with a reduction in the overall waiting time as well as the patient journey time.22
Home monitoring and artificial intelligence (AI)
The ultimate goal for the future of ARMD care would be that the patient may not have to attend in person at all for the necessary visual monitoring and retinal imaging.
New in-home monitoring devices and mobile medical software applications offer practical tools for early detection of changes to visual function, signalling potential disease progression. FDA approved downloadable apps include myVisiontrack (Vital art and Science/Genentech) and Alleye (Oculocare Medical), both of which are designed to detect metamorphopsia, with ophthalmologists able to remotely view the patient’s test results and decide on the necessity and urgency of further review.23
An even more substantial breakthrough is the emergence of in-home OCT imaging devices. Although not yet approved by the FDA, Notal Vision’s home-based OCT imaging device showed promising correlation with in-office OCT for detecting the presence of retinal fluid, an important biomarker in wet AMD, with > 95% agreement.24 However, at-home OCT cannot be widely adopted without the ability to filter the large amount of images generated into actionable information. Yim et al have already shown that in the setting of in-hospital OCT imaging, AI-based analysis of images for detecting progression of ARMD is equal to retinal specialists.25 Kim et al have taken this a step further with AI-based analysis of at-home OCT images. Using a novel deep learning AI algorithm (Notal OCT Analyzer) that was developed to detect and quantify retinal fluid overtime, Kim et al confirmed a high correlation of over 97% between patient self-acquired scans using the AI algorithm and expert-graded commercial OCT scans.26 The potential for AI and home monitoring devices for the future appears bright.
Conclusion
ARMD represents the single most important threat to vision in Ireland’s population over a lifetime. The future looks optimistic with innovations across the board in terms of treatments, monitoring as well as innovative ways of accessing care with diagnostic hubs, in-home monitoring and the introduction of technologies augmented with AI to optimise diagnostic accuracy and accessibility.
References
Kelliher C. Trends in blind registration in the adult population of the Republic of Ireland 1996-2003. Br J Ophthalmol 2006; 90(3):367-371. DOI: 10.1136/bjo.2005.075861
Chakravarthy U, Wong TY, Fletcher A et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol 2010; 10:31. DOI: 10.1186/1471-2415-10-31
Akuffo KO, Nolan J, Stack J et al. Prevalence of age-related macular degeneration in the Republic of Ireland. Br J Ophthalmol 2015; 99(8):1037-44. DOI: 10.1136/bjophthalmol-2014-305768
The Age-Related Eye Disease Study (AREDS) Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol 2001; 119(10):1417-36. DOI: 10.1001/archopht.119.10.1417
The Age-Related Eye Disease 2 (AREDS2) Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. Jama 2013; 309(19):2005-15. DOI: 10.1001/jama.2013.4997
Cabral De Guimaraes TA, Daich Varela M, Georgiou M, Michaelides M. Treatments for dry age-related macular degeneration: therapeutic avenues, clinical trials and future directions. Br J Ophthalmol 2022; 106(3):297-304. DOI: 10.1136/bjophthalmol-2020-318452
Liao DS, Grossi FV, El Mehdi D et al. Complement C3 inhibitor pegcetacoplan for geographic atrophy secondary to age-related macular degeneration. Ophthalmology 2020; 127(2):186-95. DOI: 10.1016/j.ophtha.2019.07.011
Kaiser E. DERBY and OAKS: 18-month data shows continuous reduction in foveal, extrafoveal lesion growth in eyes with GA. Modern Retina 2022, May 12
Jaffe GJ, Westby K, Csaky KG et al. C5 Inhibitor avacincaptad pegol for geographic atrophy due to age-related macular degeneration. Ophthalmology 2021; 128(4):576-86. DOI: 10.1016/j.ophtha.2020.08.027
HSE. Pimary Care: Eye Services Review Group Report 2017. www.hse.ie/eng/services/publications
Wykoff CC, Croft DE, Brown DM et al. Prospective Trial of Treat-and-Extend versus Monthly Dosing for Neovascular Age-Related Macular Degeneration: TREX-AMD 1-Year Results. Ophthalmology 2015; 122(12):2514-22. DOI: 10.1016/j.ophtha.2015.08.009
Kim LN, Mehta H, Barthelmes D, Nguyen V, Gillies MC. Meta-analysis of real-world outcomes of intravitreal ranibizumab for the treatment of neovascular age-related macular degeneration. Retina 2016; 36(8):1418-31. DOI: 10.1097/iae.0000000000001142
Forooghian F, Albiani DA, Kirker AW, Merkur AB. Comparison of endophthalmitis rates following intravitreal injection of compounded bevacizumab, ranibizumab, and aflibercept. Can J Ophthalmol 2017; 52(6):616-9. DOI: 10.1016/j.jcjo.2017.04.016
Dugel PU, Koh A, Ogura Y et al. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2020; 127(1):72-84. DOI: 10.1016/j.ophtha.2019.04.017
Heier JS, Khanani AM, Quezada Ruiz C et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet 2022;399(10326):729-40. DOI: 10.1016/s0140-6736(22)00010-1
Campochiaro PA, Marcus DM, Awh CC et al. The Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2019; 126(8):1141-54. DOI: 10.1016/j.ophtha.2019.03.036
Holekamp NM, Campochiaro PA, Chang MA et al. Archway Randomized Phase 3 Trial of the Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2022; 129(3):295-307. DOI: 10.1016/j.ophtha.2021.09.016
Perrott-Reynolds R, Cann R, Cronbach N et al. The diagnostic accuracy of OCT angiography in naive and treated neovascular age-related macular degeneration: a review. Eye 2019;33(2):274-282. DOI: 10.1038/s41433-018-0229-6
Spaide RF, Fujimoto JG, Waheed NK, Sadda SR, Staurenghi G. Optical coherence tomography angiography. Progress in Retinal and Eye Research 2018; 64:1-55. DOI: https://doi.org/10.1016/j.preteyeres.2017.11.003
Sommer AC, Blumenthal EZ. Telemedicine in ophthalmology in view of the emerging COVID-19 outbreak. Graefes Arch Clin Exp Ophthalmol 2020; 258(11):2341-52. DOI: 10.1007/s00417-020-04879-2
Hanumunthadu D, Adan K, Tinkler K et al. Outcomes following implementation of a high-volume medical retina virtual clinic utilising a diagnostic hub during Covid-19. Eye 2022; 36(3):627-33. DOI: 10.1038/s41433-021-01510-4
Faes L, Bachmann LM, Sim DA. Home monitoring as a useful extension of modern tele-ophthalmology. Eye 2020; 34(11):1950-3. DOI: 10.1038/s41433-020-0964-3
Kim JE, Tomkins-Netzer O, Elman MJ et al. Evaluation of a self-imaging SD-OCT system designed for remote home monitoring. BMC Ophthalmol 2022; 22(1):261. DOI: 10.1186/s12886-022-02458-z
Yim J, Chopra R, Spitz T et al. Predicting conversion to wet age-related macular degeneration using deep learning. Nat Med 2020; 26(6):892-9. DOI: 10.1038/s41591-020-0867-7
Lally D, Kim JE, Elman MJ et al. Performance of a novel deep learning algorithm for Automatic Retinal Fluid Quantification in Home OCT Images. Invest Ophthalmol Vis Sci 2020; 61(7):2571
 (click to enlarge)
(click to enlarge)